

Sir,
Musculoskeletal complaints have an immense potential to have a huge impact on the society through direct and indirect effects on health. These disorders have largely been neglected until recent times because of their “non-fatal outcomes.” Their importance was recognized by the United Nations and World Health Organization (WHO) through the endorsement of the decade 2000-2010 as a bone and joint decade.[1] In India, rheumatic musculoskeletal symptoms were found to be the commonest morbidities in the community.[2] Yet, there is a lack of studies reporting prevalence of musculoskeletal complaints and associated risk factors from Tamil Nadu and Puducherry.
In October 2013, we conducted a community-based cross-sectional study to estimate the prevalence of musculoskeletal pain and joint complaints, and to find out the predictors of musculoskeletal pain, particularly with respect to socio-demographic factors, personal and medical history, and work related risk factors. It was carried out in one of the four villages under the field practice area of Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry. This village having a population of around 3,500 was selected purposively for the study. Individuals ≥20 years of age and residing in Thondamanatham village for at least one year were included. Individuals who were bed ridden or were too sick to participate were excluded. Using prevalence of the musculoskeletal complaints as 26.08%,[3] and an absolute precision of 5%, the required sample size was 296. One person was randomly chosen from one household by lottery method out of those eligible and available at the time of visit. Systematic random sampling was used to select the households.
A pre-tested semi-structured interview schedule was used for data collection. A pain diagram having a sketch of the human body in a standing posture (rear view) along with body locations marked with arrows was shown to the participants. Participants were asked to pinpoint the body location (s) where pain/joint-related complaints were felt in the preceding seven days (current pain) and one year. Joint-related complaints were complaints other than pain (i.e., stiffness, tenderness, loss of flexibility, or feeling a grating sensation while using a joint). Informed written consent was taken from all the study participants. Those having musculoskeletal complaints were referred to the nearest Primary Health Centre for necessary management and follow up. Data were entered in Epidata software (version 3.1) and analyzed using Statistical Package for Social Sciences (SPSS) version 17.0. Chi-square test was used to compare proportions among groups. Variables significantly associated (P < 0.25) with musculoskeletal pain (dependent variable) in bivariate analysis were included in multivariate analysis using logistic regression.
A total of 304 participants were recruited, of which 223 (73.4%) were females. Mean age was 42.2 (SD 14.1) years. Majority (47.4% participants) belonged to the age group 20-39 years, were currently married (83.9%), and 59.5% belonged to lower socio-economic classes (modified Prasad's classification). Around 32% of the study participants were illiterate or did not complete primary school education. About 39.8% participants went out of their homes for work or study purpose.
One year prevalence of musculoskeletal pain was 33.9% (103/304). Prevalence of joint related complaints (other than pain) was 29.7% (90/303). When current pain and one year prevalence of pain was considered, lower back was most commonly involved (10.2% and 14.5% of participants respectively), followed by hips/thighs and knees. When joint complaints were asked, knees were most commonly involved (current joint complaint in 18.1% and one year pain in 23.4% participants), followed by hips/thighs and ankles. Results of multivariate analysis are shown in Table 1.
Table 1.
Predictors of musculoskeletal pain identified by regression analysis (n=304)
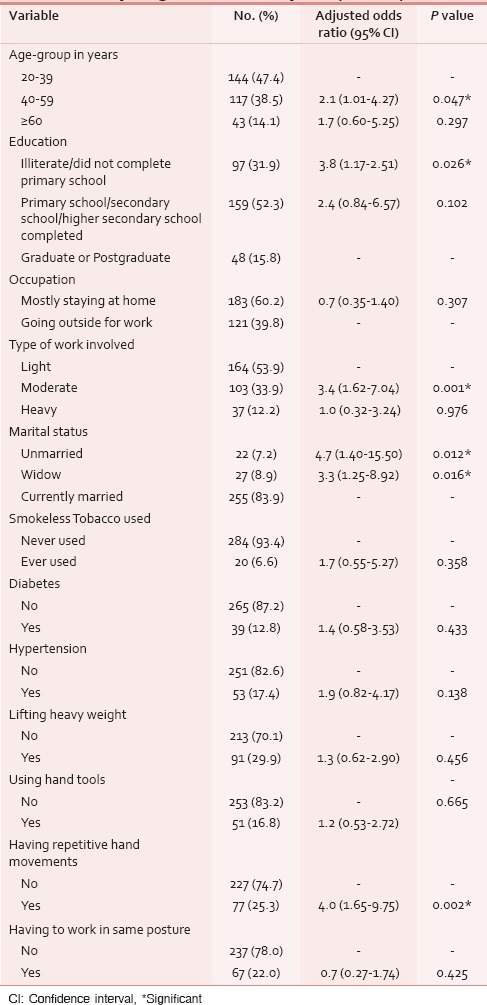
Earlier studies from India reported prevalence of rheumatic-musculoskeletal symptoms (RMS)/disorders ranging from 7.08-26.08%.[3,4,5,6,7] Our finding that being unmarried or widow was associated with musculoskeletal pain was in contrast to a previous study reporting married status as a predictor for RMSD.[8] In previous studies, lower education status has been found to be significantly associated with a higher prevalence of RMSD, as in our study.[7,8] In the present study, 12.2% subjects perceived their work as heavy. This was similar to a previous study in which 19% men and 6% women belonging to 25-54 years age-group had perceived their work as heavy.[6]
One limitation of our study was that other factors which might influence the presence/absence of musculoskeletal pain, for example, nutritional status, amount of physical activity, and anthropometric parameters alike Body Mass Index (BMI) and body fat composition were not studied. Also there is a predominance of female participants, though gender was not found to be significantly associated with musculoskeletal pain during analysis.
In the present study, one year prevalence of musculoskeletal pain and joint related complaints was found to be 33.9% and 29.7%, respectively. Middle age, lower education status, not being currently married, performing moderate work, and having repetitive hand movements at work acted as predictors of musculoskeletal pain. These factors should be kept in mind while making ergonomic modifications at the workplace, while devising physiotherapy regimens, and during Information, education and communication activities.
REFERENCES
- 1.WHO Scientific Group on the Burden of Musculoskeletal Conditions at the Start of the New Millennium. The burden of musculoskeletal conditions at the start of the new millennium. World Health Organ Tech Rep Ser. 2003:919. [PubMed] [Google Scholar]
- 2.Chopra A, Patil J, Billempelly V, Relwani J, Tandle HS. WHO-ILAR COPCORD Study. WHO International League of Associations from Rheumatology Community Oriented Program from Control of Rheumatic Diseases. Prevalence of rheumatic diseases in a rural population in western India: A WHO-ILAR COPCORD Study. J Assoc Physicians India. 2001;49:240–6. [PubMed] [Google Scholar]
- 3.Mathew AJ, Chopra A, Thekkemuriyil DV, George E, Goyal V, Nair JB, et al. Trivandrum COPCORD Study Group. Impact of musculoskeletal pain on physical function and health-related quality of life in a rural community in south India: A WHO-ILAR-COPCORD-BJD India study. Clin Rheumatol. 2011;30:1491–7. doi: 10.1007/s10067-011-1824-0. [DOI] [PubMed] [Google Scholar]
- 4.Sharma R. Epidemiology of Musculoskeletal Conditions in India. New Delhi, India: Indian Council of Medical Research (ICMR); 2012. [Google Scholar]
- 5.Bihari V, Kesavachandran C, Pangtey BS, Srivastava AK, Mathur N. Musculoskeletal pain and its associated risk factors in residents of National Capital Region. Indian J Occup Environ Med. 2011;15:59–63. doi: 10.4103/0019-5278.90375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chopra A, Saluja M, Patil J, Tandale HS. Pain and disability, perceptions and beliefs of a rural Indian population: A WHO. ILAR COPCORD study. WHO-International League of Associations for Rheumatology. Community Oriented Program for Control of Rheumatic Diseases. J Rheumatol. 2002;29:614–21. [PubMed] [Google Scholar]
- 7.Pingle AS, Pandit DD. A cross sectional study of rheumatic muskuloskeletal disorders in an urban slum population. Indian J Community Med. 2006;31:244–7. [Google Scholar]
- 8.Paul BJ, Rahim AA, Bina T, Thekkekara RJ. Prevalence and factors related to rheumatic musculoskeletal disorders in rural south India: WHO-ILAR-COPCORD-BJD India Calicut study. Int J Rheum Dis. 2013;16:392–7. doi: 10.1111/1756-185X.12105. [DOI] [PubMed] [Google Scholar]