

Abstract
Background
Heavy drinking is common during transitions from high school to college. Optimal programs for diminishing risks for high alcohol consumption often tailor the approach to the specific needs of students. This paper describes the results of an Internet-based prevention protocol that tailors the information to the risk associated with a preexisting phenotype, the Low level of Response (Low LR) to alcohol.
Methods
Using stratified random assignment, 454 freshmen with Low and High LR values were assigned to two education groups (LR-Based where all examples were given the context of the Low LR model of heavy drinking, or a State of the Art Group where the same lessons were taught but without an emphasis on LR) or a no-intervention Control Group. Individuals in the two education groups viewed 50-minute online videos once per week for four weeks. Changes in drinking patterns were assessed at Baseline, 4 weeks, and 8 weeks using a 2 (LR status) by 3 (education group) by 3 (time points) ANOVA, with additional tests for ethnicity and sex.
Results
Low LR participants tended to decrease their usual (p<.06) and maximum (p<.05) drinks per occasion most prominently when assigned to the LR-Based protocol, while those with High LRs improved more in the State Of The Art Group. The most robust differences were seen when controlling for ethnicity. The effect sizes were small to medium.
Conclusions
These results support the advantages of carrying out prevention via the Internet and in tailoring the approach to a preexisting phenotype.
Introduction
The transition from home to college is a time when alcohol consumption is likely to rapidly increase (Fromme et al., 2008; Johnston et al., 2013; Mallett et al., 2013). While ∼50% of high school seniors report ever drinking, over 80% of college students consume alcohol, with 54% versus 70% of the two groups reporting having ever been drunk (Johnston et al., 2013). Consistent with prior studies (e.g., Mallett et al., 2013; Polak and Conner, 2012), a recent paper reported that during their first college year 60% of students drank enough to be physically sick, 54% reported blackouts, 37% evidenced drinking behaviors that disappointed other people, and 30% each engaged in regretted romantic behaviors or felt alcohol interfered with schoolwork (Barnett et al., 2014).
The risk for heavier drinking and associated problems is not evenly distributed among drinkers. Generally, males are more likely to have alcohol problems than females (Barnett et al., 2014; Polak and Conner, 2012), and European Americans (EA) and Hispanics consume more alcohol than African Americans (AA) and Asians (Barnett et al., 2014; Eng et al., 2007; Li et al., 2011; Wu et al., 2011). Heavy drinking and associated problems also relate to several aspects of a person's response to alcohol (King et al., 2014; Newlin and Renton, 2010; Schuckit, 2014), including the need for higher blood alcohol concentrations (BACs) to produce a range of effects (Low level of Response, or Low LR, to alcohol) (Quinn and Fromme, 2011; Schuckit et al., 2011a). Low LR best predicts future higher quantities per occasion, with less impact on drinking frequencies (Chung and Martin, 2009; Quinn and Fromme, 2011; Schuckit et al., 2011b, 2012b, 2014; Scott, 2012).
Several additional characteristics that relate to heavier drinking also relate to the Low LR to alcohol. Regarding sex, men have lower LRs per drink than women, and regarding ethnic backgrounds, EA and Hispanic individuals show lower LRs than Asian and AA subjects (Ehlers et al., 2004; Eng et al., 2007; Pederson et al., 2013; Schuckit et al., 2012b).
Our group has been interested in whether enhancing knowledge of Low LR in the usual student entering college might help decrease future heavy drinking. We were guided by a literature indicating that such prevention programs are more effective if lessons are personalized to relate to an individual's attributes, usually focusing on a person's demography and recent drinking patterns (Carey et al., 2007; Conrod et al., 2011; Larimer and Cronce, 2007). Several recent studies also evaluated the effectiveness of tailoring prevention messages to address preexisting phenotypes, including feelings of hopelessness, anxiety sensitivity, impulsivity, or sensation seeking, demonstrating that such personalized interventions were associated with long term lower levels of alcohol and drug involvement (Conrod et al., 2010, 2011, 2013). As suggested by Chinn and Brewer (1993), organizing information around a principle (e.g., how a Low LR impacts on future drinking) with which a person with Low LR identifies might increase the likelihood that the information will be remembered and acted upon.
Our recent prevention efforts have been structured to reach large groups at lower cost to make interventions optimally attractive to administrators. Thus, we turned to Internet-based prevention approaches where, across a range of substances, 4+ sessions in a Web-based format were associated with lower future substance use (Champion et al., 2013; Kypri et al., 2012; Polak and Connor, 2012).
In 2012, our group published a pilot study of 64 freshman to evaluate whether an Internet-based personalized prevention approach that focused on a Low LR to alcohol was effective. We created two sets of four videos, with one set based on the low LR to alcohol (a Low LR-Based [LRB] Group) and the other incorporating more generic State of the Art (SOTA) information without an emphasis on any model of risk. We then compared drinking outcomes over eight weeks in drinking college freshmen (Schuckit et al., 2012a). Similar to procedures described in the Methods below, both LRB and SOTA videos used didactic presentations that incorporated key elements of Motivational Interviewing (MI) and Brief Intervention (BI). Video sets for the two groups differed in that all examples in LRB videos were based on the model of how the impact of a Low LR on heavier drinking operated partly through environmental mediators (e.g., selecting heavier drinking friends) and attitudes (e.g., positive alcohol expectancies) (Schuckit et al., 2011a, 2011b), while examples in SOTA videos focused on negative affect and impulsivity as risk factors as well. Results indicated that, while both Low and High LR subjects diminished drinking in both education groups, those with Low LR decreased quantities more when in the LRB educational protocol, and subjects with High LR demonstrated slightly better outcomes in a SOTA group.
The small number of participants in that protocol highlights the need for testing in larger samples (Scott, 2012). Potential impacts of sex and racial/ethnic group membership on drinking practices and on LR support the need to consider ethnicity and sex while evaluating differential impacts of LRB and SOTA education groups on drinking practices in Low and High LR individuals. This report presents data from a new sample of 500 drinking subjects exposed to similar videos as in the pilot study and evaluated over the same three time points as in the original program. Our goal was to further evaluate a protocol aimed at helping the usual student drinker to minimize heavy alcohol consumption during transition from high school to college. We evaluated three hypotheses: 1) both Low and High LR participants will demonstrate decreases in drinking quantities across eight weeks (i.e., the interventions will do no harm); 2) even after considering changes in drinking for the Control Group as well as race/ethnicity and sex, the Low LR students will show greater decreases in drinking quantities in the LRB Group; and 3) in the context of those same ethnicity and sex considerations, consistent with the pilot results, participants with High LR will show greater drinking decreases in the SOTA Group.
Methods
Subjects
The protocol, approved by the University of California, San Diego (UCSD) Human Protections Committee, began with a Campus Questionnaire emailed to all (∼4,000) entering freshmen. They were paid $10 to answer items adapted from the Semi-Structured Assessment for the Genetics of Alcoholism (SSAGA) interview. These covered demography, drinking and drug use patterns, and related diagnoses from the Fourth Diagnostic and Statistical Manual of the American Psychiatric Association (DSM-IV) (American Psychiatric Association, 1994). The SSAGA has repeat reliabilities and validities compared to additional instruments of ∼.80 (Bucholz et al., 1994; Hesselbrock et al., 1999). Respondents were considered for the next study phase if they had consumed alcohol in the prior month, never met criteria for alcohol or drug dependence, had no major medical problems, and were not taking medications that could affect their response to alcohol. They also answered questions from the Self-Rating of the Effects of Alcohol (SRE) instrument measuring LR as the average number of drinks for up to four effects (initial feeling any effect of alcohol, slurring speech, stumbling, and unwanted falling asleep) during the approximate first five times of drinking (SRE First 5) (Schuckit et al., 2011b). The SRE instrument has a one-year repeat reliability of .66 (Ray et al., 2007), and Cronbach α of 0.88 in the current sample.
Using an SRE median split, the student with the lowest LR was identified and a high LR participant with the same sex and similar ethnicity and recent alcohol quantities and frequencies was selected. With >80% of eligible students agreeing to participate, the process continued until 500 individuals were enrolled. As <2% of UCSD students are AAs and smaller proportions are Malay, Filipino, Middle Eastern or other minorities, these subjects were sometimes matched with participants of different minority ethnicities. High and Low LR pairs were randomly assigned to the LRB, SOTA, and Control Groups stratified by sex, alcohol quantities and frequencies, and ethnicity, with fewer assigned as controls to optimize power for comparisons of outcomes for LRB and SOTA groups.
Interventions
At Baseline (Week 1), all subjects were paid $20 for Assessment Questionnaires (and $20 for each additional assessment) regarding prior month alcohol-related items. After completing the assessment, subjects in the two video groups (paid $20 for each video) accessed a 50-minute video on a secure Website and answered questions addressing comprehension of the major points presented. That process for videos was repeated each week for the first month, and in Week 4 participants in all three groups completed their second Assessment Questionnaire, which for video groups was only available after watching Video 4. At Week 8, subjects in all three groups completed their third paid assessment regarding prior month alcohol use.
The four LRB and four SOTA videos were the same didactic lectures delivered by Dr. Schuckit in the pilot study (Schuckit et al., 2012a), and included animated PowerPoint slides to emphasize his major points. Each video incorporated MI and BI techniques by using a non-dogmatic approach to emphasize that each student needed to make their own decisions about drinking, their personal responsibility for change, and discussing assets and liabilities of drinking practices. The videos also offered feedback on the risks of consuming >three drinks per occasion, discussed the importance of accurate expectations of alcohol's effects, offered a menu of options regarding ways to decrease drinking, reiterated each student's ability to change, and helped students set realistic goals for altering drinking behaviors (Carey et al., 2007; Larimer and Cronce, 2007). Videos defined standard drinks and their relationship to BACs, presented a menu of ways to refuse drinks (Borsari and Carey, 2001), presented accurate data about UCSD dinking practices (Borsari and Carey, 2003; Neighbors et al., 2007), and offered healthy ways to identify and cope with stress (King and Chassin, 2008). Individualized feedback was incorporated by asking subjects to write down answers to questions earlier in the video (e.g., the average number of drinks per occasion for UCSD students), and telling them the correct answers later in the video.
LRB and SOTA videos differed in that while a range of risk factors for heavy drinking was discussed for each group, LRB Group examples focused on the LR-based model of how Low LR related to peer pressures, alcohol expectancies, stress, and drinking to cope to produce heavier alcohol use (e.g., Schuckit et al., 2011a). The SOTA videos also offered a range of examples to demonstrate the points made, but did not emphasize the LR-based model.
Analyses
For each outcome (maximum and usual quantities, usual frequencies, and frequency of consuming 4+ drinks), we performed a 2 LR group by 3 education group by 4 racial/ethnic group (EA, Asian, White Hispanic, and “others”) by 3 time-point mixed design ANOVA, with time as the repeated measure, including an evaluation of the LR by education group by time 3-way interaction. Four- and 3-way interactions regarding LR by education groups by sex by time were also conducted. Race/ethnicity and sex were included in the 4-way ANOVAs because both LR and alcohol use patterns can differ across these subgroups, and two separate evaluations were done rather than one 5-way analysis to optimize interpreting results while avoiding extremely small cells. Linear contrasts were used because, consistent with our prior approaches (Schuckit et al., 2012a), we projected linear decreases in alcohol use over time. Data were evaluated using log transformations because of the skewed distributions often seen with alcohol-related data where many subjects have low scores and fewer report high values. SPSS multiple imputation was used for the 4 subjects with some missing data. Effect sizes were determined using partial eta squared (np2).
Results
Subjects
As shown in Figure 1, among the 2,892 subjects responding to the Campus Questionnaire, 1,107 met eligibility criteria, and the 500 who agreed to participate represented ∼80% of those asked. Among these, 23 (4.6%) were subsequently dropped from the protocol because: 17 agreed to do the study but did no assessments or videos; 3 did Assessment 1 but watched no videos; and 3 did Assessment and Video 1 but had no additional participation. Deleting these individuals and their matches left 454 subjects.
Figure 1.

Flow chart illustrating recruitment, assignment to Level of Response Based (LRB), State Of The Art (SOTA) or Control groups, and study task completion.
* Although 10 participants in the SOTA did not complete study tasks, two participants were in the same pair, this resulted in the deletion of 9 pairs for the analyses.
+Note that while 477 subjects completed the 8 week protocol, after deleting the 23 additional subjects who were matched to the 23 dropouts, 454 participants were used in the analyses (227 matched pairs).
Table 1 presents demographic, alcohol, and drug backgrounds across six groups at baseline (Low and High LR subjects in three education groups). Statistical evaluations are given at the right side of the table for overall results across all six conditions, as well as for Low LRs across the three education groups and High LRs across those groups. There were no significant differences for demographic characteristics. By definition, SRE scores were different across the six groups, as were drinking quantities, but for these variables Low LR subjects were similar across the three education groups, as was the case for those with High LR. There were no differences for two other characteristics that have been reported in the literature to relate to future drinking, Baseline tobacco smoking and cannabis use.
Table 1. Demography, Alcohol, and Drug Characteristics at Time 1 Across the 3 Experimental Conditions for 454 Subjects*.
| Education Group | LRB | SOTA | CONTROL | Overall | Low LR | High LR | |||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| LR (Group) | Low LR | High LR | Low LR | High LR | Low LR | High LR | F/χ2 | F/χ2 | F/χ2 |
|
| |||||||||
| N | 89 | 89 | 106 | 106 | 32 | 32 | |||
|
| |||||||||
| Demography | |||||||||
|
| |||||||||
| Age | 18.1 (0.41) | 18.2 (0.49) | 18.1 (0.36) | 18.2 (0.52) | 18.1 (0.44) | 18.2 (0.62) | 0.77 | 0.19 | 0.48 |
|
| |||||||||
| Female (%) | 65.2 | 65.2 | 58.5 | 58.5 | 65.6 | 65.6 | 2.22 | 1.11 | 1.11 |
|
| |||||||||
| Race/Ethnicity (%) | 5.36 | 2.56 | 2.68 | ||||||
| EA | 23.6 | 23.6 | 27.4 | 27.4 | 28.1 | 28.1 | |||
| Asian | 31.5 | 31.5 | 32.1 | 30.2 | 25.0 | 25.0 | |||
| Hispanic | 12.4 | 12.4 | 11.3 | 13.2 | 6.3 | 6.3 | |||
| Other | 32.6 | 32.6 | 29.2 | 29.2 | 40.6 | 40.6 | |||
|
| |||||||||
| Dormitory residence (%) | 94.4 | 92.3 | 93.4 | 93.4 | 93.8 | 87.5 | 1.91 | 0.08 | 1.17 |
|
| |||||||||
| Alcohol | |||||||||
|
| |||||||||
| SRE 1st 5 | 6.0 (1.82) | 2.5 (0.82) | 5.8 (1.79) | 2.5 (0.81) | 5.5 (1.89) | 2.8 (0.68) | 124.57c | 0.86 | 1.69 |
|
| |||||||||
| Maximum quantityˆ | 7.4 (4.45) | 5.6 (4.45) | 7.1 (4.71) | 5.5 (4.06) | 8.4 (6.23) | 5.2 (4.15) | 4.20c | 0.94 | 0.11 |
|
| |||||||||
| Usual quantityˆ | 5.0 (3.08) | 3.6 (2.52) | 4.7 (2.94) | 3.6 (2.36) | 5.0 (4.07) | 3.1 (2.38) | 5.00c | 0.24 | 0.07 |
|
| |||||||||
| Usual frequencyˆ | 4.6 (4.47) | 3.7 (3.62) | 4.5 (4.97) | 4.1 (3.90) | 5.1 (4.43) | 4.7 (4.33) | 0.81 | 0.25 | 0.93 |
|
| |||||||||
| Times 4+ drinksˆ | 2.8 (2.90) | 2.3 (2.77) | 2.5 (2.51) | 2.1 (2.75) | 3.2 (3.02) | 2.1 (2.42) | 1.29 | 0.74 | 0.10 |
|
| |||||||||
| Drugs (%) | |||||||||
|
| |||||||||
| Smoke 5+ 6mo (%) | 9.0 | 4.5 | 3.8 | 4.7 | 0.0 | 12.5 | 7.86 | 4.70 | 3.17 |
|
| |||||||||
| Cannabis | 53.9 | 39.3 | 38.7 | 38.7 | 43.8 | 46.9 | 6.64 | 4.58 | 0.72 |
|
| |||||||||
| Participation | |||||||||
|
| |||||||||
| All 4 assessments (%) | 97.8 | 98.9 | 100.0 | 99.1 | 100.0 | 100.0 | 3.48 | 3.13 | 0.35 |
|
| |||||||||
| Number assessments | 2.98 (0.15) | 2.99 (0.11) | 3.00 (0.00) | 2.99 (0.10) | 3.00 (0.00) | 3.00 (0.00) | 0.69 | 1.57 | 0.17 |
|
| |||||||||
| Number videos | 3.92 (0.34) | 3.97 (0.18) | 3.99 (0.10) | 3.98 (0.14) | 2.10 | 3.91a | 0.42 | ||
|
| |||||||||
| Viewing minutes mean | 47.8 (7.95) | 48.0 (6.89) | 49.2 (14.10) | 50.9 (8.73) | 1.98 | 0.69 | 6.37a | ||
|
| |||||||||
| Viewed all 4 videos (%) | 94.4 | 96.6 | 99.1 | 98.1 | 4.34 | 3.54 | 0.43 | ||
|
| |||||||||
| Correct post-video items (of 18) | 16.3 (2.20) | 16.7 (1.44) | 17.0 (1.19) | 17.1 (2.22) | 2.93a | 4.14a | 3.45 | ||
LRB = Low Response Based Education Group, SOTA = State of the Art Education Group, Control = no videos education group, Low LR/High LR = Subjects classified as having low vs. high level of response to alcohol, EA = European Americans, SRE = Self-Report of the Effects of Alcohol, frequency = # days drank in last month, usual quantity = # drinks usually had in 24 hours in the last month, maximum quantity = largest # of drinks in 24 hours in the last month
= analyses used log transformations
p<.05;
p<.01;
p<.001
Protocol Participation for the 454 Subjects
Table 1's lower segment describes study task participation for relevant groups. The numbers completing all three assessments (98% to 100%) were similar across relevant groups, as were proportions of Low and High LR subjects who watched all four videos (94% to 99%). There were small, but significant, differences among Low or among High LR participants for the average number of videos watched, average minutes spent per video, and number of correct answers to post-video questions. Slightly fewer videos were watched by Low LR subjects in the LRB Group, which could have diminished the impact of videos on their outcomes. However, these differences could not be used as covariates in the following analyses when the outcome evaluations included Controls, as none of those subjects were assigned videos.
Outcomes
Table 2 presents raw data for Baseline, 4 week and 8 week Assessments of prior month usual and maximum drinking quantities, usual frequencies, and frequencies of consuming 4+ drinks per occasion for the 454 subjects in the six groups. Regarding Hypothesis 1, among the 24 cells in the table (the six groups across the four outcomes), all cells demonstrated decreases or no change in drinking parameters from Baseline to 4 and/or 8 weeks. Thus, there was no evidence that the protocol harmed participants.
Table 2. Prior Month Drinking Characteristics across the 3 Assessments for 454 Low and High LR Subjects in the 3 Education Groups (Means and SD).
| Education Group | LRB | SOTA | CONTROL | |||
|---|---|---|---|---|---|---|
|
| ||||||
| LR Group | Low | High | Low | High | Low | High |
|
| ||||||
| N | 89 | 89 | 106 | 106 | 32 | 32 |
|
| ||||||
| Maximum quantity | ||||||
|
| ||||||
| Baseline | 7.4 (4.45) | 5.5 (4.27) | 7.0 (4.49) | 5.6 (4.04) | 8.2 (5.71) | 5.2 (4.15) |
| 4 week | 6.2 (4.94) | 4.8 (3.39) | 6.1 (4.07) | 5.0 (4.05) | 6.7 (5.50) | 4.6 (4.18) |
| 8 week | 5.8 (4.37) | 4.7 (3.6) | 5.7 (4.26) | 4.5 (3.69) | 7.3 (6.02) | 4.4 (4.08) |
|
| ||||||
| Usual quantity | ||||||
| Baseline | 5.0 (3.08) | 3.4 (2.52) | 4.7 (2.94) | 3.6 (2.36) | 5.0 (4.07) | 3.5 (2.38) |
| 4 week | 4.0 (2.81) | 3.4 (2.50) | 4.2 (2.70) | 3.3 (2.55) | 4.1 (2.90) | 3.3 (2.91) |
| 8 week | 3.9 (2.48) | 3.5 (2.75) | 4.0 (2.83) | 3.2 (2.58) | 5.0 (4.12) | 3.5 (3.35) |
|
| ||||||
| Usual frequency | ||||||
| Baseline | 4.6 (4.59) | 3.7 (3.62) | 4.4 (4.35) | 4.1 (3.90) | 5.1 (4.43) | 4.7 (4.33) |
| 4 week | 3.6 (4.04) | 3.3 (2.67) | 3.6 (3.73) | 3.0 (2.88) | 4.3 (4.37) | 3.8 (4.00) |
| 8 week | 3.8 (3.69) | 3.1 (2.62) | 3.7 (3.64) | 3.1 (3.85) | 3.8 (3.19) | 3.2 (2.78) |
|
| ||||||
| 4+ times/occasion | ||||||
| Baseline | 2.8 (2.90) | 2.3 (2.77) | 2.5 (2.51) | 2.1 (2.75) | 3.2 (3.02) | 2.1 (2.42) |
| 4 week | 2.3 (2.78) | 1.7 (2.01) | 2.3 (2.39) | 1.7 (2.09) | 2.6 (3.52) | 1.6 (2.56) |
| 8 week | 2.4 (3.00) | 1.7 (1.91) | 2.3 (2.59) | 1.7 (2.26) | 2.8 (2.48) | 1.7 )2.39) |
Abbreviations are described in the footnote for Table 1
Table 2 data are also illustrated in Figures 2 and 3 for maximum quantities, as well as Figures 4 and 5 for usual quantities. Those figures are heuristic and visually represent data from Table 2 and the statistical analyses in Table 3. Because of Baseline differences across groups for some drinking parameters (see Table 1), Figures 2-5 are given as percent changes from Baseline, but the statistical analyses in Table 3 are based on the log transformations of values in Table 2.
Figure 2.
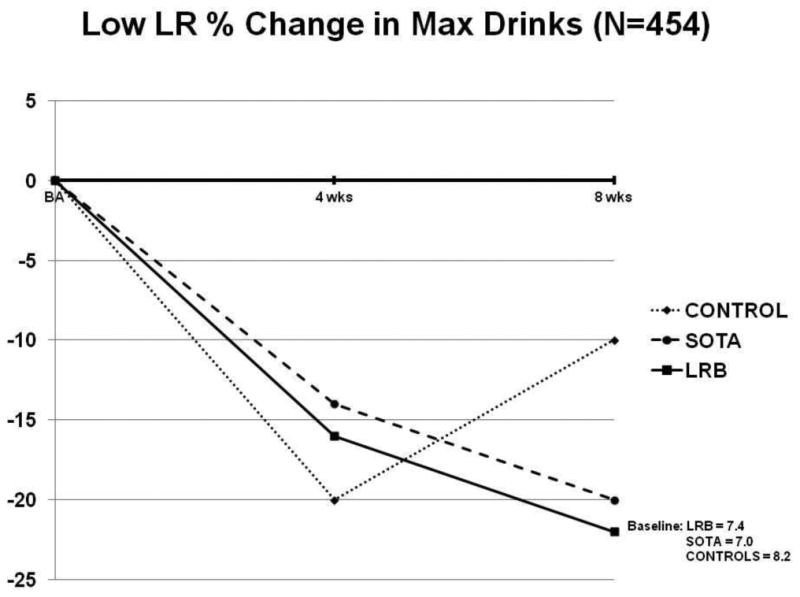
Percentage change in maximum drinks per occasion among low LR drinkers in the Control, State Of The Art (SOTA), and Level of Response Based (LRB) groups from Baseline to 4 and 8 weeks.
Figure 3.
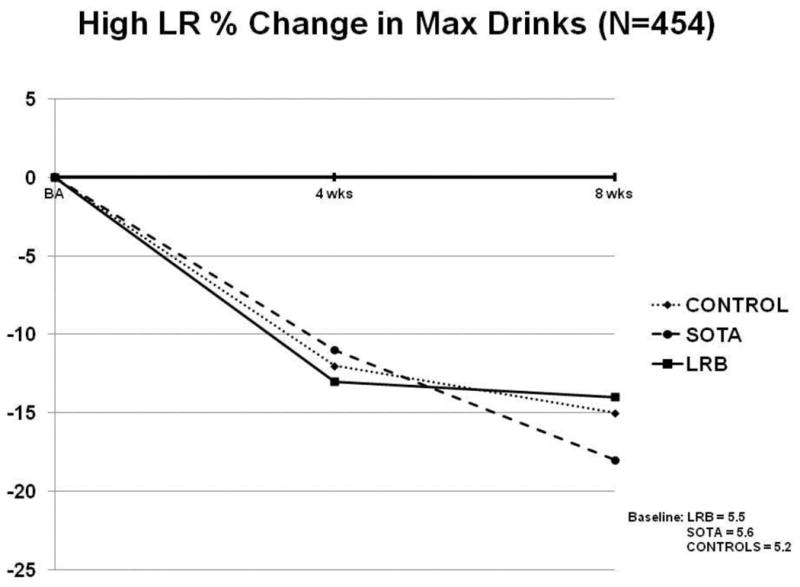
Percentage change in maximum drinks per occasion among high LR drinkers in the Control, State Of The Art (SOTA), and Level of Response Based (LRB) groups from Baseline to 4 and 8 weeks.
Figure 4.
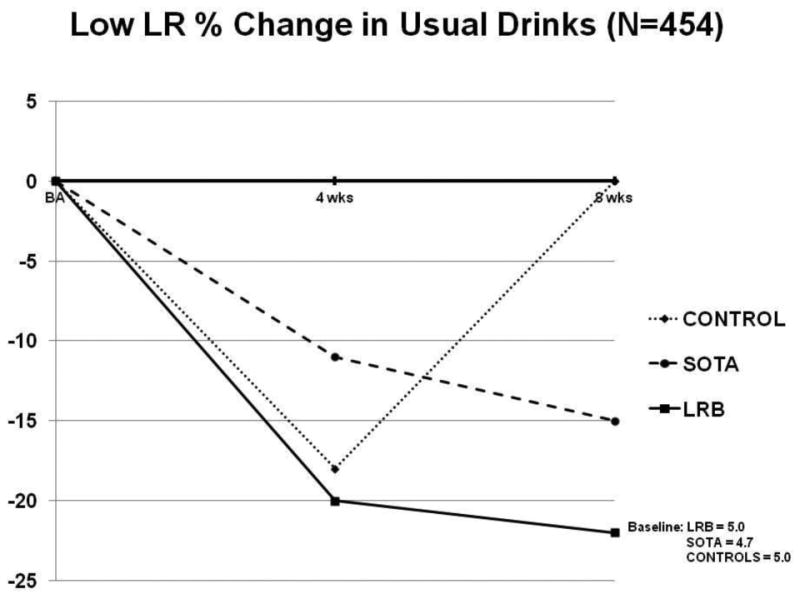
Percentage change in usual drinks per occasion among low LR drinkers in the Control, State Of The Art (SOTA), and Level of Response Based (LRB) groups from Baseline to 4 and 8 weeks.
Figure 5.
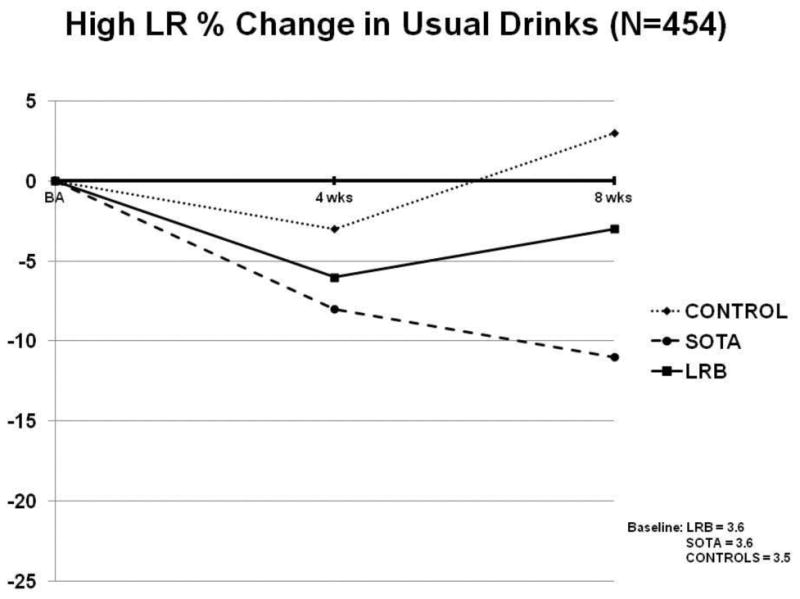
Percentage change in usual drinks per occasion among high LR drinkers in the Control, State Of The Art (SOTA), and Level of Response Based (LRB) groups from Baseline to 4 and 8 weeks.
Table 3.
Four-way and 3-way Interactions and main effects for mixed-model ANOVA with Time as the Repeated Measure for 454 Subjects (F value and significance level)
| 4-way Interaction (df=6,430)* | 3-way Interaction df=(2,430)** | Main Effects | ||||
|---|---|---|---|---|---|---|
| LR (df=1,430) | Education Group(df=2,430) | Race/Ethnicity (df=3,430) | Time (df=1,0) | |||
| Maximum quantity | 2.17 a, .03 | 3.20 a, .02 | 6.10 a, .01 | 0.06 | 9.45 c, .06 | 19.78 c, .04 |
| Usual quantity | 1.92 x, .03 | 2.86 x, .01 | 5.48 a, .01 | 0.76 | 7.66 c, .05 | 9.15 b, .02 |
| Usual frequency | 1.03 | 1.52 | 0.99 | 0.99 | 9.28 c, .06 | 16.72 c, .06 |
| Times 4+ drinks/occasion | 1.29 | 0.28 | 6.68 b, .02 | 0.92 | 11.18 c, .03 | 16.16 c, .04 |
LR × Education Group × Race/Ethnicity × Time
LR × Education Group × Time
p-values are given as superscripts in the table (a = <.05, b = <.01, c = <.001, x = p-values .06 to .08)
partial eta squared effect sizes (ηp2) are described in Table 3
Table 3 addresses Hypotheses 2 and 3 regarding interactions between LR status and education group for drinking parameters over time. The table demonstrates statistically significant results for maximum drinks per occasion for both 4-way (2 LR status × 3 education groups × 4 ethnicity groups × 3 time points) and for the key 3-way (LR × education groups × time) interactions, with np2 between small and medium. As visually demonstrated in Figure 2, Low LR subjects in the LRB Group had a greater decrease over time from Baseline to follow up for maximum drinks compared to those in the SOTA Group. While Low LRs in the Control Group also decreased maximum quantities at four weeks, their values returned toward Baseline levels at eight weeks. High LR subjects in Figure 3 demonstrated decreases in maximum drinks in all 3 education groups, with a bit greater decrease at 8 weeks when in the SOTA Group.
The significance levels for 4-way (p =.08) and 3-way (p =.06) interactions for usual drinks were trends in Table 3. However, considering the relationship of usual drinks to LR in prior studies, these data are graphed in Figure 4 for Low LRs and Figure 5 for High LRs. Once again potential LR group differences by education group by time were most obvious for Low LR subjects, indicating greater change when assigned to the LRB Education Group. High LR subjects in Figure 5 demonstrated a pattern of potential greater decreases from Baseline in the SOTA Group.
Thus, Table 3 shows major results for this study and Figures 2 – 5 visually demonstrate patterns of change over time. However, Table 3 indicates significant (p <.001) main effects for ethnicity for all four drinking outcomes. The consistent importance of ethnicity regarding outcomes and the ethnic differences in drinking practices and regarding LR discussed in the Introduction prompted us to re-review the adequacy of ethnic matches across Low and High LR pairs. This revealed ideal ethnic matches for 308 subjects, but demonstrated that smaller ethnic groups (e.g., AA, Filipino, Pacific South Islanders, Middle Eastern and Native American subjects) were often matched with other ethnic groups within the heterogeneous “other” category, and that some White Hispanic subjects had been matched with EA individuals to optimize baseline matching on the quantity and frequency variables also used as outcomes. Thus, it was necessary to determine if these sub-optimally matched subjects may have affected the data in Table 3 (i.e., if those results were spurious). Therefore, Table 4 repeats the analyses from Table 3, but is limited to the 308 optimally ethnically matched individuals. Results in Table 4 are similar to Table 3, showing significant LR × education group × time interactions for both maximum and usual drinks, with between small and medium np2.
Table 4.
Four-way and 3-way Interactions and main effects for mixed-model ANOVA with Time as the Repeated Measure for 308 Well-Matched Subjects on Ethnicity (F value and significance level)
| 4-way Interaction (df=4,290)* | 3-way Interaction df=(2,290)** | Main Effects | ||||
|---|---|---|---|---|---|---|
| LR (df=1,290) | Education Group(df=2,290) | Race/Ethnicity (df=2,290) | Time (df=1,290) | |||
| Maximum quantity | 1.76 | 4.51 a, .03 | 2.26 | 0.12 | 12.26 c, .08 | 13.36 c, .04 |
| Usual quantity | 1.88x | 3.79 a, .02 | 2.69 | 0.15 | 9.91 c, .06 | 6.36 b, .02 |
| Usual frequency | 0.82 | 1.98 | 0.08 | 0.99 | 9.28 c, .06 | 16.72 c, .06 |
| Times 4+ drinks/occasion | 0.11 | 1.21 | 3.63 x, .01 | 0.32 | 16.22 c, .10 | 13.66 c, .04 |
Another concern regarding Tables 3 and 4 is that it is possible the 3-way interactions were carried primarily by outcomes for Controls. Therefore, analyses in Table 4 were repeated for the 270 subjects after excluding 38 Controls. These 3-way interactions remained significant for maximum drinks (F[1,258]=4.69, p<.05, np2= .02), with a trend for usual drinks (F[1,258]=3.34, p<.07, np2= .01). To further evaluate three-way interactions for maximum drinks for these subjects, analyses were performed regarding group-by-time interactions within the 135 low LR subjects (F[1,133]=3.95, p<.05, np2 =.03) and within 135 high LRs (F[1,133]=1.66,p=.20, np2 =.01). We also evaluated changes over time within the 60 low LRs in the LRB (F[1,59]=18.87, p<.001, np2 =.24) and the 75 low LRs in SOTA (F[1,74]=4.87,p=.03, np2 =.06), as well as the 60 high LRs in the LRB (F[1,59]=0.65, p<.43, np2 =.01), and the 75 high LRs in SOTA (F[1,74]=8.23,p<.01, np2 =.10).
While ethnicity proved to be an important element in these analyses, we were also concerned about the possible impact of sex on the results. Thus, 4-way analyses similar to those regarding ethnicity were performed regarding sex. Here, no significant within group effects were found for 4- or 3-way interactions (LR by education group by time). There were main between-group effects for LR [df=1,442] regarding: frequency (F=4.47, p<.05, np2= .01); usual quantity (F=13.95, p<.001, np2=.03); maximum quantity (F=16.57, p<.001, np2=.04); and 4+ drinks per occasion (F=15.47, p<.001,np2=.03), although no main between-group effects were seen for either sex or education group.
Finally, while mechanisms through which Low LR subjects improved more in the LRB than the SOTA Group are complex, we examined data regarding whether Low LR subjects changed how they rated themselves on a 5-point scale of self-perceived alcohol sensitivity (very sensitive, somewhat sensitive, neutral, somewhat insensitive, very insensitive) from before Video 1 to after Video 4. The proportion of Low LRs in the LRB Group who rated themselves as somewhat or very insensitive at Baseline was 18.0%, and that proportion increased to 37.1% (McNamar Change Test p <.001). However, no similar change was observed for the Low LR subjects in the SOTA (31.2% to 29.2%, p =.84) or Control Group (31.2% to 28.1%, p =1.00).
Discussion
This paper describes results of an Internet-based, relatively inexpensive to run and easily implemented approach for diminishing drinking quantities in college freshmen by tailoring messages to a preexisting phenotype, the Low LR to alcohol. With only 23 participants dropping out over the eight weeks, even after deleting their matched pair from these analyses data from >90% of participants demonstrated that students with Low and High LRs decreased their maximum drinks per occasion. Those with Low LRs diminished their maximum drinks more when in an education protocol that taught drinking-related lessons by emphasizing the model of how a low LR contributes to heavy alcohol intake.
The results support all three original hypotheses. Regarding Hypotheses 1, recognizing that any intervention could do harm, the data in Table 2 and the main time effect in Table 3 indicate that drinking levels decreased over time or remained unchanged for all six LR status by education group pairings. Regarding Hypothesis 2, the predicted pattern of greater decreases in heavy drinking for Low LR participants in the LRB Group was observed, with statistical significance remaining even when considering racial/ethnic backgrounds. This conclusion was supported in Table 3 by the 3-way interactions for LR by education group by time for maximum quantities, and a trend (p=.06) for usual quantities. The Hypothesis 3 prediction that High LR students would decrease drinking more in the SOTA Group was also consistent with the results, perhaps because predispositions toward heavy drinking by High LRs may relate to risk factors other than Low LR (e.g., impulsivity or negative affect), and these predispositions may have been easier for students to identify with in the SOTA Group where those issues were discussed more extensively.
Consistent with our prior studies of LR and our predictions of differential results for frequency versus quantity, few significant effects were seen for drinking frequencies. The effect of LR is primarily on how much one drinks per occasion, rather than on whether a person decides to drink at a specific time (Chung and Martin, 2009; Quinn and Fromme, 2011; Schuckit et al., 2011b, 2012b, 2014; Scott, 2012).
The impact of ethnicity is important to recognize. This variable was emphasized because higher LRs are seen in Asians and AA individuals and lower values in EA and Hispanic subgroups (Ehlers et al., 2004; Eng et al., 2007; Pederson et al., 2013; Schuckit et al., 2012b), and rates of heavy drinking and alcohol problems are higher in EA and Hispanic groups and lower in Asians and AAs (Barnett et al., 2014; Eng et al., 2007; Li et al., 2011). The role of race/ethnicity in the current work was supported by interactions for maximum and usual quantities, and the significant ethnicity main effects for all four outcomes in Tables 3 and 4. Additional support comes from the result that when the variance explained by ethnicity was allowed to remain in the error term in the evaluations of 3-way interactions in ANOVAs using sex instead of ethnicity, the 3-way interaction became non-significant. Space constraints do not allow for more extensive evaluation of which ethnic groups contributed most to the results and the mechanisms associated with those effects, but we will return to those questions in future reports.
Two ancillary findings are worthy of comment. First, it's interesting to note the decreased drinking for Controls at four weeks. This may relate to a “placebo” and/or a “herd” effect. In the former, filling out a drinking questionnaire might call attention to dangers associated with alcohol, with subsequent temporary decreases in alcohol intake (Litten et al., 2013). Regarding a “herd” effect, Controls living in close proximity to LRB or SOTA participants may have been indirectly affected by modeling changes in drinking behaviors of the video participants (Conrod et al., 2013). Second, the finding that participants with low LR in the LRB Group showed greater increases in their self-recognition of their low sensitivity to alcohol than low LRs in SOTA might indicate that the change in self-evaluation partially mediated the greater change in maximum drinks for LRB participants with low LR. This, too, will require further analyses.
The present data have several levels of potential importance. The central message is that prevention protocols for many behaviors may be optimized by organizing the message around a preexisting phenotype with which subjects can identify. A second lesson is that such approaches may be beneficial even when delivered on the Internet in a relatively inexpensive protocol that incorporates, as best as possible, key elements of MI and BI approaches.
The results presented here set the stage for several future steps. First, having established that interventions were associated with short term improvements in drinking quantities, it is important to continue to follow these subjects to determine how long the effect lasts. This will be addressed through additional follow ups over the next nine months. Second, immediately following the 12-week assessments, LRB and SOTA subjects will view a 60-minute video that summarizes major points from their original videos, with similar distinctions between how messages are framed for the LRB and SOTA Groups. This “booster” session will be followed with assessments that evaluate the impact of the booster and, if present, determine how long that effect lasts. Third, there is a need to see if spacing the original videos over a longer period (e.g., over two rather than one month) might produce greater or longer lasting effects, and it will be interesting to evaluate the protocol's effects on alcohol problems as well as on drinking patterns. Finally, we plan to evaluate if the same type of Internet-based approach is useful for mitigating future heavy drinking associated with externalizing and internalizing characteristics (Crum et al., 2013; Sher et al., 1991), and whether the approach works in high school or military settings or for students mandated to take alcohol education due to violations of campus policies.
Our results must be viewed in light of several caveats. The study was conducted at the same university as the pilot protocol, and evaluations of generalizability to other settings are needed. Second, UCSD students are primarily of EA, Asian, and Hispanic backgrounds, and, considering the importance of race/ethnicity in the analyses, the impact of the prevention protocol on AA and other ethnic groups will require additional study. Third, our focus was on students who were already drinkers (testing the prevention protocol in students at greater risk for heavy drinking) and our personal interest was to work with the broad scope of drinkers who are more representative of drinking students, rather than those with alcohol dependence. Thus, it will be important to test the intervention in students selected because of problematic drinking and on adolescents who have not yet begun to drink. Fourth, we also chose to evaluate how well the protocol works in entering freshmen who were willing to be part of the alcohol education videos, similar to what is likely to be the case if such Internet-based videos are implemented at any university. Thus, we didn't focus on results of students who refused participation or who never participated enough to gain likely benefits from the videos, choosing to not use an intention to treat design, a decision that might exaggerate intervention effects. Additionally, it is important to note that racial/ethnic backgrounds and alcohol histories were all self-reported. However, despite these issues, the current work supports the role of an Internet-based and relatively inexpensive prevention program tailored to address a relatively common predisposing phenotype that increases the risk of heavy drinking, the low LR to alcohol, in decreasing heavier drinking in college freshmen.
Acknowledgments
Sources of Support: NIH grants 1 R01 AA021162 and 5 T32 AA013525
Footnotes
Second revision submitted to Alcoholism: Clinical and Experimental Research 10/15/2014
References
- American Psychiatric Association. Fourth diagnostic and statistical manual. APA Press; Washington DC: 1994. [Google Scholar]
- Barnett NP, Clerkin EM, Wood M, Monti PM, Tevyaw TO, Corriveau D, Fingeret A, Kahler CW. Description and predictors of positive and negative alcohol-related consequences in the first year of college. J Stud Alcohol Drugs. 2014;75:103–114. doi: 10.15288/jsad.2014.75.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Descriptive and injunctive norms in college drinking: a meta-analytic integration. J Stud Alcohol. 2003;64:331–341. doi: 10.15288/jsa.2003.64.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bucholz KK, Cadoret R, Cloninger CR, Dinwiddie SH, Hesselbrock VM, Nurnberger JI, Jr, Reich T, Schmidt I, Schuckit MA. A new, semi-structured psychiatric interview for use in genetic linkage studies: a report on the reliability of the SSAGA. J Stud Alcohol. 1994;55:149–158. doi: 10.15288/jsa.1994.55.149. [DOI] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LA, Carey MP, DeMartini KS. Individual-level interventions to reduce college student drinking: a meta-analytic review. Addict Behav. 2007;32:2469–2494. doi: 10.1016/j.addbeh.2007.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Champion KE, Newton NC, Barrett EL, Teesson M. A systematic review of school-based alcohol and other drug prevention programs facilitated by computers or the Internet. Drug Alcohol Rev. 2013 Mar;32:115–123. doi: 10.1111/j.1465-3362.2012.00517.x. [DOI] [PubMed] [Google Scholar]
- Chinn CA, Brewer WF. The role of anomalous data in knowledge acquisition: a theoretical framework and implications for science instruction. Rev Educational Res. 1993;63:1–49. [Google Scholar]
- Chung T, Martin CS. Subjective stimulant and sedative effects of alcohol during early drinking experiences predict alcohol involvement in treated adolescents. J Stud Alcohol Drugs. 2009;70:660–667. doi: 10.15288/jsad.2009.70.660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos-Ryan N. Long-term effects of a personality-targeted intervention to reduce alcohol use in adolescents. J Consult Clin Psychol. 2011;79:296–306. doi: 10.1037/a0022997. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos-Ryan N, Strang J. Brief, personality-targeted coping skills interventions and survival as a non-drug user over a 2-year period during adolescence. Arch Gen Psychiatry. 2010;67:85–93. doi: 10.1001/archgenpsychiatry.2009.173. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, O'Leary-Barrett M, Newton N, Topper L, Catellanos-Ryan N, Mackie C, Girard A. Effectiveness of a selective, personality-targeted prevention program for adolescent alcohol use and misuse. JAMA Psychiatry. 2013;70:334–342. doi: 10.1001/jamapsychiatry.2013.651. [DOI] [PubMed] [Google Scholar]
- Crum RM, Mojtabai R, Lazareck S, Bolton JM, Robinson J, Sareen Jitender, Green KM, Stuart EA, La Flair L, Alvanzo AAH, Storr CL. A prospective assessment of reports of drinking to self-medicate mood symptoms with the incidence and persistence of alcohol dependence. JAMA Psychiatry. 2013;70:718–726. doi: 10.1001/jamapsychiatry.2013.1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehlers CL, Phillips E, Schuckit MA. EEG alpha variants and alpha power in Hispanic American and white non-Hispanic American young adults with a family history of alcohol dependence. Alcohol. 2004;33:99–106. doi: 10.1016/j.alcohol.2004.05.003. [DOI] [PubMed] [Google Scholar]
- Eng MY, Luczak SE, Wall TL. ALDH2, ADH1B, and ADH1C genotypes in Asians: a literature review. Alcohol Res Health. 2007;30:22–27. [PMC free article] [PubMed] [Google Scholar]
- Fromme K, Corbin WR, Kruse MI. Behavioral risks during the transition from high school to college. Dev Psychol. 2008;44:1497–1504. doi: 10.1037/a0012614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hesselbrock M, Easton C, Bucholz KK, Schuckit MA, Hesselbrock V. A validity study of the SSAGA - a comparison with the SCAN. Addiction. 1999;94:1361–1370. doi: 10.1046/j.1360-0443.1999.94913618.x. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Overview of key findings 2012, in Monitoring the Future national results on adolescent drug use. Institute for Social Research; The University of Michigan, Ann Arbor: 2013. [Google Scholar]
- King AC, McNamara PJ, Hasin DS, Cao D. Alcohol challenge responses predict future alcohol use disorder symptoms: a 6-year prospective study. Biol Psychiatry. 2014;75:798–806. doi: 10.1016/j.biopsych.2013.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King KM, Chassin L. Adolescent stressors, psychopathology, and young adult substance dependence: a prospective study. J Stud Alcohol Drugs. 2008;69:629–638. doi: 10.15288/jsad.2008.69.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kypri K, McCambridge J, Vater T, Bowe SJ, Saunders JB, Cunningham JA, Horton NJ. Web-based alcohol intervention for Māori university students: double-blind, multi-site randomized controlled trial. Addiction. 2012;108:331–338. doi: 10.1111/j.1360-0443.2012.04067.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Indentification, prevention, and treatment revisited: individual-focused college drinking prevention strategies 1999-2006. Addict Behav. 2007;32:2439–2468. doi: 10.1016/j.addbeh.2007.05.006. [DOI] [PubMed] [Google Scholar]
- Li D, Zhao H, Gelernter J. Strong association of the alcohol dehydrogenase 1B gene (ADH1B) with alcohol dependence and alcohol-induced medical diseases. Biol Psychiatry. 2011;70:504–512. doi: 10.1016/j.biopsych.2011.02.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litten RZ, Castle IJP, Falk D, Ryan M, Fertig J, Chen CM, Yi Hy. The placebo effect in clinical trials for alcohol dependence: an exploratory analysis of 51 naltrexone and acamprosate studies. Alcohol Clin Exp Res. 2013;37:2128–2137. doi: 10.1111/acer.12197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallett KA, Varvil-Weld L, Borsari B, Read JP, Neighbors C, White HR. An update of research examining college student alcohol-related consequences: new perspectives and implications for interventions. Alcohol Clin Exp Res. 2013;37:709–716. doi: 10.1111/acer.12031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neighbors C, Lee CM, Lewis MA, Fossos N, Larimer ME. Are social norms the best predictor of outcomes among heavy-drinking college students? J Stud Alcohol Drugs. 2007;68:556–565. doi: 10.15288/jsad.2007.68.556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newlin DB, Renton RM. High risk groups often have higher levels of alcohol response than low risk: the other side of the coin. Alcohol Clin Exp Res. 2010;34:199–202. doi: 10.1111/j.1530-0277.2009.01081.x. [DOI] [PubMed] [Google Scholar]
- Pedersen S, McCarthy D. Differences in acute response to alcohol between African Americans and European Americans. Alcohol Clin Exp Res. 2013;37:1056–1063. doi: 10.1111/acer.12068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polak MA, Conner TS. Impairments in daily functioning after heavy and extreme episodic drinking in university students. Drug Alcohol Rev. 2012;31:763–769. doi: 10.1111/j.1465-3362.2012.00429.x. [DOI] [PubMed] [Google Scholar]
- Quinn PD, Fromme K. Subjective response to alcohol challenge: a quantitative review. Alcohol Clin Exp Res. 2011;35:1759–1770. doi: 10.1111/j.1530-0277.2011.01521.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray LA, Audette A, DiCristoforo S, Odell K, Kaiser A, Hutchison KE. Behavioral, laboratory, and genetic correlates of low level of response to alcohol. Alcohol Clin Exp Res. 2007;31:131A. [Google Scholar]
- Saltz RF, Welker LR, Paschall MJ, Feeney MA, Fabiano PM. Evaluating a comprehensive campus-community prevention intervention to reduce alcohol-related problems in a college population. J Stud Alcohol Drugs. 2009;Suppl 16:21–27. doi: 10.15288/jsads.2009.s16.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuckit MA. A brief history of research on the genetics of alcohol and other drug use disorders. J Stud Alcohol Drugs. 2014;Suppl 17:59–67. doi: 10.15288/jsads.2014.s17.59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuckit MA, Kalmijn JA, Smith TL, Saunders G, Fromme K. Structuring a college alcohol prevention program on the low level of response to alcohol model: a pilot study. Alcohol Clin Exp Res. 2012a;36:1244–1252. doi: 10.1111/j.1530-0277.2011.01723.x. [DOI] [PubMed] [Google Scholar]
- Schuckit MA, Smith TL, Danko GP, Bucholz KK, Agrawal A, Dick DM, Nurnberger JI, Jr, Kramer J, Hesselbrock M, Saunders G, Hesselbrock V. Predictors of subgroups based on maximum drinks per occasion over six years for 833 adolescents and young adults in COGA. J Stud Alcohol Drugs. 2014;75:24–34. doi: 10.15288/jsad.2014.75.24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuckit MA, Smith TL, Heron J, Hickman M, Macleod J, Lewis G, Davis JM, Hibbeln JR, Brown S, Zuccolo L, Miller LL, Davey-Smith G. Testing a level of response to alcohol-based model of heavy drinking and alcohol problems in 1,905 17-year-olds. Alcohol Clin Exp Res. 2011a;35:1897–1904. doi: 10.1111/j.1530-0277.2011.01536.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuckit MA, Smith TL, Trim RS, Allen RC, Fukukura T, Knight EE, Cesario EM, Kreikbaum SA. A prospective evaluation of how a low level of response to alcohol predicts later heavy drinking and alcohol problems. Am J Drug Alcohol Abuse. 2011b;37:479–486. doi: 10.3109/00952990.2011.598590. [DOI] [PubMed] [Google Scholar]
- Schuckit MA, Smith TL, Trim RS, Kuperman S, Kramer J, Hesselbrock V, Bucholz KK, Nurnberger JI, Jr, Hesselbrock M, Saunders G. Sex differences in how a low sensitivity to alcohol relates to later heavy drinking. Drug Alcohol Rev. 2012b;31:871–880. doi: 10.1111/j.1465-3362.2012.00469.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott DM. Magnitude of the problem of drinking alcohol on college campuses, commentary on “Structuring a college alcohol prevention program on the low level of response to alcohol model: a pilot model ”. Alcohol Clin Exp Res. 2012;36:1126–1130. doi: 10.1111/j.1530-0277.2012.01828.x. [DOI] [PubMed] [Google Scholar]
- Sher KJ, Walkitzer KS, Wood PK, Brent EE. Characteristics of children of alcoholics: putative risk factors, substance use and abuse, and psychopathology. J Abnorm Psychol. 1991;100:427–448. doi: 10.1037//0021-843x.100.4.427. [DOI] [PubMed] [Google Scholar]
- Wu LTZ, Woody GE, Yang C, Pan JJ, Blazer DG. Racial/ethnic variations in substance-related disorders among adolescents in the United States. Archives Gen Psychiatry. 2011;68:1176–1185. doi: 10.1001/archgenpsychiatry.2011.120. [DOI] [PMC free article] [PubMed] [Google Scholar]