

Abstract
Purpose
The purpose of this study was to examine a J-shaped relationship between alcohol consumption and depression among the elderly in South Korea.
Materials and Methods
Cross-section data were drawn from a community-based sample of individuals 60 years of age and older (n=1819). Respondents completed the Alcohol Use Disorders Intensification Test (AUDIT) and the Korean Beck Depression Inventory. Using a regression approach, the effect of alcohol consumption as a non-linear effect was assessed in relation to gender, marital status, exercise, smoking, age, education, and physical and mental health.
Results
AUDIT total score were found to exert linear and quadratic effects that were significantly associated with higher depression scores among sample respondents. The results lend support to a J-shaped relationship between alcohol use and depression, wherein abstainers and problem drinkers were at a higher risk of depression.
Conclusion
This study confirms a J-shaped (i.e., curvilinear) relationship between alcohol consumption and depression among elderly South Koreans, similar to that frequently found in studies of Western-based samples. The findings of this study, therefore, imply the applicability of the J-shaped relationship hypothesis for non-Western society samples and within different cultural contexts.
Keywords: Depression, alcohol consumption, AUDIT, BDI, a J-shaped relationship, South Korean elderly population in Gangneung city
INTRODUCTION
Co-morbidity between hazardous alcohol use and various types of mental problems is well established in the literature.1,2,3,4,5,6,7 Studies consistently demonstrate that excessive levels of alcohol consumption are associated with an elevated risk of depressive symptoms and various types of mental disorders.6,7,8,9 There remains, however, a debate regarding the strength and direction of this relationship.10,11,12,13,14 Recent studies have offered evidence in support of the existence of a curvilinear, J-shaped, relationship, between alcohol consumptions and depression, indicating that both abstainers and heavy drinkers are at an increased risk for symptoms of major depression, compared to moderate drinkers, while a relatively smaller group of studies have reported inconsistent findings as to the existence and importance of the non-linear relationship.3,10,11,12,13,14,15
In response to these inconsistent findings, some scholars have proposed alternative explanations regarding the increased risk of depression among abstainers: 1) moderate alcohol use may exert direct and positive effects on mental health, resulting in the psychological wellbeing of the moderate alcohol consumers;15 2) results mat reflect a failure to control for confounding factors from a range of correlates relevant to depression.14 With regard to the confounding effects of correlates of depression, it is true that the nature of the association between alcohol use and symptoms of depression may vary according to age. Thus, the relationship may need to be studied in ways that consider relevant social and biological correlates with depression, such as exercise, smoking, education, health condition, and general mental health levels. Studies to date, however, have yet to account for these factors in examining the potential of a quadratic relationship between alcohol consumption and its effect on depression.
Furthermore, even if a J-shaped relationship does exist, there is still lack of understanding regarding whether this non-linear relationship exists across varying age groups. Since alcohol consumption patterns are less systematic by age, it is not clear whether a non-linear curve can be identified across every age group. Particularly, studies examining problems associated with alcohol use among the elderly are quite rare and findings are generally mixed.14,16,17
Overall, given the discrepancy and lack of studies examining the elderly, regarding a J-shaped or J-shaped relationship between alcohol use and its effect on depression, it is important to implement empirical research examining its existence. The importance of such exploration lies in our understanding of the etiology of the mental health problems often associated with alcohol consumption, which is critical in developing effective preventive strategies and programming.10
Therefore, the purpose of the present study was to examine the nature and shape of any association between alcohol consumption and depression in a very large community-based sample of elderly South Korea individuals. Specifically, this study was designed to control for various measures identified as social correlates of depression risk in previous studies that have not been routinely accounted for when assessing there relation to alcohol consumption.18,19
MATERIALS AND METHODS
Participants, data, and sampling
The present study utilized a cross-sectional survey of individuals that collected information specific to alcohol consumption and depression among a community-based sample of individuals aged 60 years or older, residing in Gangneung city, South Korea. Individuals were selected for participation via a two-staged clustered random sampling method. By utilizing the cluster sampling process, the authors attempted to ensure that the sample represented the city's varying socioeconomic levels. First, city units (villages) within Gangneung were randomly selected on the basis of their geographic location. In the second stage, participants older than 60 years were randomly selected within those selected geographical units and invited to participate in the survey (discussed below). The data collection was conducted from 2002 to 2007 at a senior center in each village.
More specifically, at the beginning of the study, participants were informed about the purpose of the study. Upon an orientation, trained medical student interviewers individually conducted face-to-face interviews with respondents, which lasted about 30 minutes to one hour. For the data collection, informed consent was obtained before beginning the interviews from all participants in accordance with the requirement of the Institutional Review Board of the Medical College at Catholic Kwandong University. A total of 1819 individuals participated.
Measures
Problem alcohol consumption
This study utilized the 10-item Alcohol Use Disorders Identification Test (AUDIT) to assess a range of alcohol use behavior (Cronbach's alpha=0.89). AUDIT is a screening instrument that is particularly useful in measuring excessive alcohol consumption, such as dependency, harmful drinking, and diagnosed alcohol abuse, and is widely used in measuring alcohol related social and medical problems in the general population.15,20 The scores of AUDIT have a possible range from 0 to 40. In many Western countries, a standard cutoff score of 8 indicates problem and hazardous drinking behaviors with higher cutoffs (12 and 22) indicating alcohol-related problems. In Korea, however, scores of 12, 15, and 26 have been suggested as cutoff scores for problematic drinkers (lower levels and higher levels of problem drinkers), harmful/hazardous drinkers, respectively.21 The sensitivity and specificity of these cutoffs among Korean are 85.7-96.9% and 79.5-100%, respectively.21 In the present study, on the basis of the previous Korean study, an AUDIT score of 12 was used to identify problem drinking. Thus, respondents with scores lower than 12 were considered not to have an alcohol consumption problem.
Depression
The measure of depression used in this study was primarily derived from the participants' response to a Korean version of the Beck Depression Inventory (K-BDI).22 BDI is a self-reported instrument consisting of 21 items survey questionnaires with a 4-point Likert Scale (Cronbach's alpha=0.91). Possible scores of the K-BDI range from 0 to 63. The applicability of K-BDI has been validated by Han, et al.'s23 study, and the reliability of the instrument has been identified as 0.86 for men and 0.84 for women.24,25 With regard to the cutoff score of the K-BDI, Korean scholars suggest that Korean adults show relatively higher mean scores of K-BDI, compared to the samples in Western countries.21,23,24,25 Kim, et al.21 explains that this is partially due to the Korean culture of allowing widespread expression of depression symptoms even among the normal population. Given that the higher mean score on the BDI for Korean adults (mean=12.7, SD=7.73) and distinctive culture from the Western societies, studies agree that the higher cutoff score for this study would be considered to be appropriate for Korean samples. In our study, therefore, a score of 21 indicates the optimal cutoff score for major depression, which is higher than the cutoff score of 13 used in samples from Western countries.
Potential confounding factors
Several potential confounding factors identified as correlates of depression in previous studies were included herein. Such factors included gender, age, marital status, education, current smoking, exercise, and physical and psychological well-being of the participants. General physical and psychological well-being of the participants was measured by Short Form-12 (Version 1) (SF-12). The Short Form-12 (Version 1) Health Survey (SF-12) is a 12-item self-reported instrument designed to access general physical and psychological well-being with strong validity and reliability. SF-12 consists of Mental Component Summary (MCS) and Physical Component Summary (PCS), with scores for each component ranging from 0 to 100. Higher scores reflect better health (Cronbach's alpha=0.85).
The exercise variable was measured by asking participants if they exercised at least once a week. Each participant's response was coded as a binary measure (yes=1, no=0). Smoking is an indicator of current smoking status of the participant at the time of survey (smoking=1, non-smoking=0). Marital status measure reflects the classification of marital or single status of the participant. Specifically, the single status includes various single life styles, such as divorced, being a widow/widowers, and never having been married [married=1, not married (single status)=0]. Educational attainment measure reflects year of education the participants completed. Gender (male=1, female=0) and age (a continuous measure, over 60 years only) also were included as important control measures in this study.
Analysis
We first report descriptive statistics to describe the socio-demographic characteristics of the sample and the prevalence rate of depression and problem drinking behavior. Further, the mean score for depression and the result of one-way ANOVA test of the four different alcohol use groups based on AUDIT scores are presented. Next, we report on a set of bivariate correlations and mean difference tests among key variables. Finally, a multiple regression (OLS) analysis with polynomial explanatory variables is utilized to examine the risk of depression (BDI scores) on the basis of the reported AUDIT scores with controlled covariates in the model. Particularly, a quadratic term for AUDIT was specified to further examine curvilinear trends in AUDIT and BDI. Finally, in an attempt to determine the functional form of the relationship between depression and AUDIT scores, a graph of this relationship was generated after conditioning for the influence of the control variables on the independent variables.
RESULTS
Descriptive and bivariate analyses
Table 1 presents descriptive statistics for the participants. In this sample, 35% of the participants were men, while 65% of the participants were women. The age of the respondents ranged from 60 to 105 years, with a mean age of 75.6 years old (SD=7.8). When age was broken down into three categories about 29% of the participants were between 60 and 70 years old, about 43% were between 71 and 80 years old, and about 29% were 81 years old or over. The average educational attainment was 4.3 years, ranging from 0 to 20 (SD=4.4) and the majority of the participants (80%) reported that they had completed an elementary school level education or less only. Additionally, in terms of the average educational attainment of the participants, the level of education was pretty low, indicating that the entire sample only completed elementary school or less. Finally, of the total participants, 49.6% reported they were married, 18% were current smokers, and 38% were involved in at least once a week exercise at the time of data collection.
Table 1.
Socio-Demographic Characteristics of the Participants Together with Scores on Measurement Instruments (n=1819)
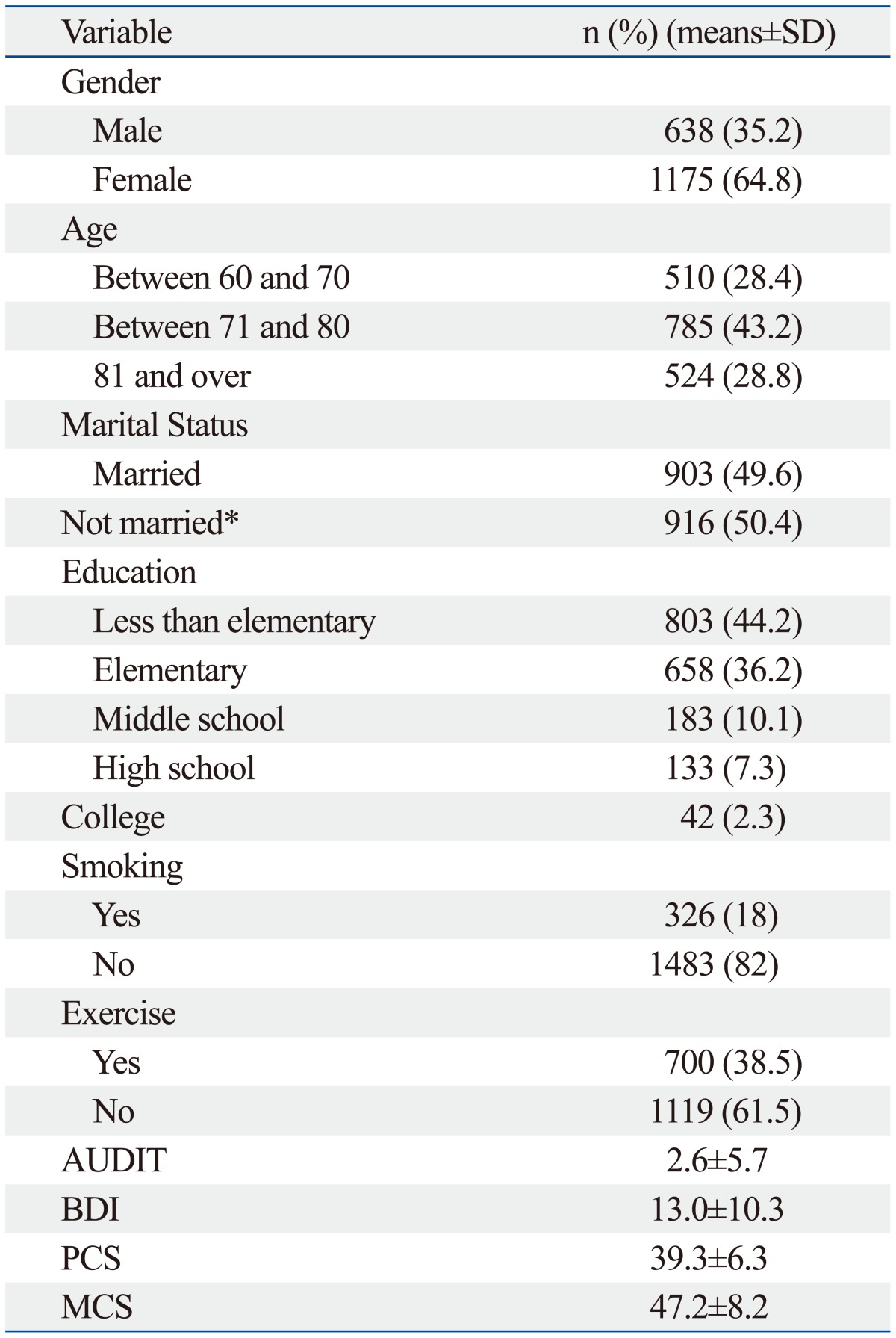
AUDIT, Alcohol Use Disorders Identification Test; BDI, Beck Depression Inventory; PCS, Physical Component Summary; MCS, Mental Component Summary.
*Includes divorced, being a widow or widower, and never having been married.
The prevalence of problem drinking was 8.4% of the total sample, with a mean AUDIT score of 2.6 (SD=5.7), ranging from 0 to 38. The prevalence of depression was 18.5% of the total sample and the average score of the K-BDI was 13.0 (SD=10.3), with a range of 1 to 62. Regarding physical and psychological wellbeing, the mean scores of PCS and MCS were 39.3 (SD=6.3) and 47.2 (SD=8.2), respectively.
Table 2 presents the mean scores on BDI according to four different levels of alcohol use groups on the basis of the AUDIT scores. A one-way ANOVA test indicated a significant effect of AUDIT on BDI for the four conditions (F=18.59 <0.001***). As for non-problem drinkers, defined as those who scored less than 12 on AUDIT, the mean score for depression was 14.1 (SD=10.7). The mean scores on depression among individuals who exhibited "problematic but lower level drinker," "problematic and higher level drinker," and "harmful/hazardous drinker" were 8.4, 9.3, and 10.9, respectively. This finding suggests the potential for a J-shaped relationship between AUDIT and BDI scores in this sample.
Table 2.
Mean Scores of Beck Depression Inventory for Different Level of Alcohol Consumptions of the Elders

AUDIT, Alcohol Use Disorders Identification Test.
***p<0.001.
†Participants' AUDIT score<12 score.
‡12≤participants' AUDIT score<15 score.
§15≤participants' AUDIT score<26 score.
∥26≤participants' AUDIT score & above.
Table 3 demonstrates the results of group-mean difference test for depression of the variables. As shown in the table, women were more likely report depression than men. The participants who reported being married and involved in weekly exercise were less likely to report depression symptoms than their counterparts, while there was no significant mean difference found between smokers and non-smokers.
Table 3.
Bivariate Analysis of Variables with BDI
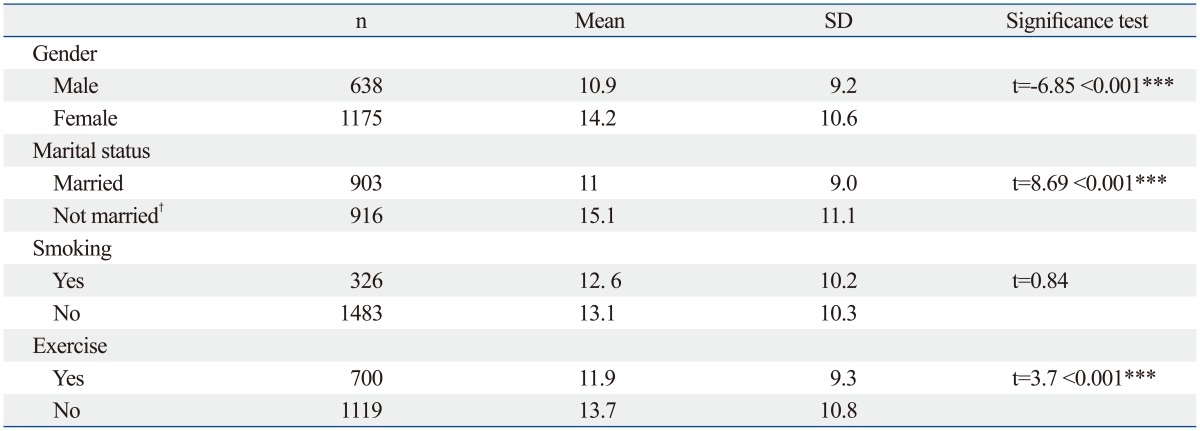
BDI, Beck Depression Inventory.
***p<0.001.
†Includes divorced, being a widow or widower, and never having been married.
Table 4 presents bivariate correlation analyses among the variables. AUDIT, PCS, MCS, and education were significantly associated with BDI. Specifically, AUDIT and MCS exhibited a negative association, while PCS and education attainment had a positive relationship with BDI. These relationships indicate that participants who reported higher levels of alcohol use and higher scores on mental health were less likely to report depression symptoms (AUDITr=-0.11, MCSr=-0.31, p<0.001, respectively). On the other hand, the participants who reported higher scores on physical well-being and higher levels of educational attainment were more likely to report higher levels of depression (PCSr=0.05*, Educationr=-0.01*, p<0.05, respectively).
Table 4.
Correlation Matrix

BDI, Beck Depression Inventory; AUDIT, Alcohol Use Disorders Identification Test; PCS, Physical Component Summary; MCS, Mental Component Summary.
*p<0.05.
**p<0.01.
***p<0.001.
†Total number of years educated.
Multiple regression analysis
Multiple regression results are presented in Table 5. In this model, specifically, a quadratic term of AUDIT2, which is a separate score of AUDIT, was included in order to test for a curvilinear relationship between problem alcohol use and depression. The model results revealed a J-shaped relationship between problem drinking and depression. The problem alcohol use measures, AUDIT (linear) and AUDIT2 (quadratic), were significantly associated with depression, net of other effects. Fig. 1 graphically illustrates the pattern of a curvilinear relationship between AUDIT and BDI after having conditioned for other influential variables. In Fig. 1, the turning point value of AUDIT, where the negative relationship of AUDIT and BDI changed to the positive direction, was a score of 11.67, which is close to the AUDIT score of 12 that is defined as problematic drinking and differentiated from alcohol disorder and dependence among elderly Koreans. Therefore, among non-problem drinkers, the effect of alcohol use was negatively related to depression. For problem-drinkers, however, increased alcohol use was associated with higher levels of depression.
Table 5.
Results of Multiple Regression on Depression (n=1819)
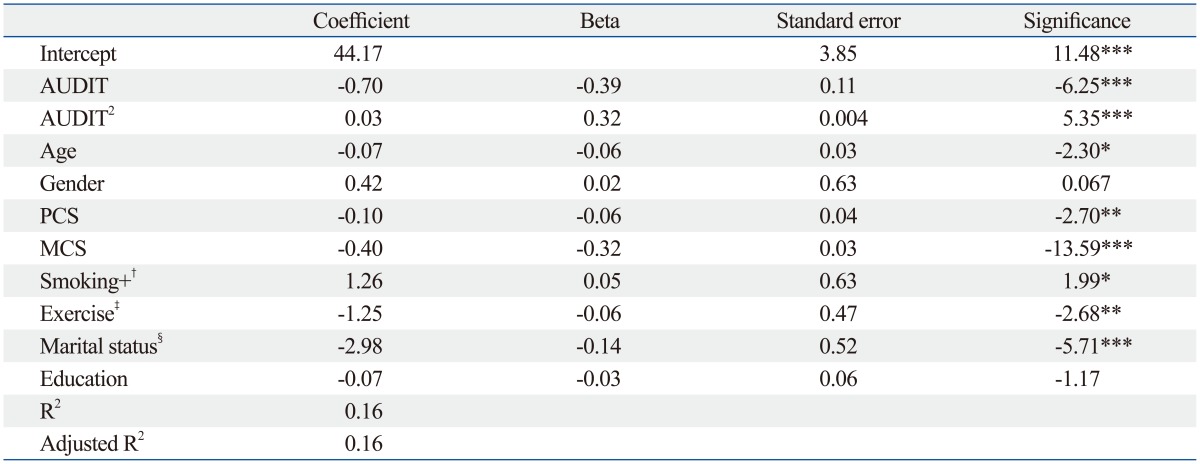
AUDIT, Alcohol Use Disorders Identification Test; AUDIT2, a quadratic term of AUDIT score; PCS, Physical Component Summary; MCS, Mental Component Summary.
*p<0.05.
**p<0.01.
***p<0.001.
†1=smoking, 0=non-smoking.
‡1=yes, 0=no.
§1=married, 0=not married.
Fig. 1.

Curvilinear relationship between depression and alcohol consumption after controlling for other variables (n=1819). AUDIT, Alcohol Use Disorders Identification Test; BDI, Beck Depression Inventory.
With regard to controlling factors included in the regression model, age, smoking, exercise, marital status and psychical and mental health were found to be statistically significant correlates of depression, relatively speaking, and net of other effects. Both PCS and MCS were found to have negative and significant effects on depression (beta=-0.06, p<0.01, beta=-0.32, p<0.001, respectively), indicating physical and mental well-being of the elderly are protective factors in terms of self-reported depression. In terms of the size of standardized beta coefficients of these two variables, the MCS was the second most influential factors associated with depression, followed by the AUDIT score in this model. This finding indicates that mental well-being has greater influence on reducing depression than that of physical well-being for the elderly group.
Being married was found to be the third most influential factors in reducing the depression, indicating married participants were more likely to report lower level of risk for depression than their counterparts (beta=-0.14, p<0.001). Participants who were younger (beta=-0.06, p<0.05) and involved in exercise at least once a week (beta=-0.06, p<0.05) were more likely to report lower levels of depression. Finally, participants who reported being a current smoker were more likely to report higher levels of depression (beta=0.05, p<0.05).
DISCUSSION
The goal of the present study was to examine whether there exists a J-shaped relationship between alcohol consumption and depression in a Korean elderly population after controlling for various known correlates of depression. Specifically, this study utilized continuous measures of AUDIT (including a quadratic terms of AUDIT score) and BDI scores as independent and dependent variables in the analyses. Using data from a large community-based sample, this study confirmed the known J-shaped relationship between alcohol consumption and depression among the elderly population, especially in relation to a quadratic AUTID total score (Fig. 1).12,15 The general pattern found in the analysis, based on a quadratic specification of the AUDIT scale, was one of a rise in depression score only at the upper end of the AUDIT score. Conversely, the curve suggested decreased scores on the depression measure at the point around or above the problem drinking cutoff score of AUDIT. That is, consistent with previous studies, abstaining from alcohol is associated with depression, as is the case for problem drinking behavior. Moderate drinking was negatively associated with depression, while problem drinking increased the risk of higher levels of depression. Our findings thus imply that selective interventions designed to vary alcohol consumption level need to be developed specific to the elderly.
With regard to the correlates of depression, the directions of the relationship between the correlate and depression were consistent with previous studies. That is, younger, being married, and being involved in current exercise had protective effects on depression for the elderly, while smoking among the elderly was a risk factor for depression. Notably, however, gender was not a significant factor on depression in this sample. This finding is not contradictive of previous empirical studies, in that gender difference within this relationship has yet to be clearly established. Some studies, for example, report a stronger relationship between alcohol use and depression for women than men, while some other studies report the opposite relationship.8,9
Physical and mental well-being were found to be relevant to depression among the Korean elderly population. Both PCS and MCS were found to be negatively associated with depression, indicating physical and mental well-being has a protective function for the elderly, based on regression model results. Particularly, the results imply that intervention promoting mental well-being seems to be more promising in the prevention of depression for the elderly population. In fact, MCS reflecting mental well-being of the elderly was the second most impactful variable, followed by the AUDIT score in this multiple regression model.
In terms of PCS, however, there is one notable finding. That is, PCS was positively associated with BDI; however, in the multivariate model controlling for MCS and other correlates, the association between PCS and BDI became negative, indicating psychical well-being of the participants is related with lower level of BDI, which is a relationship frequently found in previous studies. These findings may suggest that MCS is a confounding factor that needs to be controlled for in clarifying a relationship between alcohol use and depression. Therefore, it implies that future studies need to consider including various correlates with depression and alcohol consumption, such as mental well-being in this study, to control for any potential confounding effects of these measures on the alcohol consumption/depression nexus.
This study has the following strengths: first, the study utilized a large and diverse community-based sample of the elderly population specific to South Korea. The majority of previous studies, in fact, have relied primarily on relatively small, hospitalized alcohol dependence populations with only young and intermediate age groups serving as participants. The present study presents results that aid in alleviating the general lack of understanding about the alcohol use/depression relationship specific to elderly individuals, particularly those who are over 60 years of age. Second, various correlates associated with depression, such as general mental health status, were controlled for in order to clarify the relationship between depression and alcohol consumption. Although many studies have identified contributing factors in the relationship between alcohol and depression, studies that have controlled for these variables are very rare.10,14 Validation of our findings are needed to more firmly established whether a J-shaped relationship between alcohol use and depression holds across different samples and between different contexts.
There are, however, some limitations to this study: first, a general shortcoming of the present study is the cross-sectional nature of the data, which limits the study's findings in terms of establishing causation among the relationship between alcohol consumption and depression. Secondly, in the sampling procedure, we randomly selected villages and were not able to include all of the population over 60 years in each village as an initial target population. Since interviews were conducted at a senior center that provides free medical check-ups for the study participants, there would be the possibility that some residents who were not mobile enough to come to the senior center would have been unable to participate in the research. Thirdly, this study used higher cutoff points of AUDIT score than those of Western studies in order to classify groups of problematic and harmful drinking groups from non-problematic drinkers in this sample. Although the suitability of using higher cutoffs were addressed in prior Korean studies, there is still lack of literature validating the use of higher cutoff AUDIT scores than that of Western studies, especially for elderly populations. Therefore, it is necessary that future studies investigate the validity of Korean version of cutoffs of AUDIT among the elderly population in Korea. Finally, the data used in this study were drawn from a specific region of the world, one city in South Korea, which restrains the possibility of generalizing the above findings to different populations, contexts, and cultures.
Overall, as societies move toward fast aging societies, there is a demand for better understanding of the effects of alcohol habits on prevalent mental problems in order to promote the psychological well-being of elderly individuals. Considering the lack of understanding about the relationship between depression and alcohol consumption among the elderly population, especially from within a sample drawn from South Korea, this study's finding of a J-shaped association contributes to the literature by filling a gap in the understanding of this complex relationship.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Currie SR, Patten SB, Williams JV, Wang J, Beck CA, El-Guebaly N, et al. Comorbidity of major depression with substance use disorders. Can J Psychiatry. 2005;50:660–666. doi: 10.1177/070674370505001013. [DOI] [PubMed] [Google Scholar]
- 2.Davis LL, Rush JA, Wisniewski SR, Rice K, Cassano P, Jewell ME, et al. Substance use disorder comorbidity in major depressive disorder: an exploratory analysis of the Sequenced Treatment Alternatives to Relieve Depression cohort. Compr Psychiatry. 2005;46:81–89. doi: 10.1016/j.comppsych.2004.07.025. [DOI] [PubMed] [Google Scholar]
- 3.Golding JM, Burnam MA, Wells KB. Alcohol use and depressive symptoms among Mexican Americans and non-Hispanic Whites. Alcohol Alcohol. 1990;25:421–432. [PubMed] [Google Scholar]
- 4.Grant BF, Harford TC. Comorbidity between DSM-IV alcohol use disorders and major depression: results of a national survey. Drug Alcohol Depend. 1995;39:197–206. doi: 10.1016/0376-8716(95)01160-4. [DOI] [PubMed] [Google Scholar]
- 5.Hasin DS, Grant BF. Major depression in 6050 former drinkers: association with past alcohol dependence. Arch Gen Psychiatry. 2002;59:794–800. doi: 10.1001/archpsyc.59.9.794. [DOI] [PubMed] [Google Scholar]
- 6.Degenhardt L, Hall W, Lynskey M. Alcohol, cannabis and tobacco use among Australians: a comparison of their associations with other drug use and use disorders, affective and anxiety disorders, and psychosis. Addiction. 2001;96:1603–1614. doi: 10.1046/j.1360-0443.2001.961116037.x. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva: World Health Organization; 2002. [Google Scholar]
- 8.Caldwell TM, Rodgers B, Jorm AF, Christensen H, Jacomb PA, Korten AE, et al. Patterns of association between alcohol consumption and symptoms of depression and anxiety in young adults. Addiction. 2002;97:583–594. doi: 10.1046/j.1360-0443.2002.00092.x. [DOI] [PubMed] [Google Scholar]
- 9.Hartka E, Johnstone B, Leino EV, Motoyoshi M, Temple MT, Fillmore KM. A meta-analysis of depressive symptomatology and alcohol consumption over time. Br J Addict. 1991;86:1283–1298. doi: 10.1111/j.1360-0443.1991.tb01704.x. [DOI] [PubMed] [Google Scholar]
- 10.Alati R, Lawlor DA, Najman JM, Williams GM, Bor W, O'Callaghan M. Is there really a 'J-shaped' curve in the association between alcohol consumption and symptoms of depression and anxiety? Findings from the Mater-University Study of Pregnancy and its outcomes. Addiction. 2005;100:643–651. doi: 10.1111/j.1360-0443.2005.01063.x. [DOI] [PubMed] [Google Scholar]
- 11.Graham K, Massak A, Demers A, Rehm J. Does the association between alcohol consumption and depression depend on how they are measured? Alcohol Clin Exp Res. 2007;31:78–88. doi: 10.1111/j.1530-0277.2006.00274.x. [DOI] [PubMed] [Google Scholar]
- 12.Power C, Rodgers B, Hope S. U-shaped relation for alcohol consumption and health in early adulthood and implications for mortality. Lancet. 1998;352:877. doi: 10.1016/S0140-6736(98)23937-7. [DOI] [PubMed] [Google Scholar]
- 13.Sareen J, McWilliams L, Cox B, Stein MB. Does a U-shaped relationship exist between alcohol use and DSM-III-R mood and anxiety disorders? J Affect Disord. 2004;82:113–118. doi: 10.1016/j.jad.2002.12.001. [DOI] [PubMed] [Google Scholar]
- 14.Skogen JC, Harvey SB, Henderson M, Stordal E, Mykletun A. Anxiety and depression among abstainers and low-level alcohol consumers. The Nord-Trøndelag Health Study. Addiction. 2009;104:1519–1529. doi: 10.1111/j.1360-0443.2009.02659.x. [DOI] [PubMed] [Google Scholar]
- 15.Rodgers B, Korten AE, Jorm AF, Jacomb PA, Christensen H, Henderson AS. Non-linear relationships in associations of depression and anxiety with alcohol use. Psychol Med. 2000;30:421–432. doi: 10.1017/s0033291799001865. [DOI] [PubMed] [Google Scholar]
- 16.Lopes MA, Furtado EF, Ferrioli E, Litvoc J, Bottino CM. Prevalence of alcohol-related problems in an elderly population and their association with cognitive impairment and dementia. Alcohol Clin Exp Res. 2010;34:726–733. doi: 10.1111/j.1530-0277.2009.01142.x. [DOI] [PubMed] [Google Scholar]
- 17.Osborn DP, Fletcher AE, Smeeth L, Stirling S, Bulpitt CJ, Breeze E, et al. Factors associated with depression in a representative sample of 14 217 people aged 75 and over in the United Kingdom: results from the MRC trial of assessment and management of older people in the community. Int J Geriatr Psychiatry. 2003;18:623–630. doi: 10.1002/gps.896. [DOI] [PubMed] [Google Scholar]
- 18.Khan AY, Carrithers J, Preskorn SH, Lear R, Wisniewski SR, John Rush A, et al. Clinical and demographic factors associated with DSM-IV melancholic depression. Ann Clin Psychiatry. 2006;18:91–98. doi: 10.1080/10401230600614496. [DOI] [PubMed] [Google Scholar]
- 19.Tambs K, Harris JR, Magnus P. Genetic and environmental contributions to the correlation between alcohol consumption and symptoms of anxiety and depression. Results from a bivariate analysis of Norwegian twin data. Behav Genet. 1997;27:241–250. doi: 10.1023/a:1025662114352. [DOI] [PubMed] [Google Scholar]
- 20.Bohn MJ, Babor TF, Kranzler HR. The Alcohol Use Disorders Identification Test (AUDIT): validation of a screening instrument for use in medical settings. J Stud Alcohol. 1995;56:423–432. doi: 10.15288/jsa.1995.56.423. [DOI] [PubMed] [Google Scholar]
- 21.Kim MH, Yum YS, Lee EJ, Yoon MS. The Korean family alcohol dependence and intervention program. J Korean Soc Welf. 1995;124:72–93. [Google Scholar]
- 22.Beck D. [Indication for psychoanalytic short time therapy] Z Psychosom Med Psychoanal. 1967;13:257–265. [PubMed] [Google Scholar]
- 23.Han HM, Shin YW, Kim KH, Yoon DJ, Chung KJ. A Standardization Study of Beck Depression inventory in Korea. J Korean Neuropsychiatr Assoc. 1986;25:487–502. [Google Scholar]
- 24.Lee MK, Lee YH, Park SH, Son CH, Jung YJ, Hong SK, et al. A Standardization Study of Beck Depression Inventory 2-Korean Version (K-BDI): Validity-I. Korean J Psychopathol. 1995;4:77–95. [Google Scholar]
- 25.Lee MK, Lee YH, Jung HY, Choi JH, Kim SH, Kim YK, et al. A Standardization Study of Beck Depression Inventory 2-Korean Version (K-BDI): Validity-II. Korean J Psychopathol. 1995;4:96–104. [Google Scholar]