

Abstract
Background
We performed a meta-analysis to evaluate the effect of anti–tumor necrosis factor (TNF) therapy on the frequency of extra–articular manifestations (EAMs) in patients with ankylosing spondylitis (AS).
Methods
We searched with the terms ‘ankylosing spondylitis’, ‘infliximab’, ‘etanercept’, ‘adalimumab’, ‘golimumab’, ‘certolizumab’, ‘TNF inhibitor/blocker/antagonists’ or ‘anti-TNF’ on MEDLINE, EMBASE and Cochrane Library for randomized controlled trials (RCTs) of ≥12 weeks with parallel or crossover design of TNF inhibitor versus placebo to treat uveitis, inflammatory bowel disease (IBD) and/or psoriasis of AS, published before February 2014.
Results
We found 8 RCTs that fit our criteria. Anti–TNF therapy was associated with less uveitis than placebo in patients with AS (OR: 0.35, 95% CI: 0.15–0.81, P = 0.01). Subgroup analysis showed receptor fusion proteins were more efficacious for uveitis than placebo (OR: 0.30, 95% CI: 0.09–0.94, P = 0.04), but monoclonal antibodies were not (OR: 0.43, 95% CI: 0.12–1.49, P = 0.18). Anti–TNF therapy and placebo group did not significantly differ in treating IBD in AS patients (OR: 0.75, 95% CI: 0.25–2.29, P = 0.61). In subgroup analysis, neither monoclonal antibodies (OR: 0.45, 95% CI: 0.10–1.92, P = 0.28) nor receptor fusion proteins (OR: 1.52, 95% CI: 0.25–9.25, P = 0.65) significantly differed from placebo in treating IBD. We found no suitable reports on psoriasis.
Conclusions
Anti–TNF therapy was preventive for flares or new onset of uveitis in AS patients, and might be an alternative for these patients. However, monoclonal anti–TNF antibodies and TNF receptor fusion proteins were not efficacious for IBD in AS patients.
Keywords: Ankylosing spondylitis, Anti-TNF therapy, Extra–articular manifestations, Uveitis, Inflammatory bowel disease, Meta–analysis
Background
Ankylosing spondylitis (AS) is a chronic, progressive, inflammatory rheumatic disease that primarily affects the sacroiliac joints [1]. AS is primarily a disease of the axial skeleton, but some patients have peripheral joint involvement [2]. AS also has some extra–articular manifestations (EAMs). An epidemiological study in Belgium found that 42% of patients with definite AS had one or more EAMs [3]. EAMs mostly occurred in the eye (uveitis), gastrointestinal tract (inflammatory bowel disease, IBD) and skin (psoriasis) [4].
Uveitis, which is characterized by pain with red eye and photophobia, increased tear production and blurring of vision [5], occurs in approximately 20–30% of AS patients during the course of their disease, and is considered the most common EAM [6,7]. Non–steroidal anti–inflammatory drugs (NSAIDs) can only relieve uveitis symptoms for a short period in AS patients, but cannot change the course of their disease or prevent structural damage. NSAIDs treatment can also increase the tendency towards osteoporosis if used for a longer period of time. Some evidence indicates that disease–modifying anti–rheumatic drugs (DMARDs) can reduce uveitis recurrence [8,9]. TNF is present at high concentrations in both aqueous humor and serum of patients with uveitis [10], and may participate actively in the pathogenesis of uveitis. In recent years, several trials have demonstrated the efficacy of anti–TNF therapy in reducing acute uveitis [11,12].
IBD is characterized by a chronic inflammation of the gut mucosa and includes Crohn’s disease (CD) and ulcerative colitis (UC). A recent systematic review and meta-analysis showed the pooled prevalence of IBD in patients with AS to be 6.8% [7]. Traditionally, treatment of IBD has relied on corticosteroids to reduce flares and on immunomodulators to maintain remission [13]. Aminosalicylic acid is widely used to treat UC, but its use in CD is controversial [14]. Several recent trials have demonstrated the efficacy of anti-TNF therapy in reducing IBD [15].
Psoriasis is a systemic inflammatory cutaneous disease with plaque lesions and nail deformities. The pooled prevalence of psoriasis, a secondary disorder in AS, was 9.3% in patients with AS [7].
In a 2010 update by the Assessments in Ankylosing Spondylitis International Society and the European League against Rheumatism (ASAS/EULAR) of recommendations for the management of AS [16], NSAIDs are considered the first-line drug treatment for AS patients with pain and stiffness; DMARDs and intra–articular injections of glucocorticoids in patients with peripheral arthritis may also be considered, although there is no evidence to support the use of these medications for axial diseases; anti-TNF therapy is another option for patients with persistently high disease activity despite conventional treatments.
Infliximab (INF) is a chimeric mouse–human monoclonal immunoglobulin G (IgG) 1 antibody [17]. Adalimumab (ADA) [18], golimumab (GOL) [18] and certolizumab (CZP) [19] are humanized monoclonal anti-TNF-α antibodies. Etanercept (ETA) [20] is a dimeric fusion protein of the TNF receptor linked to the Fc portion of human IgG1.
Additionally, trials of anti–TNF therapy in AS have yielded impressive results [21-25] and a recent systematic review and meta–analysis [26] described the benefits of anti–TNF therapy in patients with AS. However, only a small trial has reported on the efficacy of anti–TNF therapy for EAMs of AS [11], and further meta–analysis could strengthen this evidence. Therefore, we performed a meta–analysis of randomized clinical trials (RCTs) to provide an up–to–date and comprehensive picture of the clinical efficacy of anti–TNF therapy for the most common EAMs in patients with AS—uveitis, IBD and psoriasis.
Methods
We captured all relevant studies published before February 2014 on MEDLINE, EMBASE and the Cochrane Library using following search terms: ‘ankylosing spondylitis’, ‘infliximab’, ‘etanercept’, ‘adalimumab’, ‘golimumab’, ‘certolizumab’, ‘TNF inhibitor/blocker/antagonists’ or ‘anti-TNF’.
Studies included in this meta-analysis met the following criteria: they were RCTs; their duration of study was ≥12 weeks; they used a parallel or crossover design of TNF inhibitor versus placebo treatment; and their data included information on uveitis, IBD and psoriasis in patients with AS.
Two independent investigators determined the relevance of the cited articles by reading the abstracts. Disagreements were resolved through discussion and consensus or, as needed, with consensus with a third investigator. When there were multiple articles from the same trial, the most complete and recently reported data were included.
Evaluations of methodological quality and risk of bias were performed independently by two reviewers, and disagreements between the two were resolved by consensus. Methodological quality of included articles was further assessed using modified Jadad criteria with an 8-item scale designed to assess randomization, blinding, withdrawals and dropouts, inclusion and exclusion criteria, adverse effects and statistical analysis [27]. Score range was from 0 (lowest quality) to 8 (highest quality). Scores of 4–8 denoted good to excellent (high quality) and 0–3 poor or low quality. Risk of bias was assessed according to the recommendations of the Cochrane Collaboration, classified as having either a low, high or unclear risk of bias [28,29]. Assessment of risk of bias in the included studies was based on sequence generation, allocation concealment, blinding (of participants, personnel and outcome assessors), incomplete outcome data, selective outcome reporting and other sources of bias, such as baseline imbalance and early stopping bias.
The statistical analysis was performed using Review Manager 5.2 (The Nordic Cochrane Centre, Copenhagen, Denmark) from the Cochrane Collaboration, 2013. Categorical dichotomous variables were assessed using the odds ratio (OR). P <0.05 was considered to be statistically significant; 95% confidence intervals (CI) were reported. Homogeneity was tested using the Q statistic (significance level at P < 0.10) and the I2 statistic (significance level at I2 > 50%) [30]. A random-effects model was used if the Q or I2 statistic was significant. Otherwise, a fixed-effects model was used. The existence of a publication bias for the meta-analysis was examined using a funnel plot. To assess the potential confounding effect of heterogeneity, subgroup analyses were performed. According to TNF-inhibitor classification, we divided those into two subgroups of TNF receptor fusion proteins (ETA) and monoclonal anti-TNF antibodies (INF, AND, GOL and CZP).
Results
A total of 1,395 relevant articles were retrieved from various databases of which 801 were excluded after scanning the titles; 521 after carefully reading the abstracts; and an additional 65 articles for various reasons (duplicates, not RCT or no required data; Figure 1). Finally, 8 RCTs were retained for meta-analysis [31-38]. Overall, included studies were of adequate methodological quality (mean modified Jadad score 6.875 for included studies, and all 8 studies had a score ≥6). Included studies, basic characteristics of enrolled patients and details about drug therapy are presented in Table 1.
Figure 1.
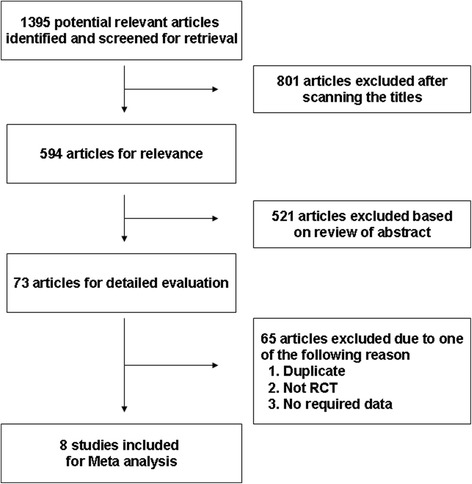
Flow chart demonstrating the process of study selection.
Table 1.
Basic characteristics of included studies
| Study | No. of patients | Age (years) | Male patients N (%) | Duration of AS (years) | Study Duration (weeks) | Medications allowed during the study | Modified Jadad Score | Risk of bias | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sequence generation | Allocation concealment | blinding | Incomplete outcome data | Selective outcome reporting | other sources of bias | ||||||||
| ADA | |||||||||||||
| van der Heijde D. 2006 [31] | 315 | 24 | DMARDs, NSAIDs and glucocorticoids | 6 | ? | ? | √ | √ | √ | √ | |||
| ADA 40 mg every 2 weeks | 208 | 41.7 ± 11.69 | 157 (75.5) | 11.3 ± 9.99 | |||||||||
| Placebo | 107 | 43.4 ± 11.32 | 79 (73.8) | 10.0 ± 8.34 | |||||||||
| ETA | |||||||||||||
| Brandt J. 2003 [32] | 30 | 24 | NSAIDs | 8 | √ | √ | √ | √ | √ | √ | |||
| ETA 25 mg twice weekly | 14 | 38.9 ± 9.1 | 10 (71.4) | 14.9 ± 8.3 | |||||||||
| Placebo | 16 | 32.0 ± 7.5 | 12 (75) | 11.4 ± 8.8 | |||||||||
| Davis JC Jr. 2003 [33] | 277 | 24 | DMARDs, NSAIDs and glucocorticoids | 6 | ? | ? | √ | √ | √ | √ | |||
| ETA 25 mg twice weekly | 138 | 42.1 (24–70) | 105 (76) | 10.1 (0–30.7) | |||||||||
| Placebo | 139 | 41.9 (18–65) | 105 (76) | 10.5 (0–35.3) | |||||||||
| van der Heijde D. 2006 [34] | 356 | 12 | DMARDs, NSAIDs and glucocorticoids | 6 | ? | ? | √ | √ | √ | √ | |||
| ETA 25 mg twice weekly | 150 | 39.8 ± 10.7 | 114 (76) | 10.0 ± 9.1 | |||||||||
| ETA 50 mg weekly | 155 | 41.5 ± 11.0 | 109 (70) | 9.0 ± 8.7 | |||||||||
| Placebo | 51 | 40.1 ± 10.9 | 40 (78) | 8.5 ± 6.8 | |||||||||
| IFX | |||||||||||||
| Braun J. 2002 [35] | 69 | 12 | NSAIDs | 8 | √ | √ | √ | √ | √ | √ | |||
| IFX 5 mg/Kg | 34 | 40.6 ± 8.0 | 23 (68) | 16.4 ± 8.3 | |||||||||
| Placebo | 35 | 39.0 ± 9.1 | 22 (63) | 14.9 ± 9.3 | |||||||||
| Marzo-Ortega H. 2005 [36] | 42 | 30 | NSAIDs, oral corticosteroids | 8 | √ | √ | √ | √ | √ | √ | |||
| IFX 5 mg/Kg + MTX | 28 | 41 (28–74) | 23 (82.14) | 8 (0–41) | |||||||||
| Placebo + MTX | 14 | 39 (30–56) | 11 (78.57) | 10 (0–35) | |||||||||
| GOL | |||||||||||||
| Inman RD. 2008 [37] | 356 | 24 | NSAIDs, MTX, SSA, HCQ, corticosteroids | 7 | ? | ? | √ | √ | √ | √ | |||
| GOL 50 mg | 138 | 38 (29–46) | 102 (73.8) | 5.15 (1.60–11.60) | |||||||||
| GOL 100 mg | 140 | 38 (30–47) | 98 (70.0) | 5.20 (1.50–13.25) | |||||||||
| Placebo | 78 | 41 (31–50) | 55 (70.5) | 7.25 (2.80–18.60) | |||||||||
| CZP | |||||||||||||
| Landewé R. 2014 [38] | 325 | 24 | DMARDs, NSAIDs, MTX, SSA | 6 | ? | ? | √ | √ | √ | √ | |||
| CZP 200 mg every 2 weeks | 111 | 39.1 ± 11.9 | 67 (60.4) | 6.9 (0.3–34.2) | |||||||||
| CZP 400 mg every 4 weeks | 107 | 39.8 ± 11.3 | 68 (63.6) | 7.9 (0.3–44.8) | |||||||||
| Placebo | 107 | 39.9 ± 12.4 | 65 (60.7) | 7.7 (0.3–50.9) | |||||||||
ADA = adalimumab; ETA = etanercept; IFX = infliximab; GOL = golimumab; CZP: certolizumab; MTX = methotrexate; DMARDs = disease-modifying antirheumatic drugs; NSAIDs = non-steroidal anti-inflammatory drugs; SSA = sulfasalazine; HCQ = hydroxychloroquine; √, low risk of bias; ?, unclear risk of bias.
The pooled analysis included 1,770 patients (1,223 randomized to anti-TNF therapy and 547 to placebo). Six trials [32-36,38] reported on uveitis that occurred in 7 patients in the anti-TNF therapy group and 16 in the placebo group; 5 trials [31,33,34,37,38] reported on IBD that occurred in 5 patients in the anti-TNF therapy group and 4 in the placebo group. No included trial reported on psoriasis.
Anti-TNF therapy was associated with less uveitis than placebo in patients with AS (OR: 0.35, 95% CI: 0.15–0.81, P = 0.01, Figure 2). Subgroup analysis for uveitis in patients with AS showed TNF receptor fusion proteins to be more efficacious than placebo (OR: 0.30, 95% CI: 0.09–0.94, P = 0.04); whereas monoclonal anti-TNF antibodies did not significant differ from placebo (OR: 0.43, 95% CI: 0.12–1.49, P = 0.18). Analysis for IBD in these patients found that the anti-TNF therapy and placebo did not significantly differ (OR: 0.75, 95% CI: 0.25–0.29, P = 0.61, Figure 3); and neither monoclonal anti-TNF antibodies (OR: 0.45, 95% CI: 0.10–1.92, P = 0.28 versus placebo) or receptor fusion proteins (OR: 1.52, 95% CI: 0.25–9.25, P = 0.65 versus placebo) significantly differed from placebo. Funnel plot analysis showed symmetry, which indicates that publication bias was not a significant factor in these studies (Figures 4 and 5).
Figure 2.
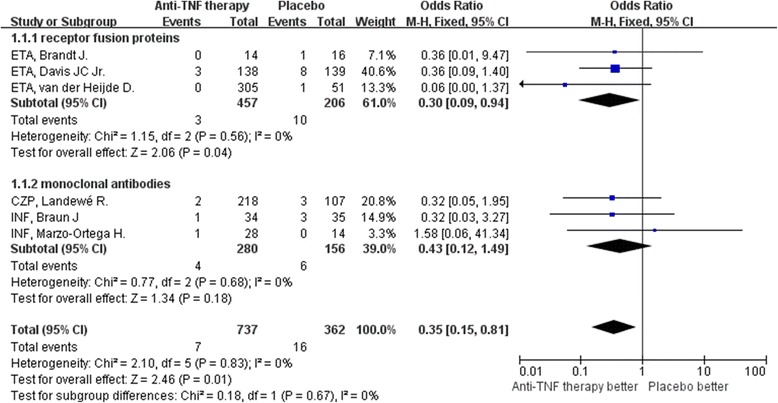
Meta-analysis of uveitis between anti-TNF therapy and placebo for ankylosing spondylitis.
Figure 3.
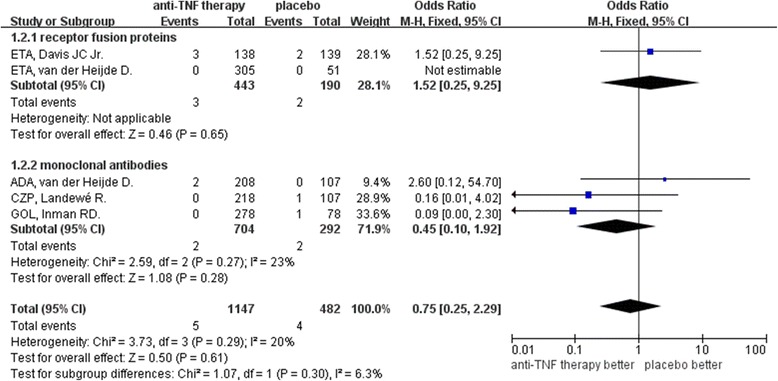
Meta-analysis of inflammatory bowel disease between anti-TNF therapy and placebo for ankylosing spondylitis.
Figure 4.
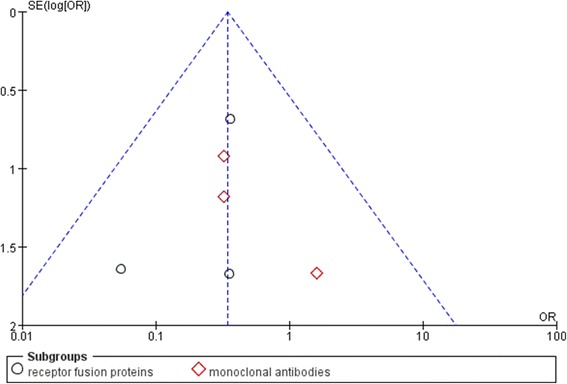
Funnel plot of included trials that reported uveitis.
Figure 5.
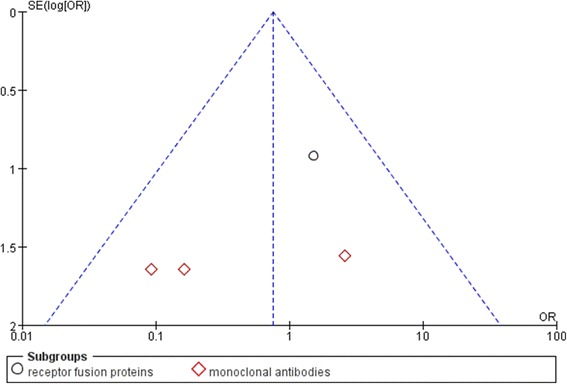
Funnel plot of included trials that reported inflammatory bowel diseases.
Analysis of risk of bias showed that only 3 trials reported their methods of sequence generation and allocation concealment in detail [32,35,36]. Blinding was performed properly in all included trials. All trials were free from incomplete outcome data and free from selective outcome reporting as well as other sources of bias. All 8 included trials had low or moderate risk of bias (Table 1).
Discussion
This meta-analysis compared anti-TNF therapy with placebo in patients with AS. The results indicate significant positive benefits of anti-TNF agents to treat uveitis in these patients. For IBD treatment outcomes, the anti-TNF therapy group and the placebo group did not significantly differ. However, Subgroup analysis showed the receptor fusion protein ETA was more efficacious than placebo for uveitis in this patient population, whereas monoclonal anti-TNF antibodies were not. Neither monoclonal antibodies nor receptor fusion proteins significantly differed from placebo in treating IBD.
Anti-TNF therapy has been shown to be beneficial for the treatment of uveitis in patients with AS. A retrospective study [39] of patients with spondyloarthropathy further confirms the efficacy of anti-TNF therapy in reducing acute uveitis flares. Therefore, all available data imply that ETA would not be as effective as monoclonal anti-TNF antibodies [40-42]. However, our results differed. This discrepancy may reflect the biggest difference between our study and previous ones; we included trials that were all prospective RCTs whereas previous studies were almost all retrospective which tend to show larger risk values. Moreover, the mechanisms of anti-TNF antibodies and receptor fusion proteins are different; besides TNF-α, ETA also inhibits TNF-β. In an animal model of uveitis, higher TNF-β levels were found; ETA would therefore be expected to be even more effective [43]. More RCTs are required to further define the effect of ETA in AS patients with uveitis.
Braun et al. [44] investigated flare-ups or new-onset IBD in patients with AS who were treated with INF, ETA and ADA. New-onset and flares of IBD are infrequent in AS patients who receive anti-TNF therapy. The results showed that only INF and ADA might prevent IBD activity, both of which were associated with significant IBD rate reductions compared with ETA. The incidence of new-onset IBD in patients treated with placebo was not statistically different from that for any anti-TNF agent. ETA is not effective in controlling active CD [45]; in fact, cases have been reported of possible associated CD flare-ups [46] or new-onset CD [47] in AS patients undergoing ETA therapy. In our meta-analysis, we found that neither monoclonal anti-TNF antibodies nor TNF receptor fusion proteins were efficacious for IBD, but monoclonal anti-TNF antibodies had lower OR (implying greater efficacy) than TNF receptor fusion proteins. Only 5 small RCTs in our analysis had AS patients with IBD who were treated with anti-TNF agents. More RCT data is needed to establish the efficacy of anti-TNF antibodies for IBD in these patients.
Although anti-TNF agents are effective in treating skin and nail lesions of psoriasis [48,49], treatment with anti-TNF agents also can result in new manifestations of psoriasis for some patients [50]. We were unable to assess this in our meta-analysis because the included trails had no reported data of psoriasis.
The present study evaluated the efficacy of anti-TNF therapy on the frequency of EAMs in patients with AS. Anti-TNF therapy including ETA could be a credible alternative for AS patients who have uveitis. However, no anti-TNF therapy was efficacious for treating IBD in patients with AS. The 8 included studies that met the inclusion criteria had high-moderate Jadad scores; therefore the conclusions of this systematic analysis are reliable. More high-quality, large prospective RCTs with long-term follow-up are needed to confirm the efficacy and outcomes of anti-TNF therapy for EAMs of AS.
Conclusions
Compared with placebo, anti-TNF therapy including ETA was associated with significantly fewer flares and new onset of uveitis, but were not significant efficacious for treating IBD in AS patients. This meta-analysis of patient-level data from 8 RCTs significantly advances the notion that anti-TNF therapy may be a credible alternative for AS patients with uveitis. Future studies involving anti-TNF therapy for EAMs of AS are needed.
Acknowledgements
We thank Marla Brunker who provided professional English editing service.
Abbreviations
- TNF
Anti-tumor necrosis factor
- AS
Ankylosing spondylitis
- EAM
Extra-articular manifestation
- RCT
Randomized controlled trial
- IBD
Inflammatory bowel disease
- CD
Crohn’s disease
- UC
Ulcerative colitis
- ASAS
Assessments in Ankylosing Spondylitis International Society
- EULAR
European League against Rheumatism
- NSAIDs
Non-steroidal anti-inflammatory drugs
- DMARDs
Disease-modifying antirheumatic drugs
- INF
Infliximab
- IgG
Immunoglobulin G
- ADA
Adalimumab
- GOL
Golimumab
- CZP
Certolizumab
- ETA
Etanercept
- OR
Odds ratio
- CI
Confidence interval
- HLA
Human leukocyte antigen
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
DW and NZ conceived and designed the study. DW, LXH and TJ analyzed and interpreted the data. YYG, NNX and SZ contributed to acquisition of data. All authors helped draft the manuscript and its revisions for critically important intellectual content, and gave final approval of the version to be published.
Contributor Information
Dan Wu, Email: crystal0553@163.com.
Ying-Ying Guo, Email: guoyy_sjhospital@163.com.
Nan-Nan Xu, Email: xunn_sjhospital@163.com.
Shuai Zhao, Email: zhaos_sjhospital@163.com.
Lin-Xin Hou, Email: houlx_sjhospital@163.com.
Ting Jiao, Email: jiaot_sjhospital@163.com.
Ning Zhang, Email: zhangn_sjhospital@163.com.
References
- 1.Sieper J, Rudwaleit M, Khan MA, Braun J. Concepts and epidemiology of spondyloarthritis. Best Pract Res Clin Rheumatol. 2006;20:401–17. doi: 10.1016/j.berh.2006.02.001. [DOI] [PubMed] [Google Scholar]
- 2.Lee JH, Jun JB, Jung S, Bae SC, Yoo DH, Kim TY, et al. Higher prevalence of peripheral arthritis among ankylosing spondylitis patients. J Korean Med Sci. 2002;17:669–73. doi: 10.3346/jkms.2002.17.5.669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vander Cruyssen B, Ribbens C, Boonen A, Mielants H, de Vlam K, Lenaerts J, et al. The epidemiology of ankylosing spondylitis and the commencement of anti-TNF therapy in daily rheumatology practice. Ann Rheum Dis. 2007;66:1072–7. doi: 10.1136/ard.2006.064543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Elewaut D, Matucci-Cerinic M. Treatment of ankylosing spondylitis and extra-articular manifestations in everyday rheumatology practice. Rheumatology (Oxford) 2009;48:1029–35. doi: 10.1093/rheumatology/kep146. [DOI] [PubMed] [Google Scholar]
- 5.Hajj-Ali RA, Lowder C, Mandell BF. Uveitis in the internist’s office: are a patient’s eye symptoms serious? Cleve Clin J Med. 2005;72:329–39. doi: 10.3949/ccjm.72.4.329. [DOI] [PubMed] [Google Scholar]
- 6.Rosembaum JT. Acute uveitis and spondyloarthropathies. Rheum Dis Clin North Am. 1992;18:143–51. [PubMed] [Google Scholar]
- 7.Stolwijk C, van Tubergen A, Castillo-Ortiz JD, Boonen A. Prevalence of extra-articular manifestations in patients with ankylosing spondylitis: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74:65–73. doi: 10.1136/annrheumdis-2013-203582. [DOI] [PubMed] [Google Scholar]
- 8.Muñoz-Fernández S, Hidalgo V, Fernández-Melón J, Schlincker A, Bonilla G, Ruiz-Sancho D, et al. Sulfasalazine reduces the number of flares of acute anterior uveitis over a one-year period. J Rheumatol. 2003;30:1277–9. [PubMed] [Google Scholar]
- 9.Simonini G, Paudyal P, Jones GT, Cimaz R, Macfarlane GJ. Current evidence of methotrexate efficacy in childhood chronic uveitis: a systematic review and meta-analysis approach. Rheumatology (Oxford) 2013;52:825–31. doi: 10.1093/rheumatology/kes186. [DOI] [PubMed] [Google Scholar]
- 10.Pérez-Guijo V, Santos-Lacomba M, Sánchez-Hernández M, Castro-Villegas Mdel C, Gallardo-Galera JM, Collantes-Estévez E. Tumour necrosis factor-alpha levels in aqueous humour and serum from patients with uveitis: the involvement of HLA-B27. Curr Med Res Opin. 2004;20:155–7. doi: 10.1185/030079903125002847. [DOI] [PubMed] [Google Scholar]
- 11.Rudwaleit M, Rødevand E, Holck P, Vanhoof J, Kron M, Kary S, et al. Adalimumab effectively reduces the rate of anterior uveitis flares in patients with active ankylosing spondylitis: results of a prospective open-label study. Ann Rheum Dis. 2009;68:696–701. doi: 10.1136/ard.2008.092585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Braun J, Baraliakos X, Listing J, Sieper J. Decreased incidence of anterior uveitis in patients with ankylosing spondylitis treated with the anti-tumor necrosis factor agents infliximab and etanercept. Arthritis Rheum. 2005;52:2447–51. doi: 10.1002/art.21197. [DOI] [PubMed] [Google Scholar]
- 13.Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60:571–607. doi: 10.1136/gut.2010.224154. [DOI] [PubMed] [Google Scholar]
- 14.Williams C, Panaccione R, Ghosh S, Rioux K. Optimizing clinical use of mesalazine (5-aminosalicylic acid) in inflammatory bowel disease. Therap Adv Gastroenterol. 2011;4:237–48. doi: 10.1177/1756283X11405250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Braun J, Baraliakos X, Listing J, Davis J, van der Heijde D, Haibel H, et al. Differences in the incidence of flares or new onset of inflammatory bowel diseases in patients with ankylosing spondylitis exposed to therapy with anti-tumor necrosis factor alpha agents. Arthritis Rheum. 2007;57:639–47. doi: 10.1002/art.22669. [DOI] [PubMed] [Google Scholar]
- 16.Braun J, van den Berg R, Baraliakos X, Boehm H, Burgos-Vargas R, Collantes-Estevez E, et al. 2010 update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis. 2011;70:896–904. doi: 10.1136/ard.2011.151027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Feldmann M, Elliott MJ, Woody JN, Maini RN. Anti‑tumor necrosis factor- alpha therapy of rheumatoid arthritis. Adv Immunol. 1997;64:283–350. doi: 10.1016/S0065-2776(08)60891-3. [DOI] [PubMed] [Google Scholar]
- 18.Nash PT, Florin TH. Tumour necrosis factor inhibitors. Med J Aust. 2005;183:205–8. doi: 10.5694/j.1326-5377.2005.tb06998.x. [DOI] [PubMed] [Google Scholar]
- 19.Deeks ED. Certolizumab pegol: a review of its use in the management of rheumatoid arthritis. Drugs. 2013;73:75–97. doi: 10.1007/s40265-013-0009-3. [DOI] [PubMed] [Google Scholar]
- 20.Moreland LW, Baumgartner SW, Schiff MH, Tindall EA, Fleischmann RM, Weaver AL, et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor(p75)‑Fc fusion protein. N Engl J Med. 1997;337:141–7. doi: 10.1056/NEJM199707173370301. [DOI] [PubMed] [Google Scholar]
- 21.Giardina AR, Ferrante A, Ciccia F, Impastato R, Miceli MC, Principato A, et al. A 2-year comparative open label randomized study of efficacy and safety of etanercept and infliximab in patients with ankylosing spondylitis. Rheumatol Int. 2010;30:1437–40. doi: 10.1007/s00296-009-1157-3. [DOI] [PubMed] [Google Scholar]
- 22.Braun J, Baraliakos X, Hermann KG, van der Heijde D, Inman RD, Deodhar AA, et al. Golimumab reduces spinal inflammation in ankylosing spondylitis: MRI results of the randomised, placebo- controlled GO-RAISE study. Ann Rheum Dis. 2012;71:878–84. doi: 10.1136/annrheumdis-2011-200308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baraliakos X, Listing J, Fritz C, Haibel H, Alten R, Burmester GR, et al. Persistent clinical efficacy and safety of infliximab in ankylosing spondylitis after 8 years–early clinical response predicts long-term outcome. Rheumatology (Oxford) 2011;50:1690–9. doi: 10.1093/rheumatology/ker194. [DOI] [PubMed] [Google Scholar]
- 24.Braun J, van der Horst-Bruinsma IE, Huang F, Burgos-Vargas R, Vlahos B, Koenig AS, et al. Clinical efficacy and safety of etanercept versus sulfasalazine in patients with ankylosing spondylitis: a randomized, double-blind trial. Arthritis Rheum. 2011;63:1543–51. doi: 10.1002/art.30223. [DOI] [PubMed] [Google Scholar]
- 25.Sieper J, van der Heijde D, Dougados M, Brown LS, Lavie F, Pangan AL. Early response to adalimumab predicts long-term remission through 5 years of treatment in patients with ankylosing spondylitis. Ann Rheum Dis. 2012;71:700–6. doi: 10.1136/annrheumdis-2011-200358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Machado MA, Barbosa MM, Almeida AM, de Araújo VE, Kakehasi AM, Andrade EI, et al. Treatment of ankylosing spondylitis with TNF blockers: a meta-analysis. Rheumatol Int. 2013;33:2199–213. doi: 10.1007/s00296-013-2772-6. [DOI] [PubMed] [Google Scholar]
- 27.Oremus M, Wolfson C, Perrault A, Demers L, Momoli F, Moride Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement Geriatr Cogn Disord. 2001;12:232–6. doi: 10.1159/000051263. [DOI] [PubMed] [Google Scholar]
- 28.Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cochrane handbook for systematic reviews of interventions version 5.1.0 (updated March 2011). [http://handbook.cochrane.org/].
- 30.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 31.van der Heijde D, Kivitz A, Schiff MH, Sieper J, Dijkmans BA, Braun J, et al. Efficacy and safety of adalimumab in patients with ankylosing spondylitis: results of a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2006;54:2136–46. doi: 10.1002/art.21913. [DOI] [PubMed] [Google Scholar]
- 32.Brandt J, Khariouzov A, Listing J, Haibel H, Sörensen H, Grassnickel L, et al. Six-month results of a double-blind, placebo-controlled trial of etanercept treatment in patients with active ankylosing spondylitis. Arthritis Rheum. 2003;48:1667–75. doi: 10.1002/art.11017. [DOI] [PubMed] [Google Scholar]
- 33.Davis JC, Jr, Van Der Heijde D, Braun J, Dougados M, Cush J, Clegg DO, et al. Recombinant human tumor necrosis factor receptor (etanercept) for treating ankylosing spondylitis: a randomized, controlled trial. Arthritis Rheum. 2003;48:3230–6. doi: 10.1002/art.11325. [DOI] [PubMed] [Google Scholar]
- 34.van der Heijde D, Da Silva JC, Dougados M, Geher P, van der Horst-Bruinsma I, Juanola X, et al. Etanercept 50 mg once weekly is as effective as 25 mg twice weekly in patients with ankylosing spondylitis. Ann Rheum Dis. 2006;65:1572–7. doi: 10.1136/ard.2006.056747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Braun J, Brandt J, Listing J, Zink A, Alten R, Golder W, et al. Treatment of active ankylosing spondylitis with infliximab: a randomised controlled multicentre trial. Lancet. 2002;359:1187–93. doi: 10.1016/S0140-6736(02)08215-6. [DOI] [PubMed] [Google Scholar]
- 36.Marzo-Ortega H, McGonagle D, Jarrett S, Haugeberg G, Hensor E, O’connor P, et al. Infliximab in combination with methotrexate in active ankylosing spondylitis: a clinical and imaging study. Ann Rheum Dis. 2005;64:1568–75. doi: 10.1136/ard.2004.022582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Inman RD, Davis JC, Jr, Heijde D, Diekman L, Sieper J, Kim SI, et al. Efficacy and safety of golimumab in patients with ankylosing spondylitis: results of a randomized, double-blind, placebo-controlled, phase III trial. Arthritis Rheum. 2008;58:3402–12. doi: 10.1002/art.23969. [DOI] [PubMed] [Google Scholar]
- 38.Landewé R, Braun J, Deodhar A, Dougados M, Maksymowych WP, Mease PJ, et al. Efficacy of certolizumab pegol on signs and symptoms of axial spondyloarthritis including ankylosing spondylitis: 24-week results of a double-blind randomised placebo-controlled Phase 3 study. Ann Rheum Dis. 2014;73:39–47. doi: 10.1136/annrheumdis-2013-204231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Guignard S, Gossec L, Salliot C, Ruyssen-Witrand A, Luc M, Duclos M, et al. Efficacy of tumour necrosis factor blockers in reducing uveitis flares in patients with spondyloarthropathy: a retrospective study. Ann Rheum Dis. 2006;65:1631–4. doi: 10.1136/ard.2006.052092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pato E, Muñoz-Fernández S, Francisco F, Abad MA, Maese J, Ortiz A, et al. Systematic review on the effectiveness of immunosuppressants and biological therapies in the treatment of autoimmune posterior uveitis. Semin Arthritis Rheum. 2011;40:314–23. doi: 10.1016/j.semarthrit.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 41.D’Angelo S, Palazzi C, Cantini F, Lubrano E, Marchesoni A, Mathieu A, et al. Etanercept in spondyloarthopathies. Part II: safety and pharmacoeconomic issues. Clin Exp Rheumatol. 2011;29:865–70. [PubMed] [Google Scholar]
- 42.Wendling D, Paccou J, Berthelot JM, Flipo RM, Guillaume-Czitrom S, Prati C, et al. New onset of uveitis during anti-tumor necrosis factor treatment for rheumatic diseases. Semin Arthritis Rheum. 2011;41:503–10. doi: 10.1016/j.semarthrit.2011.05.005. [DOI] [PubMed] [Google Scholar]
- 43.Savion S, Oddo S, Grover S, Caspi RR. Uveitogenic T lymphocytes in the rat: pathogenicity vs. lymphokine production, adhesion molecules and surface antigen expression. J Neuroimmunol. 1994;55:35–44. doi: 10.1016/0165-5728(94)90144-9. [DOI] [PubMed] [Google Scholar]
- 44.Braun J, Baraliakos X, Listing J, Davis J, van der Heijde D, Haibel H, et al. Differences in the incidence of flares or new onset of inflammatory bowel diseases in patients with ankylosing spondylitis exposed to therapy with anti-tumor necrosis factor alpha agents. Arthritis Rheum. 2007;57:639–47. doi: 10.1002/art.22669. [DOI] [PubMed] [Google Scholar]
- 45.Sandborn WJ, Hanauer SB, Katz S, Safdi M, Wolf DG, Baerg RD, et al. Etanercept for active Crohn’s disease: a randomized, double-blind, placebo-controlled trial. Gastroenterology. 2001;121:1088–94. doi: 10.1053/gast.2001.28674. [DOI] [PubMed] [Google Scholar]
- 46.Marzo-Ortega H, McGonagle D, O’Connor P, Emery P. Efficacy of etanercept for treatment of Crohn’s related spondyloarthritis but not colitis. Ann Rheum Dis. 2003;62:74–6. doi: 10.1136/ard.62.1.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Song IH, Appel H, Haibel H, Loddenkemper C, Braun J, Sieper J, et al. New onset of Crohn’s disease during treatment of active ankylosing spondylitis with etanercept. J Rheumatol. 2008;35:532–6. [PubMed] [Google Scholar]
- 48.Kyriakou A, Patsatsi A, Sotiriadis D. Anti-TNF agents and nail psoriasis: a single-center, retrospective, comparative study. J Dermatolog Treat. 2013;24:162–8. doi: 10.3109/09546634.2011.646939. [DOI] [PubMed] [Google Scholar]
- 49.Leonardi CL, Powers JL, Matheson RT, Goffe BS, Zitnik R, Wang A, et al. Etanercept Psoriasis Study Group. Etanercept as monotherapy in patients with psoriasis. N Engl J Med. 2003;349:2014–22. doi: 10.1056/NEJMoa030409. [DOI] [PubMed] [Google Scholar]
- 50.Grinblat B, Scheinberg M. The enigmatic development of psoriasis and psoriasiform lesions during anti-TNF therapy: a review. Semin Arthritis Rheum. 2008;37:251–5. doi: 10.1016/j.semarthrit.2007.05.004. [DOI] [PubMed] [Google Scholar]