

Abstract
Background:
Pediatric subscapularis tears are known to be rare injuries. They are often associated with an avulsion fragment of the lesser tuberosity leading to dual description in the literature of either subscapularis tear or lesser tuberosity avulsion. Historically, they were managed nonoperatively; however, outcomes have improved with operative management. Nonoperative management often led to bony overgrowth at the lesser tuberosity that limited motion. The literature is limited to case reports and a few small case series, often not restricted to pediatric patients.
Study Design:
Case series.
Level of Evidence:
Level 5.
Methods:
Radiographic and operative databases were retrospectively reviewed to identify pediatric patients with subscapularis tears or lesser tuberosity avulsions in the past 10 years.
Results:
Five cases of pediatric subscapularis tears were identified that underwent operative management. Of the 5 cases, 4 had delayed presentation. In 1 case, the lesser tuberosity fragment was initially missed on radiographic imaging. All patients underwent operative management.
Conclusion:
These cases add to the body of knowledge of a rare pediatric injury that is commonly missed or diagnosis delayed. The importance of suspicion in the adolescent male patient without instability and unrelenting shoulder pain is stressed. Additionally, the importance of early magnetic resonance imaging with suspicion as well as an axillary view of the shoulder is demonstrated. As with all rare entities, it is important to disseminate information on natural history and interventions for this injury.
Keywords: shoulder, rotator cuff, pediatric sports medicine, imaging, radiology, sports trauma
Rotator cuff tears are an uncommon injury in the pediatric population, and isolated injury to the subscapularis tendon is even rarer. Trauma to the shoulder more commonly results in injuries to the weaker developing bone and physis than the stronger musculotendinous unit.16 Subscapularis injuries, when seen in skeletally immature patients, are usually associated with a fragment of the lesser tuberosity of varying size because of failure at the developing bony interface.22 There have been several case reports to date of pediatric subscapularis tears, the majority of which are associated with some avulsion of the lesser tuberosity.1,5,12-15,17-19,21,23 Isolated subscapularis injuries have been reported in skeletally immature patients, however, and are thought to be due to chronic overuse.22
These injuries are difficult to diagnose on the acute examination and may demonstrate overlap with an instability injury, a physeal injury, or may even be misdiagnosed as a strain.21 As a result, diagnosis is often delayed until patients present with persistent pain and weakness. The mechanism of injury to the subscapularis is an extremity forced into external rotation and abduction. Injuries and dislocations occur from direct trauma, including football, wrestling, hockey, motor cycle accident, assault, and volleyball, as well as repetitive noncontact activities, including fly fishing, falls while skateboarding, and baseball.14,23
While descriptive terms of these injuries vary between subscapularis tear and lesser tuberosity avulsion fracture, the majority of reports to date describe some bony component diagnosed by radiographs, magnetic resonance imaging (MRI), or at the time of surgery.2,3,9,11-15,17-19,21 Because the bony fragment may vary in size from a complete avulsion to a thin sleeve, they may not always be evident on plain radiographs. Complete avulsion of the subscapularis tendon off of the humerus with a thin bony fragment has been treated with direct repair.26 In some cases, imaging cannot identify the bony fragment, which is not appreciated until operative intervention and incorporated into the repair.15
This injury is best managed with surgical repair.18 When the lesser tuberosity fragment is large enough, fixation with screws has been described up to 1 year after injury.10,13,24 When residual tendon is attached to a footprint, direct repair is possible.1,22 In many reports, the subscapularis is repaired with sutures and anchors or drill holes through the lesser tuberosity footprint.6,7,12,14,15,19
Case Series
Case 1
A 12-year-old male presented with 3 days of right shoulder pain after colliding forcefully with another player in a soccer game. On initial physical examination, the patient localized pain to the proximal humeral physis. While he had active motion, his motor examination was significantly limited. Radiographs were interpreted as a Salter Harris I fracture of the proximal humerus, and widening at the lateral aspect of the physis was noted. There was no displacement or epiphyseal fracture line, so the plan was to re-examine the patient in several weeks because of pain. Additional radiographic imaging was also planned to look for periosteal reaction.
Two weeks later, the patient denied pain but demonstrated a noticeable shrug on elevation and abduction of the shoulder. He guarded on all instability tests. Radiographs at that time were normal, and he was advanced to a stretching regimen with gradual return to noncontact activities.
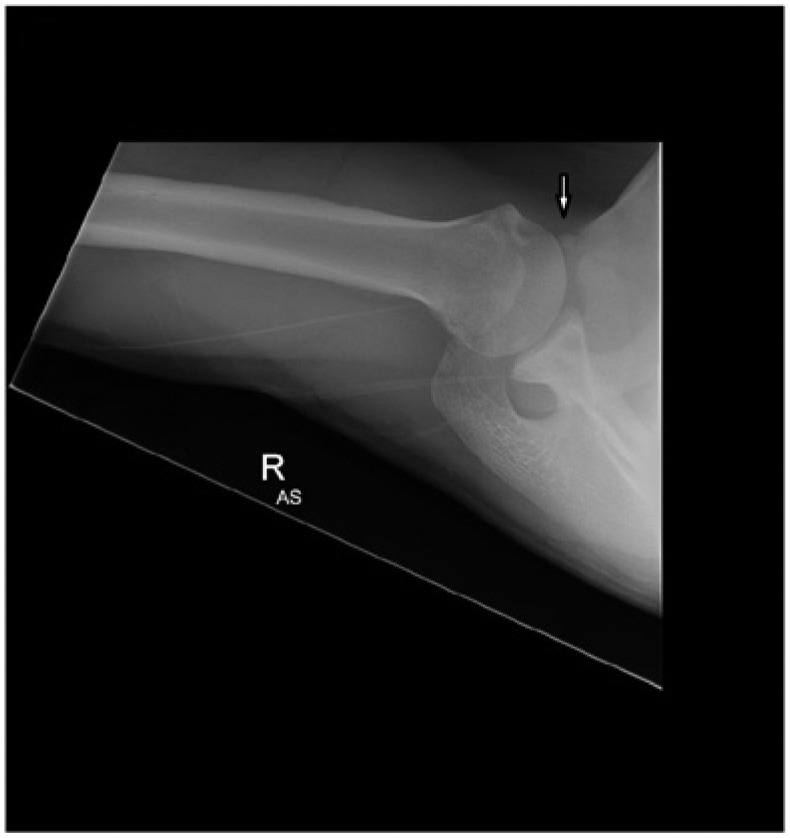
The next follow-up was delayed by the patient to 2 months after injury when he complained of anterior shoulder pain with overhead throwing activities. MRI demonstrated a small bony avulsion of the lesser tuberosity, and a retrospective review of the axillary view on presentation revealed a thin bony fragment on radiographs (Figures 1 and 2). He underwent open subscapularis repair with Mitek suture anchors (DePuy Mitek, Warsaw, Indiana) and had an uneventful postoperative course.
Figure 1.

(a,b) External/internal and (c) axillary views of case 1 on presentation. The periosteal sleeve avulsion is visible on the axial view.
Figure 2.
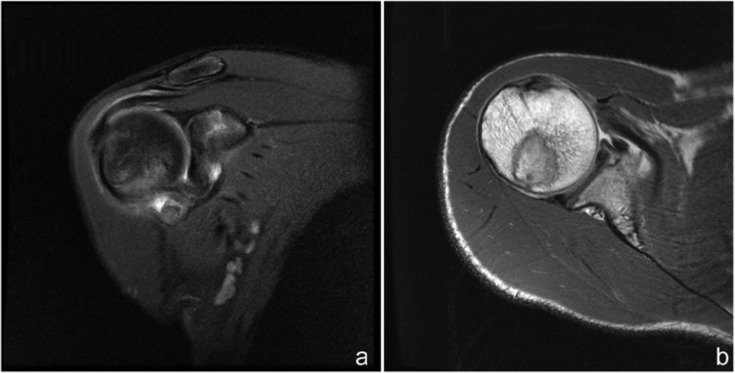
Magnetic resonance image (MRI) of case 1 subscapularis tear. MRI was performed 9 weeks after injury. (a) The coronal image demonstrates edema. (b) The axial image demonstrates subscapularis tendon retraction.
Case 2
A right hand–dominant 18-year-old male presented 5 weeks after a football injury to his right shoulder complaining of pain and paresthesia localized to his triceps region and generalized weakness of the shoulder. Physical examination revealed no atrophy of the shoulder girdle. He had difficulty lifting the right arm, and the lift-off test4 was positive with a positive O’Brien sign.20 Eccentric loading of the rotator cuff demonstrated weakness.
Shoulder radiographs revealed an avulsion fracture of the lesser tuberosity (Figure 3). A shoulder MRI performed on the same day demonstrated the avulsion fracture with retraction of the subscapularis and a small area of degeneration in the superior labrum (Figure 4).
Figure 3.
Axillary view of case 2 demonstrating avulsion fracture of the lesser tuberosity.
Figure 4.

Case 2. Axial magnetic resonance images demonstrate avulsion fracture with retraction of the subscapularis.
Arthroscopic repair was performed. Although the fragment was clearly visible on MRI, it had retracted and was only visualized arthroscopically after intracapsular dissection. A direct repair using 2 sutures through the retracted tendon was performed. Postoperatively, the patient had an uneventful course and was cleared for return to play at 4 months postoperative.
Case 3
A 12-year-old male presented 6 days after a wrestling injury to the shoulder that occurred while the arm was in an abduction external rotation. Physical examination demonstrated weakness with belly press and limited external rotation, abduction, and forward flexion. MRI showed complete avulsion of the subscapularis with a periosteal sleeve of the lesser tuberosity.
The patient underwent an open repair (Figure 5). At 3-month follow-up, the patient had full strength and range of motion.
Figure 5.
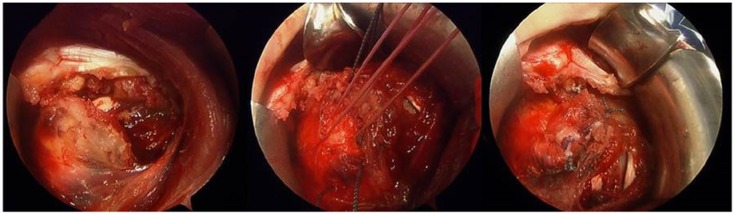
Case 3. Open view of subscapularis tear after repair with repair sutures in place.
Case 4
A 12-year-old male was injured while playing lacrosse as his shoulder was abducted and externally rotated when several players fell on top of him. He was initially managed by an emergency department, placed in a sling, and referred to physical therapy. Persistent pain and weakness complaints in the shoulder led him to seek further care after 1 month. His MRI revealed an avulsed subscapularis tendon with medial and inferior displacement of the associated lesser tuberosity fragment.
The patient had an arthroscopic repair. The postoperative course was uneventful, and he returned to sports at 5 months.
Case 5
A 13-year-old male injured in hockey presented for persistent pain after conservative measures failed at 3 months. An MRI demonstrated a subscapularis tear with an avulsed lesser tuberosity. He had a markedly positive lift-off test and pain in the abducted and externally rotated position.
After arthroscopic repair with fiber wire and 2 suture anchors, he returned to sport and at 6-month follow-up, had made the US National Hockey team.
Discussion
Injuries to the subscapularis tendon in the skeletally immature population are associated with an avulsion fracture of the lesser tuberosity of varying size.14,25,26 These injuries should be managed operatively, as a missed diagnosis can lead to persistent pain and weakness.8,9,11 In our series, time to diagnosis from injury ranged from 6 days to 3 months, emphasizing the difficulty in recognizing these injuries.
Suspicion should be raised in the adolescent patient with forced external rotation with an abducted shoulder or forced forward flexion of the arm.18 These injuries have occurred in patients as young as 8 years old, but tend to cluster in 12- to 14-year-olds.1,12-15,17 Isolated deficits in the subscapularis may not be appreciated because of global weakness and pain.
Early imaging is critical: The smaller fragments seen in children are often missed on anteroposterior, internal, and external rotation views of the humerus. An axillary view is often necessary to visualize the fragment, and even so, may be missed initially.17
Patients with nonoperatively managed subscapularis avulsion fractures can go on to develop chronic shoulder pain.5 These patients developed exostoses at the site of the avulsed tuberosity as well as degeneration within the subscapularis muscle. These can become large enough to inhibit internal rotation. Patients with surgical intervention delayed up to 20 weeks can still do well after repair.24 The results for nonoperative management have not been as successful and would recommend surgical intervention for these rare injuries.17
Footnotes
The following authors declared potential conflicts of interest: Daniel W. Green, MD, MS, FAAP, FACS, is a paid consultant for Arthrex and Pega Medical; Russell F. Warren, MD, is a board member of Orthonet and Ivy Healthcare Capital Partners, receives royalties from Biomet, and holds stock/stock options in Orthobond; Thomas L. Wickiewicz, MD, receives royalties from Mako.
References
- 1. Bhalla A, Higashigawa K, McAllister D. Subscapularis tendon rupture in an 8-year-old boy: a case report. Am J Orthop (Belle Mead NJ). 2011;40:471-474. [PubMed] [Google Scholar]
- 2. Echlin PS, Plomaritis ST, Peck DM, Skopelja EN. Subscapularis avulsion fractures in 2 pediatric ice hockey players. Am J Orthop (Belle Mead NJ). 2006;35:281-284. [PubMed] [Google Scholar]
- 3. Garrigues GE, Warnick DE, Busch MT. Subscapularis avulsion of the lesser tuberosity in adolescents. J Pediatr Orthop. 2013;33:8-13. [DOI] [PubMed] [Google Scholar]
- 4. Gerber C, Krushell RJ. Isolated rupture of the tendon of the subscapularis muscle. Clinical features in 16 cases. J Bone Joint Surg Br. 1991;73:389-394. [DOI] [PubMed] [Google Scholar]
- 5. Goeminne S, Debeer P. The natural evolution of neglected lesser tuberosity fractures in skeletally immature patients. J Shoulder Elbow Surg. 2012;21:E6-E11. [DOI] [PubMed] [Google Scholar]
- 6. Gouron R, Deroussen F, Juvet-Segarra M, Mancheron C, Bonnaire B, Collet LM. Isolated rupture of the subscapularis tendon in children: a case report and literature review. J Pediatr Orthop B. 2013;22:138-140. [DOI] [PubMed] [Google Scholar]
- 7. Heyworth BE, Dodson CC, Altchek DW. Arthroscopic repair of isolated subscapularis avulsion injuries in adolescent athletes. Clin J Sport Med. 2008;18:461-463. [DOI] [PubMed] [Google Scholar]
- 8. Klasson SC, Vander Schilden JL, Park JP. Late effect of isolated avulsion fractures of the lesser tubercle of the humerus in children. Report of two cases. J Bone Joint Surg Am. 1993;75:1691-1694. [DOI] [PubMed] [Google Scholar]
- 9. Kunkel SS, Monesmith EA. Isolated avulsion fracture of the lesser tuberosity of the humerus: a case report. J Shoulder Elbow Surg. 1993;2:43-46. [DOI] [PubMed] [Google Scholar]
- 10. Kuroda T, Go G, Ojima S, Nishi S, Mizuno K. Isolated avulsion fracture of the lesser tuberosity of the humerus: a case report. J Shoulder Elbow Surg. 1993;2:221-224. [DOI] [PubMed] [Google Scholar]
- 11. Le Huec JC, Schaeverbeke T, Moinard M, Kind M, Chauveaux D, Le Rebeller A. Isolated avulsion fracture of the lesser tubercle of the humerus in children. Acta Orthop Belg. 1994;60:427-429. [PubMed] [Google Scholar]
- 12. Levine B, Pereira D, Rosen J. Avulsion fractures of the lesser tuberosity of the humerus in adolescents: review of the literature and case report. J Orthop Trauma. 2005;19:349-352. [PubMed] [Google Scholar]
- 13. Paschal SO, Hutton KS, Weatherall PT. Isolated avulsion fracture of the lesser tuberosity of the humerus in adolescents. A report of two cases. J Bone Joint Surg Am. 1995;77:1427-1430. [DOI] [PubMed] [Google Scholar]
- 14. Polousky JD, Harms S. Subscapularis tendon injuries in adolescents: a report of 2 cases. J Pediatr Orthop. 2011;31:E57-E59. [DOI] [PubMed] [Google Scholar]
- 15. Provance AJ, Polousky JD. Isolated avulsion fracture of the subscapularis tendon with medial dislocation and tear of biceps tendon in a skeletally immature athlete: a case report. Curr Opin Pediatr. 2010;22:366-368. [DOI] [PubMed] [Google Scholar]
- 16. Ramachandran M, Skaggs D. Physeal injury. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. 4th ed. Philadelphia, PA: Saunders; 2009:19-40. [Google Scholar]
- 17. Ross GJ, Love MB. Isolated avulsion fracture of the lesser tuberosity of the humerus: report of two cases. Radiology. 1989;172:833-834. [DOI] [PubMed] [Google Scholar]
- 18. Shibuya S, Ogawa K. Isolated avulsion fracture of the lesser tuberosity of the humerus. A case report. Clin Orthop Relat Res. 1986;(211):215-218. [PubMed] [Google Scholar]
- 19. Sikka RS, Neault M, Guanche CA. An avulsion of the subscapularis in a skeletally immature patient. Am J Sports Med. 2004;32:246-249. [DOI] [PubMed] [Google Scholar]
- 20. Stetson WB, Templin K. The Crank test, the O’Brien test, and routine magnetic resonance imaging scans in the diagnosis of labral tears. Am J Sports Med. 2002;30:806-809. [DOI] [PubMed] [Google Scholar]
- 21. Sugalski MT, Hyman JE, Ahmad CS. Avulsion fracture of the lesser tuberosity in an adolescent baseball pitcher: a case report. Am J Sports Med. 2004;32:793-796. [DOI] [PubMed] [Google Scholar]
- 22. Tarkin IS, Morganti CM, Zillmer DA, McFarland EG, Giangarra CE. Rotator cuff tears in adolescent athletes. Am J Sports Med. 2005;33:596-601. [DOI] [PubMed] [Google Scholar]
- 23. Teixeira RP, Johnson AR, Higgins BT, Carrino JA, McFarland EG. Fly fishing-related lesser tuberosity avulsion in an adolescent. Orthopedics. 2012;35:e748-e751. [DOI] [PubMed] [Google Scholar]
- 24. Vezeridis PS, Bae DS, Kocher MS, Kramer DE, Yen YM, Waters PM. Surgical treatment for avulsion injuries of the humeral lesser tuberosity apophysis in adolescents. J Bone Joint Surg Am. 2011;93:1882-1888. [DOI] [PubMed] [Google Scholar]
- 25. Weiss JM, Arkader A, Wells LM, Ganley TJ. Rotator cuff injuries in adolescent athletes. J Pediatr Orthop B. 2013;22:133-137. [DOI] [PubMed] [Google Scholar]
- 26. White GM, Riley LH., Jr. Isolated avulsion of the subscapularis insertion in a child. A case report. J Bone Joint Surg Am. 1985;67:635-636. [PubMed] [Google Scholar]