

Abstract
Purpose
To evaluate the efficacy of minimal stimulation using discretely administered gonadotropin combined with clomiphene citrate (CC) or letrozole (LTZ) for intrauterine insemination (IUI) cycles.
Materials and Methods
Total 257 IUI cycles from 158 infertile couples were assessed. A CC dose of 100 mg/day (n=126 cycles) or a LTZ dose of 5 mg/day (n=131 cycles) was administered on days 3-5 of the menstrual cycle for 5 days. Each group received human menopausal gonadotropin at a dose of 150 IU by two or three alternative day: CC combined with alternate-day regimen for 2 or 3 days (CC+300, n=37; CC+450, n=89) and LTZ combined with alternate-day regimen for 2 or 3 days (LTZ+300, n=36; LTZ+450, n=95).
Results
The clinical pregnancy rate was comparable between the CC and LTZ groups (18.3% vs. 13.0%, p=0.243). The clinical pregnancy rate also showed no significant difference among the 4 groups (21.6% vs. 16.9% vs. 11.1% vs. 12.6%, p=0.507). The multiple pregnancy rate was significantly higher in LTZ compared to CC group (37.5% vs. 8.7%, p=0.028) and in the LTZ+450 compared to CC+450 group (50% vs. 13.3%, p=0.038). Overall, there were 15 cases of ovarian hyperstimulation syndrome (OHSS), with the prevalence being significantly lower in the LTZ compared to CC group (1.5% vs. 10.3%, p=0.003). OHSS was more prevalent in the CC+450 compared to the LTZ+450 group (12.4% vs. 1.1%, p=0.002).
Conclusion
Our findings suggest that minimal stimulation using two alternate-day gonadotropin with LTZ decreases the development of OHSS and multiple pregnancies, while maintaining comparable pregnancy rates in IUI cycles.
Keywords: Intrauterine insemination, minimal stimulation, gonadotropin, letrozole, clomiphene citrate
INTRODUCTION
In subfertile couples, intrauterine insemination (IUI) is often a stop gap treatment while waiting for, or instead of in-vitro fertilization (IVF). Although IUI has not been included as an assisted reproductive technique, it has been widely applied emdepirically.1,2 However, the superiority of IUI compared to that of IVF or efficacy of IUI compared to that of expectant management is debatable. In 2009, the European Society of Human Reproduction and Embryology Capri Workshop Group reviewed controversies in IUI on the basis of the available evidence.3 They suggested that compared to expectant management, IUI with stimulation might lead to improved clinical outcomes.4,5 Particularly, ovarian stimulation with gonadotropin may have a moderate benefit compared to clomiphene citrate,5,6 while still being associated with increased cost for the repeated injections, frequent monitoring, risk of multiple pregnancies7,8,9 and development of ovarian hyperstimulation syndrome (OHSS) as a complication.10,11
The most desirable goal of ovulation induction for IUI is a higher pregnancy rate with reduced complications. To achieve this goal, the use of minimal stimulation has been considered, because it has been reported to reduce complications while maintaining overall pregnancy rates.12 The concept of minimal stimulation was first proposed by Kistner in 1972, who used clomiphene citrate (CC) followed by overlapping human menopausal gonadotropin (hMG) to increase the pregnancy rate compared to the use of CC alone and to reduce the amount of hMG required for stimulation. Since then, research has continued using variable agents combined with various doses and types of gonadotropin. In spite of the heterogeneity of previous studies-ranging from retrospective reviews to prospective randomized controlled studies-investigating minimal stimulation, the clinical pregnancy rates reported were equal or superior to those in gonadotropin-only regimens.13,14 Furthermore, the use of minimal stimulation resulted in fewer stimulation days and less gonadotropin use, suggesting that it is more cost-effective than gonadotropin-only cycles.10,15,16,17
Although previous studies have reported comparable pregnancy outcomes for IUI using minimal stimulation,6,12,13,14,18 there is lack of evidence regarding the regimen to be selected in the clinical field. This study aimed to identify an efficacious regimen for discrete administration of gonadotropin combined with CC or letrozole (LTZ), to be used in ovulation induction for IUI.
MATERIALS AND METHODS
The present study was designed as a retrospective comparative study. From January 2008 to March 2013, 257 IUI cycles performed in 158 couples were included in this study. Only patients aged 25-42 years with at least one patent tube were included in this study. The indications for treatment were unexplained infertility, endometriosis or male factor infertility. While most couples had a duration of infertility ≥1 year and underwent a routine infertility workup, some of them had a duration <1 year, with participating women being aged >35 years. The following exclusion criteria were adopted: bilateral tubal obstruction, stage III-IV endometriosis, cycles using donor sperm, previous IUI attempts 4 or more, and cycles cancelled due to no ovarian response to ovarian stimulation. This study was approved by the Institutional Review Board at the Severance Hospital, Yonsei University College of Medicine.
All women underwent testing for tubal patency by hysterosalpingography, evaluation of pelvic anatomy by transvaginal ultrasound, and assessment of basal hormones on day 3 of the menstrual cycle. Semen parameters were interpreted using the World Health Organization (2010) criteria. The regimen of ovulation induction was determined based on the previous response or physician's preference. A dose of 100 mg/d CC (Clomiphene, Youngpoong Pharma, Seoul, Korea) or 5 mg/d LTZ (Femara, Novartis, Basel, Switzerland) was administered on days 3-5 of the menstrual cycle for 5 days. In combination with their fixed schedule for CC or LTZ, patients received two different regimens of hMG, (IVF-M, LG Life Sciences, Seoul, Korea), either 150 IU administered on day 6 and 8 of the menstrual cycle (2-day regimen, on alternate days) or 150 IU administered on days 5, 7, and 9 of the menstrual cycle (3-day regimen, on alternate days). A total of 257 cycles were divided into 2 main groups based on the fixed schedule treatment: the CC group (n=126) or LTZ group (n=131). Each group was further divided into two subgroups according to the alternate-day regimen of gonadotropin used: CC combined with a 2-day regimen (CC+300 group, n=37) or 3-day regimen (CC+450 group, n=89), and LTZ combined with a 2-day regimen (LTZ+300 group, n=36) or 3-day regimen (LTZ+450 group, n=95). The luteinizing hormone (LH) surge was tested using LH2 kits (Bayer Corporation, Tarrytown, NY, USA). When the mean diameter of the leading follicle reached 17-18 mm, an injection of 10000 IU of urinary human chorionic gonadotropin (hCG) (IVF-C, LG Life Sciences, Seoul, Korea) or 250 µg of recombinant hCG (Ovidrel, Serono, Geneva, Switzerland) was administered intramuscularly or subcutaneously. IUI was performed 38 h after hCG administration. If the urinary LH surge test was positive, the insemination was performed the day after detection of the spontaneous LH surge, following the hCG injection.
The semen samples were microscopically examined to determine sperm motility and concentration after 30 minutes of liquefaction at room temperature. Sperm samples for IUI were prepared by density gradient centrifugation. For the insemination process, a soft catheter (Wallace artificial insemination catheter, Smiths Medical, London, UK) was used to introduce 0.5 mL of the prepared semen into the uterine cavity. After insemination, luteal support was achieved with micronized progesterone vaginal suppositories (Utrogestan, Cassenne-Aventis, Paris, France), 400 mg daily for 2 weeks.
The primary outcome measures were achievement of pregnancy, multiple pregnancy, and OHSS development. The secondary outcome measures were the size of the leading follicle, endometrial thickness on the day of hCG administration, and number of growing and mature follicles. Clinical pregnancy was defined as the presence of an intrauterine gestational sac with a pulsating fetal heart beat on ultrasound. Multiple pregnancy was defined as the presence of >2 intrauterine gestational sacs with a pulsating fetal heart beat on ultrasound. OHSS was classified as mild, moderate, severe, and critical according to criteria described previously by Navot, et al.19
Data were analyzed using the SPSS software package, version 20.0 (IBM Inc., Armonk, NY, USA) by Student t-test and one-way ANOVA to compare means for normally distributed continuous variables. The Mann-Whitney U test was used for non-parametrically distributed variables. Fisher's exact test and the chi-square test were used for categorical variables. Univariate and multivariate logistic regression analyses were also performed. Sample size calculation was not performed since the study was designed as retrospective comparative study based on chart review. A p value <0.05 was considered statistically significant.
RESULTS
There were no significant differences between the 4 groups in terms of the women's age, duration of infertility, percentage of primary infertility, causes of infertility, and tubal patency. However, there was a significant difference in basal serum follicle-stimulating hormone (FSH) levels among the 4 groups, with the post hoc analysis showing significantly higher basal serum FSH levels in the LTZ+450 group compared to the CC+300 group (6.66±2.09 vs. 8.75±3.81, p=0.021). Furthermore, the number of previous IUI attempts was significantly different among the 4 groups, with the post hoc analysis showing a significantly higher number of previous IUI attempts in the LTZ+300 group compared to the CC+300 group (0.21±0.48 vs. 0.92±0.97 months, p=0.008) and in the LTZ+450 group compared to the CC+450 group (0.55±0.80 vs. 1.20±1.14, p<0.001) (Table 1).
Table 1.
Clinical Characteristics of Study Subjects
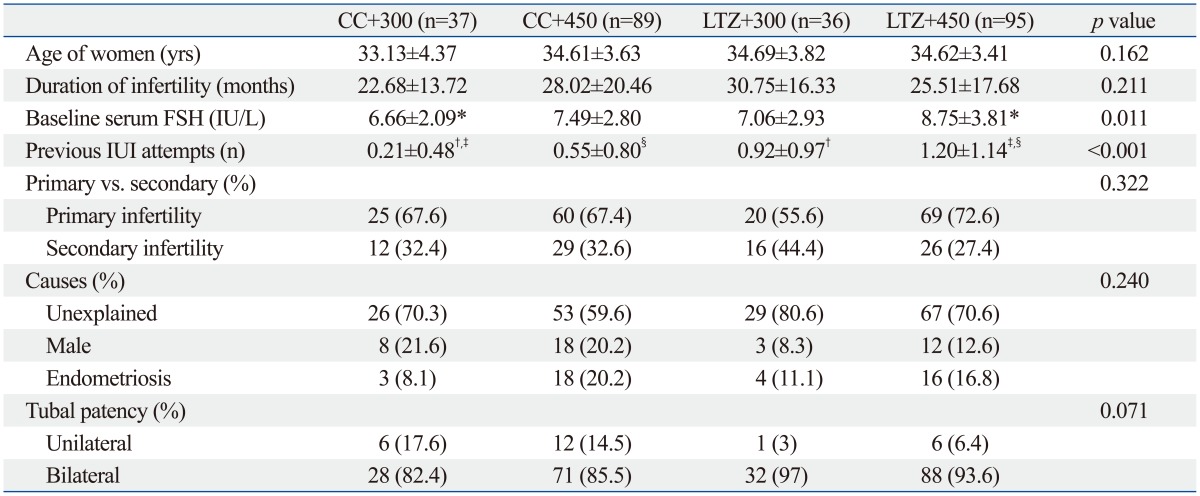
CC, clomiphene citrate; LTZ, letrozole; FSH, follicle-stimulating hormone; IUI, intrauterine insemination.
Values represent mean±SD.
*,†,‡,§Post-hoc p<0.05 by Bonferroni's multiple comparison test.
*CC300 vs. LTZ 450.
†CC300 vs. LTZ300.
‡CC300 vs. LTZ 450.
§CC450 vs. LTZ450.
The clinical pregnancy rate, multiple pregnancy rate, and the development of OHSS per cycle in the study population were 15.2%, 20.5%, and 5.8%, respectively. The clinical pregnancy rate was comparable between the CC and LTZ groups (18.3% vs. 12.2%, p=0.177). Multiple pregnancies occurred in 2 cases in the CC group and 6 cases in the LTZ group (8.7% vs. 37.5%, p=0.028), for a total of 7 twin and 1 triplet pregnancies. OHSS was significantly more prevalent in the CC group than in the LTZ group [13 cases (10.3%) vs. 2 cases (1.5%), p=0.003]. The size of the leading follicle and the number of follicles with a mean diameter of ≥18 mm on the day of hCG administration were comparable between the two groups. However, on the day of hCG administration, the number of follicles with a mean diameter 11-13 mm was significantly higher (0.93±1.27 vs. 0.49±0.83, p=0.001) and endometrial thickness was significantly lesser in the CC group (9.37±2.02 vs. 9.98±1.85, p=0.005) than the LTZ group. Although there was no difference in total motile sperm count (TMSC) before preparation between the two groups, the post-preparation sperm concentration was significantly higher in the LTZ group than in the CC group (Table 2).
Table 2.
The Outcomes of Intrauterine Insemination Cycles Using Gonadotropin Combined with Clomiphene Citrate or Letrozole
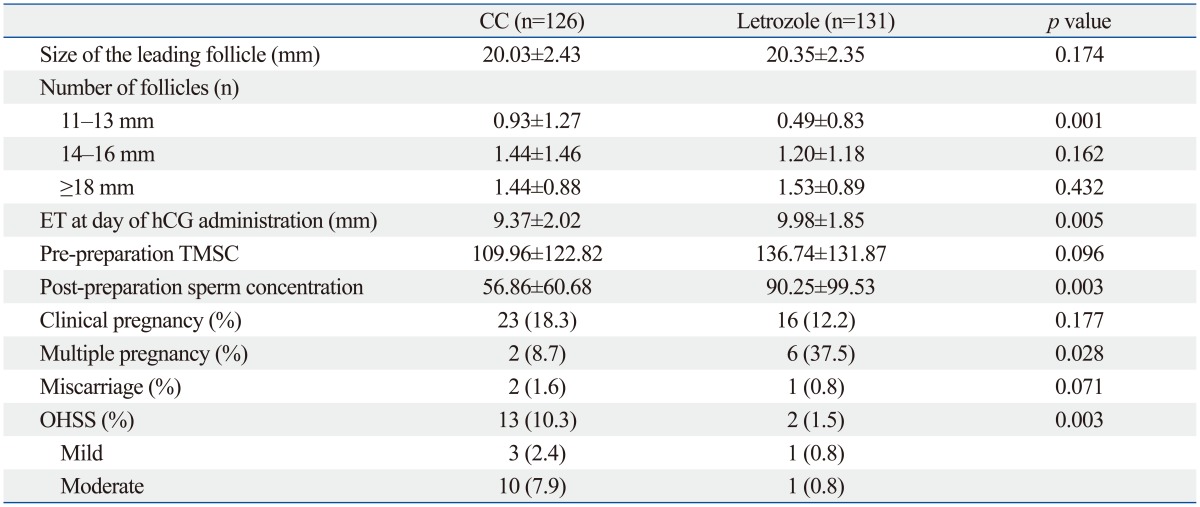
CC, clomiphene citrate; ET, endometrial thickness; OHSS, ovarian hyperstimulation syndrome; TMSC, total motile sperm count; hCG, human chorionic gonadotropin.
Values represent mean±SD.
In the cycles using CC, the primary and secondary outcomes were comparable between the alternate-day gonadotropin regimens of 2 and 3 days. However, the endometrial thickness on the day of hCG administration was significantly greater in the alternate-day regimen of 3 days compared to that of 2 days (8.77±2.11 mm vs. 9.62±1.94 mm, p=0.031). In the cycles using LTZ, the primary outcomes-clinical pregnancy rate, multiple pregnancy rate, and development of OHSS-and the secondary outcomes were similar between both alternate-day gonadotropin regimens (Table 3).
Table 3.
The Outcomes of IUI Cycles Using Four Regimens
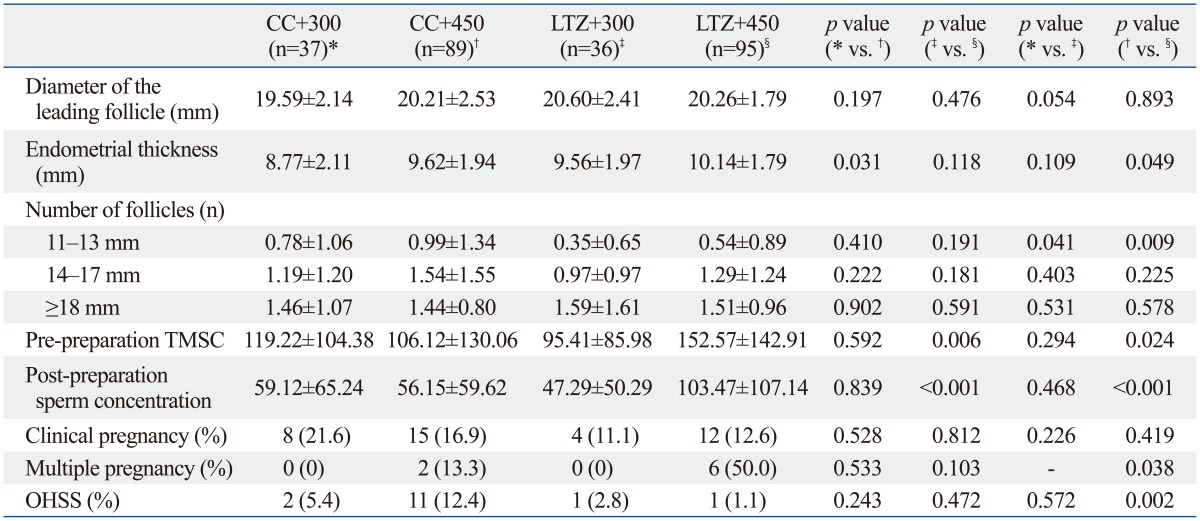
CC, clomiphene citrate; LTZ, letrozole; TMSC, total motile sperm count; OHSS, ovarian hyperstimulation syndrome; IUI, intrauterine insemination.
In the alternate-day gonadotropin regimen of 2 days, the primary and secondary outcomes were comparable between the CC+300 and LTZ+300 groups. However, the number of follicles in size of 11-13 mm on the day of hCG administration was significantly higher in CC+300 group than LTZ+300 group (0.78±1.06 vs. 0.35±0.65, p=0.041). In the alternate gonadotropin regimen of 3 days, although there was no significant difference in the clinical pregnancy rate between the cycles using CC and LTZ, the endometrial thickness was significantly greater in the LTZ+450 group (9.62±1.94 mm vs. 10.14±1.79 mm, p=0.049). The number of follicles in size of 11-13 mm on the day of hCG administration was significantly higher in the CC+450 group than in the LTZ+450 group (0.99±1.34 vs. 0.54±0.89, p=0.009). The pre-preparation TMSC and post-preparation sperm concentrations were significantly higher in the LTZ+450 group than in the CC+450 group (106.12±130.06 vs. 152.57±142.91, p=0.024; 56.15±59.62 mL vs. 103.47±107.14 mL, p<0.001). OHSS was significantly more prevalent in the CC+450 group than in the LTZ+450 (12.4% vs. 1.1%, p=0.002). Finally, the multiple pregnancy rate was significantly higher in the LTZ+450 group than in the CC+450 group (50% vs. 13.3%, p=0.038) (Table 3).
DISCUSSION
The four different regimens in our study showed comparable clinical pregnancy rates per cycle. Minimal stimulation protocols using LTZ resulted in the development of fewer small follicles, with a similar number of medium- to large-sized follicles when compared to those using CC. As a result, the development of OHSS was more prevalent in CC users, especially combined with alternate-day gonadotropin 3 days regimen. Multiple pregnancies were more prevalent in the alternate-day gonadotropin regimen of 3 days, combined with LTZ, but not in the alternate-day gonadotropin regimens of 2 days, neither in combination with CC, nor LTZ.
The clinical pregnancy and multiple pregnancy rates in the current study are comparable to those reported in previous studies.4,15,20,21,22,23,24,25 In large population observational studies26,27 and a randomized controlled trial,4 although the clinical pregnancy rate per cycle was approximately 10% in IUI with gonadotropin only, multiple pregnancies represented 30% of these cases. In other studies, the multiple pregnancy rate after ovulation induction with gonadotropin varies between 5% and 20%.4,23,25,28 In terms of OHSS, few studies have demonstrated the development of OHSS in IUI with controlled ovarian stimulation cycles. In a prospective randomized trial, the cancellation rate was reported based on the OHSS risk, instead of the OHSS development rate in IUI with gonadotropin stimulation (cancellation rate, 1.2% vs. 8.4%, respectively).29 In a prospective randomized study which compared conventional CC/hMG stimulation protocol to minimal stimulation protocol, the incidence of OHSS was 3% in conventional stimulation cycles whereas none of OHSS was developed in minimal stimulation cycles.10 Fewer OHSS cases were observed in our study than in previous studies10,11 of IUI cycles with minimal stimulation.
Interestingly, in our study, multiple pregnancies significantly increased in cycles with the alternate-day regimens of 3 days, in LTZ users. Although it cannot be clearly explained, this significant difference may be due to superovulation by combining gonadotropin and favorable endometrial receptivity by using LTZ without antiestrogenic effect on endometrium. LTZ itself has been suggested to develop less multiple pregnancies in ovulation induction for polycystic ovary syndrome (PCOS) women.30 However, our study showed that superovulation combined with gonadotropin may increase multiple pregnancies. Recently, a large retrospective review of 2929 patients with unexplained infertility showed that increasing number of mature follicles gradually increased multiple pregnancies.31 Furthermore, contrary to CC, LTZ has no antiestrogenic effect on endometrium. Our study showed that minimal stimulation combined with LTZ increased endometrial thickness compared to that combined with CC, which may indicate that the administration of CC cause hostile endometrium due to antiestrogenic effect on endometrium.
The current study showed that OHSS development was significantly lower in the LTZ group, independent of other factors such as endometrial thickness, total amount of gonadotropin, follicular number on the day of hCG administration, or multiple pregnancy (data not shown). Increasing development of OHSS in CC users can result from increased development of small size follicles than LTZ users. Regimens using CC comparing to LTZ in 3 days regimen resulted in significantly increased development of small-sized follicles (11-14 mm) with a similar number of medium- (15-17 mm) to large-sized follicles (≥18 mm); this change may result in increased levels of estradiol and contribute to more development of OHSS. In 2 days regimen, however, difference of small-sized follicles (11-14 mm) between CC and LTZ was not significant, although the actual number was higher in CC group, which might be arised from small number of subjects compared to 3 days regimen. Compared to other studies, however, there are few data showing OHSS development in ovulation induction using for IUI cycles. In a recent systemic review of aromatase inhibitor use in ovulation induction for PCOS women, 9 randomized controlled trials assessed OHSS development between various protocol using LTZ, clomiphene combined with timed intercourse or IUI. The review showed few occurrences of OHSS in most of the studies; only 2 events of OHSS was reported in clomiphene 100 mg group in a study from Indian group. They concluded no evidence for a difference in frequency of OHSS between LTZ and CC with or without adjuncts. However, it is noteworthy that, among the 9 trials, only 3 trials compared the effect of LTZ and clomiphene in ovulation induction for IUI cycle, and adjuncts with gonadotropin was in one trial.30
In the previous studies, LTZ has been shown to be neither superior nor inferior to CC, in terms of outcomes described above;30,32 except reports which have suggested advantages in PCOS patients with CC resistance allowing ovulation induction.33,34 Because of the suggested advantages, though off label, comparable outcomes after ovulation induction of LTZ have led to the use of LTZ as an alternative agent.14,35 To our knowledge, this is the first study demonstrating the superiority of LTZ over CC, in terms of less developed OHSS with comparable pregnancy rate, when administered in combination with gonadotropin in IUI cycle. Although, there was an increased risk of multiple pregnancy rate in LTZ+450 group in the present study, there was no multiple pregnancy in LTZ+300 group. To reduce multiple pregnancy rate, therefore, lower doses of gonadotropin may be preferred in minimal stimulation protocol using LTZ.
Several limitations of the present study should be mentioned. Firstly, since this was a retrospective study and not a randomized controlled trial, a selection bias or confounding factors may influence the results. However, the similarity in baseline clinical characteristics-including age, duration of infertility, and causes of infertility-suggest that the selection bias was minimal. Secondly, the sample size has limited statistical power for any conclusion to be drawn regarding the outcomes among 4 different groups. When a power calculation was performed using PS: Power and Sample size calculation software Version 3.0.43 (http://biostat.mc.vanderbilt.edu/wiki/Main/PowerSampleSize), the sample size has the power of 27.5, 58.9, and 85.5% to detect a significant difference for clinical pregnancy rate, multiple pregnancy rate and the development of OHSS, respectively, between the CC group and the LTZ group. Regarding the development of OHSS, further studies in a larger scale will be necessary to confirm our results, although this study had sufficient power
In conclusion, a minimal stimulation protocol using LTZ combined with alternate-day administration of gonadotropin for 2 days seems to be efficacious for IUI, because it does not affect superovulation and clinical pregnancy rates, while reducing multiple pregnancies and OHSS development.
ACKNOWLEDGEMENTS
This work was supported by a grant from the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (A120043).
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Zegers-Hochschild F, Nygren KG, Adamson GD, de Mouzon J, Lancaster P, Mansour R, et al. The ICMART glossary on ART terminology. Hum Reprod. 2006;21:1968–1970. doi: 10.1093/humrep/del171. [DOI] [PubMed] [Google Scholar]
- 2.Zegers-Hochschild F, Nygren KG, Adamson GD, de Mouzon J, Lancaster P, Mansour R, et al. The International Committee Monitoring Assisted Reproductive Technologies (ICMART) glossary on ART terminology. Fertil Steril. 2006;86:16–19. doi: 10.1016/j.fertnstert.2006.04.018. [DOI] [PubMed] [Google Scholar]
- 3.ESHRE Capri Workshop Group. Intrauterine insemination. Hum Reprod Update. 2009;15:265–277. doi: 10.1093/humupd/dmp003. [DOI] [PubMed] [Google Scholar]
- 4.Guzick DS, Carson SA, Coutifaris C, Overstreet JW, Factor-Litvak P, Steinkampf MP, et al. Efficacy of superovulation and intrauterine insemination in the treatment of infertility. National Cooperative Reproductive Medicine Network. N Engl J Med. 1999;340:177–183. doi: 10.1056/NEJM199901213400302. [DOI] [PubMed] [Google Scholar]
- 5.Hughes EG. The effectiveness of ovulation induction and intrauterine insemination in the treatment of persistent infertility: a meta-analysis. Hum Reprod. 1997;12:1865–1872. doi: 10.1093/humrep/12.9.1865. [DOI] [PubMed] [Google Scholar]
- 6.Cantineau AE, Cohlen BJ, Heineman MJ. Ovarian stimulation protocols (anti-oestrogens, gonadotrophins with and without GnRH agonists/antagonists) for intrauterine insemination (IUI) in women with subfertility. Cochrane Database Syst Rev. 2007:CD005356. doi: 10.1002/14651858.CD005356.pub2. [DOI] [PubMed] [Google Scholar]
- 7.Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R. Risk factors for high-order multiple pregnancy and multiple birth after controlled ovarian hyperstimulation: results of 4,062 intrauterine insemination cycles. Fertil Steril. 2005;83:671–683. doi: 10.1016/j.fertnstert.2004.10.030. [DOI] [PubMed] [Google Scholar]
- 8.Ragni G, Caliari I, Nicolosi AE, Arnoldi M, Somigliana E, Crosignani PG. Preventing high-order multiple pregnancies during controlled ovarian hyperstimulation and intrauterine insemination: 3 years' experience using low-dose recombinant follicle-stimulating hormone and gonadotropin-releasing hormone antagonists. Fertil Steril. 2006;85:619–624. doi: 10.1016/j.fertnstert.2005.09.021. [DOI] [PubMed] [Google Scholar]
- 9.Ghesquiere SL, Castelain EG, Spiessens C, Meuleman CL, D'Hooghe TM. Relationship between follicle number and (multiple) live birth rate after controlled ovarian hyperstimulation and intrauterine insemination. Am J Obstet Gynecol. 2007;197:589. doi: 10.1016/j.ajog.2007.05.016. [DOI] [PubMed] [Google Scholar]
- 10.Dhaliwal LK, Sialy RK, Gopalan S, Majumdar S. Minimal stimulation protocol for use with intrauterine insemination in the treatment of infertility. J Obstet Gynaecol Res. 2002;28:295–299. doi: 10.1046/j.1341-8076.2002.00058.x. [DOI] [PubMed] [Google Scholar]
- 11.Sengoku K, Tamate K, Takaoka Y, Morishita N, Ishikawa M. A randomized prospective study of gonadotrophin with or without gonadotrophin-releasing hormone agonist for treatment of unexplained infertility. Hum Reprod. 1994;9:1043–1047. doi: 10.1093/oxfordjournals.humrep.a138630. [DOI] [PubMed] [Google Scholar]
- 12.Goverde AJ, Lambalk CB, McDonnell J, Schats R, Homburg R, Vermeiden JP. Further considerations on natural or mild hyperstimulation cycles for intrauterine insemination treatment: effects on pregnancy and multiple pregnancy rates. Hum Reprod. 2005;20:3141–3146. doi: 10.1093/humrep/dei175. [DOI] [PubMed] [Google Scholar]
- 13.Ryan GL, Moss V, Davis WA, Sparks AE, Dokras A, Van Voorhis BJ. Oral ovulation induction agents combined with low-dose gonadotropin injections and intrauterine insemination: cost- and clinical effectiveness. J Reprod Med. 2005;50:943–950. [PubMed] [Google Scholar]
- 14.Badawy A, Elnashar A, Totongy M. Clomiphene citrate or aromatase inhibitors combined with gonadotropins for superovulation in women undergoing intrauterine insemination: a prospective randomised trial. J Obstet Gynaecol. 2010;30:617–621. doi: 10.3109/01443615.2010.497873. [DOI] [PubMed] [Google Scholar]
- 15.Dickey RP, Olar TT, Taylor SN, Curole DN, Rye PH. Sequential clomiphene citrate and human menopausal gonadotrophin for ovulation induction: comparison to clomiphene citrate alone and human menopausal gonadotrophin alone. Hum Reprod. 1993;8:56–59. doi: 10.1093/oxfordjournals.humrep.a137874. [DOI] [PubMed] [Google Scholar]
- 16.Gregoriou O, Vlahos NF, Konidaris S, Papadias K, Botsis D, Creatsas GK. Randomized controlled trial comparing superovulation with letrozole versus recombinant follicle-stimulating hormone combined with intrauterine insemination for couples with unexplained infertility who had failed clomiphene citrate stimulation and intrauterine insemination. Fertil Steril. 2008;90:678–683. doi: 10.1016/j.fertnstert.2007.06.099. [DOI] [PubMed] [Google Scholar]
- 17.Bedaiwy MA, Forman R, Mousa NA, Al Inany HG, Casper RF. Cost-effectiveness of aromatase inhibitor co-treatment for controlled ovarian stimulation. Hum Reprod. 2006;21:2838–2844. doi: 10.1093/humrep/del273. [DOI] [PubMed] [Google Scholar]
- 18.Healey S, Tan SL, Tulandi T, Biljan MM. Effects of letrozole on superovulation with gonadotropins in women undergoing intrauterine insemination. Fertil Steril. 2003;80:1325–1329. doi: 10.1016/j.fertnstert.2003.03.001. [DOI] [PubMed] [Google Scholar]
- 19.Navot D, Bergh PA, Laufer N. Ovarian hyperstimulation syndrome in novel reproductive technologies: prevention and treatment. Fertil Steril. 1992;58:249–261. doi: 10.1016/s0015-0282(16)55188-7. [DOI] [PubMed] [Google Scholar]
- 20.Agarwal SK, Buyalos RP. Clomiphene citrate with intrauterine insemination: is it effective therapy in women above the age of 35 years? Fertil Steril. 1996;65:759–763. doi: 10.1016/s0015-0282(16)58210-7. [DOI] [PubMed] [Google Scholar]
- 21.Lu PY, Chen AL, Atkinson EJ, Lee SH, Erickson LD, Ory SJ. Minimal stimulation achieves pregnancy rates comparable to human menopausal gonadotropins in the treatment of infertility. Fertil Steril. 1996;65:583–587. doi: 10.1016/s0015-0282(16)58158-8. [DOI] [PubMed] [Google Scholar]
- 22.Brzechffa PR, Buyalos RP. Female and male partner age and menotrophin requirements influence pregnancy rates with human menopausal gonadotrophin therapy in combination with intrauterine insemination. Hum Reprod. 1997;12:29–33. doi: 10.1093/humrep/12.1.29. [DOI] [PubMed] [Google Scholar]
- 23.Bhattacharya S, Templeton A. In treating infertility, are multiple pregnancies unavoidable? N Engl J Med. 2000;343:58–60. doi: 10.1056/NEJM200007063430110. [DOI] [PubMed] [Google Scholar]
- 24.Stewart JA. Stimulated intra-uterine insemination is not a natural choice for the treatment of unexplained subfertility. Should the guidelines be changed? Hum Reprod. 2003;18:903–907. doi: 10.1093/humrep/deg237. [DOI] [PubMed] [Google Scholar]
- 25.Fauser BC, Devroey P, Macklon NS. Multiple birth resulting from ovarian stimulation for subfertility treatment. Lancet. 2005;365:1807–1816. doi: 10.1016/S0140-6736(05)66478-1. [DOI] [PubMed] [Google Scholar]
- 26.Gleicher N, Oleske DM, Tur-Kaspa I, Vidali A, Karande V. Reducing the risk of high-order multiple pregnancy after ovarian stimulation with gonadotropins. N Engl J Med. 2000;343:2–7. doi: 10.1056/NEJM200007063430101. [DOI] [PubMed] [Google Scholar]
- 27.Tur R, Barri PN, Coroleu B, Buxaderas R, Martínez F, Balasch J. Risk factors for high-order multiple implantation after ovarian stimulation with gonadotrophins: evidence from a large series of 1878 consecutive pregnancies in a single centre. Hum Reprod. 2001;16:2124–2129. doi: 10.1093/humrep/16.10.2124. [DOI] [PubMed] [Google Scholar]
- 28.Ombelet W, De Sutter P, Van der Elst J, Martens G. Multiple gestation and infertility treatment: registration, reflection and reaction-- the Belgian project. Hum Reprod Update. 2005;11:3–14. doi: 10.1093/humupd/dmh048. [DOI] [PubMed] [Google Scholar]
- 29.Sagnella F, Moro F, Lanzone A, Tropea A, Martinez D, Capalbo A, et al. A prospective randomized noninferiority study comparing recombinant FSH and highly purified menotropin in intrauterine insemination cycles in couples with unexplained infertility and/or mild-moderate male factor. Fertil Steril. 2011;95:689–694. doi: 10.1016/j.fertnstert.2010.08.044. [DOI] [PubMed] [Google Scholar]
- 30.Franik S, Kremer JA, Nelen WL, Farquhar C. Aromatase inhibitors for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2014;2:CD010287. doi: 10.1002/14651858.CD010287.pub2. [DOI] [PubMed] [Google Scholar]
- 31.Wolff EF, Vahidi N, Alford C, Richter K, Widra E. Influences on endometrial development during intrauterine insemination: clinical experience of 2,929 patients with unexplained infertility. Fertil Steril. 2013;100:194–199. doi: 10.1016/j.fertnstert.2013.03.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lee VC, Ledger W. Aromatase inhibitors for ovulation induction and ovarian stimulation. Clin Endocrinol (Oxf) 2011;74:537–546. doi: 10.1111/j.1365-2265.2011.04006.x. [DOI] [PubMed] [Google Scholar]
- 33.McKnight KK, Nodler JL, Cooper JJ, Jr, Chapman VR, Cliver SP, Bates GW., Jr Body mass index-associated differences in response to ovulation induction with letrozole. Fertil Steril. 2011;96:1206–1208. doi: 10.1016/j.fertnstert.2011.08.002. [DOI] [PubMed] [Google Scholar]
- 34.Ganesh A, Goswami SK, Chattopadhyay R, Chaudhury K, Chakravarty B. Comparison of letrozole with continuous gonadotropins and clomiphene-gonadotropin combination for ovulation induction in 1387 PCOS women after clomiphene citrate failure: a randomized prospective clinical trial. J Assist Reprod Genet. 2009;26:19–24. doi: 10.1007/s10815-008-9284-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Barroso G, Menocal G, Felix H, Rojas-Ruiz JC, Arslan M, Oehninger S. Comparison of the efficacy of the aromatase inhibitor letrozole and clomiphene citrate as adjuvants to recombinant follicle-stimulating hormone in controlled ovarian hyperstimulation: a prospective, randomized, blinded clinical trial. Fertil Steril. 2006;86:1428–1431. doi: 10.1016/j.fertnstert.2006.03.044. [DOI] [PubMed] [Google Scholar]