

Abstract
Background:
Understanding the learning styles of medical students can drive the institutions to adapt instructional materials to enhance students’ learning of knowledge and skills. This study explored the learning styles of undergraduate medical students, comparing gender variations in terms of their significant preferences.
Materials and Methods:
A cross-sectional observational study was performed in 2012-2013, incorporating 1st-5th year undergraduate medical students of Taibah University. The instrument used was a Learning Style Questionnaire, with four learning styles (activist, reflector, theorist and pragmatist) and 40 items.
Results:
Of 450 students, 384 responded (response rate; 85%). No single learning style predominated; 96 (25%) reflectors, 78 (20%) theorists, 68 (17%) pragmatists, and 37 (9%) activists. Combined reflector and theorist was the predominant dual learning style in 27 (7%) students. Among genders, theorist style had a significant result (P = 0.071) indicating that theorists varied among genders due to their different opinions. Learning style preferences of theorists and pragmatists also showed a significant result (P = 0.000 each), depicting that both genders had unique preferences. Males had fewer variations of preferences, when compared with females who showed a significant difference of opinions (P < 0.05).
Conclusion:
The students in the study preferred diverse learning styles, which were unevenly distributed, reflectors being the most common and activists as the least common. The results reflect the need to promote self-directed learning and modifications of instructional strategies, with expectant tilt in the students’ learning styles towards activists and pragmatists.
Keywords: Learning styles, learning preferences, learning styles questionnaire, medical students, undergraduate medical curriculum
INTRODUCTION
Learning is the most striking capability, as it is the gateway to any other capability an individual might wish to develop. The process of learning is active and passive, taught and self-managed, short and long-term, superficial and deep, voluntary and compulsory, planned and accidental, formal and informal, and the process and an outcome.[1] These diverse learning dimensions spring from the presence of a variety of learning styles, which need to be understood for appropriate learning. Evidence-based research convincingly suggests that learning is more effective if education is delivered and oriented in a way that matches individuals’ learning style.[2] The process includes a combination of cognitive, affective, and physical factors, which an individual employs to understand, interact, and relate to the learning environment. It has been suggested that by identifying the knowledge of students’ learning styles, academic institutions can develop the strategic framework for the delivery of educational programs and resources to motivate students’ integration and application of professional knowledge.[3] Understanding the students preferred modes can also help the teacher in delivering instructions tailored to the students’ preferences, underpinning the need to coach the students by using diverse teaching strategies. For all practical reasons, if the students know their learning styles, they could prepare suitable material for self-directed learning (SDL).
Historically, a wealth of learning styles has been described in the literature. Convergent thinkers follow an argument in a linear fashion leading to a single conclusion, whereas divergent group follows diverse directions producing multiple conclusions.[4] Pask in 1976 challenged the convergent-divergent duality and coined the holist-serialist approach.[5] Holists intuitively synthesize concepts through illustrations and analogies; hence art students commonly adopt this style. Serialists develop piecemeal ideas by applying a logical and structured approach; this style being more obvious in science students. Later, Kolb presented experiential learning cycle of concrete experience, reflective observation, abstract conceptualization, and active experimentation.[6] Honey and Mumford further refined Kolb's experiential learning model and generated a Learning Styles Questionnaire (LSQ), which is based on the premise that the best way to determine learning styles is to question students on how they learn.[7] It is not clear that the LSQ has greater validity than Kolb's inventory, but it is still considered to be a useful instrument to measure learning styles in higher education.[8]
This study looks into the learning styles of the 1st-5th year undergraduate medical students at the college of medicine, Taibah University, Almadinah Almunawwarah, Saudi Arabia, using LSQ. The resulting dominant single and multiple preferred learning styles are presented, and their implications are analyzed.
MATERIALS AND METHODS
A cross-sectional observational study was conducted at the end of the academic year 2012-2013, on all the enrolled 1st-5th year male and female medical undergraduate students of Taibah University, Almadinah Almunawwarah, Saudi Arabia. This institution has a teacher-oriented, discipline-based, and nonsystematic curriculum. For a 5-year MBBS course, first half is devoted to basic sciences and the other half to clinical sciences, with minimal integration. The instrument used was a self-completion LSQ, which was adopted from Honey and Mumford.[7] LSQ measures the individual's tendency towards particular learning styles. For better understanding and convenience of the students, a validated Arabic version of LSQ was administered. The instrument contains four learning styles (activist, reflector, theorist and pragmatist) and 40 items [Appendix 1]. Each learning style had 10 statements randomly distributed in the instrument [Appendix 2]. Learning style is a distinctive and habitual manner of acquiring knowledge, skills and attitude, whereas learning preference is favoring one particular mode of teaching over another.[9] The relevant Institutional Review Board approved the study.
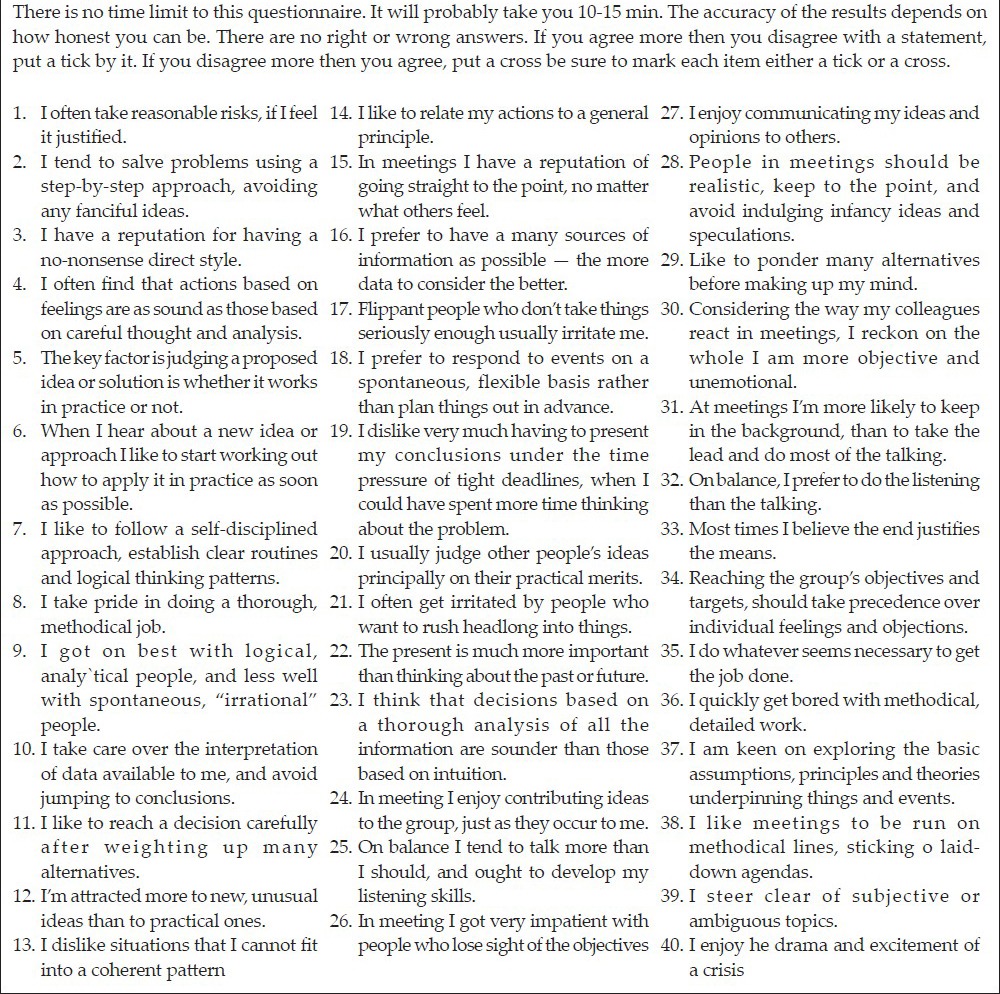
APPENDIX 1.
Learning styles questionnaire
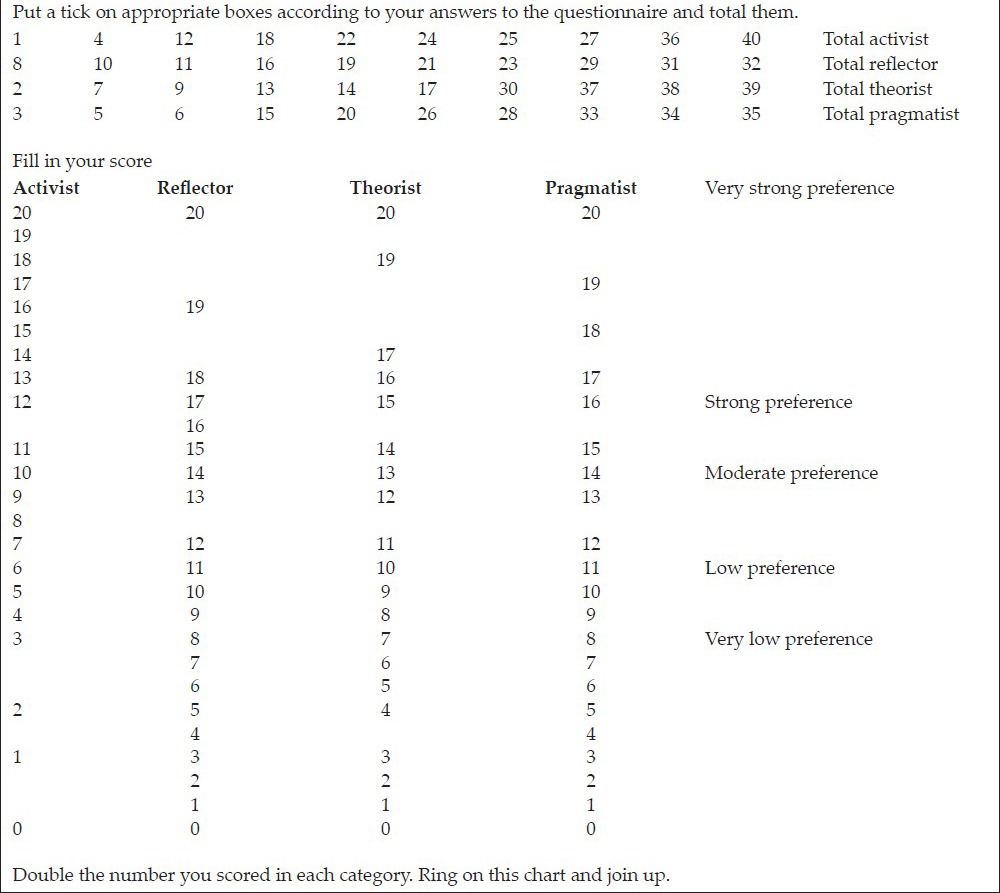
APPENDIX 2.
Scales of learning styles and preferences
Learning Styles Questionnaire does not contain direct questions about respondents’ learning; rather addresses general queries about an individual's beliefs and behaviors. The main purpose of the study was conveyed to the students in classrooms, and their verbal consent was obtained. The data were entered and analyzed through Statistical Package for Social Sciences 20 (SPSS). Frequency distribution and summary statistics were analyzed by descriptive analysis. For inferential analysis, Kolmogorov-Smirnov test was applied for confirming the normality of the data. Kruskal-Wallis test was used for comparing the learning styles of the entire cohort and Mann-Whitney U-test was used to compare learning styles and preferences of male and female students. Using 1%, 5% and 10% levels of significance, the hypotheses of Kruskal-Wallis and Mann-Whitney U-tests were assessed.
RESULTS
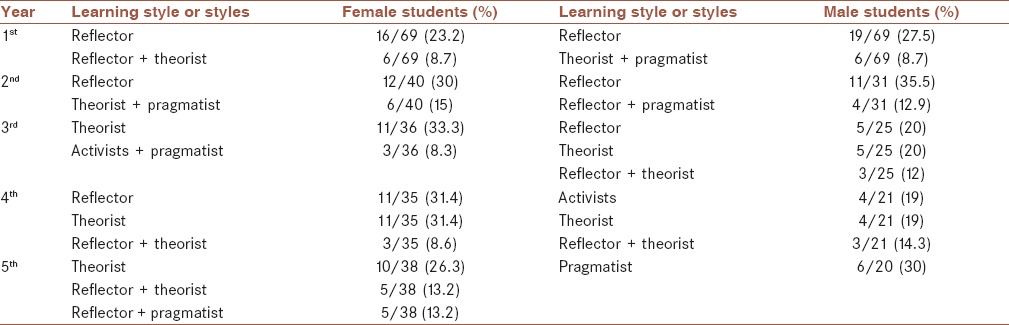
Of the 450 students, 384 responded (response rate of 85.3%). The cohort included 217 female and 167 male students with age range of 19-26 years. Reflector learning style was predominant in 96 (25%) students, followed by 78 (20%) theorists, 68 (17%) pragmatist, and 37 (9%) activists [Figure 1]. Combined reflector and theorist style was ranked the most frequent (27; 7%) dual learning style, whereas reflector, theorist, and pragmatist learning styles were the most common combination learning styles (7; 1.8%). Reflector style was the most common mode found in 1st year male (23.2%) and female students (27.5%) as shown in [Table 1]. The most common dual learning style of 1st year male students was reflector and theorist (8.7%), whereas first year female students preferred theorist and pragmatist styles (8.7%). Similarly, individual and dual learning styles of other years are appended in Table 1.
Figure 1.
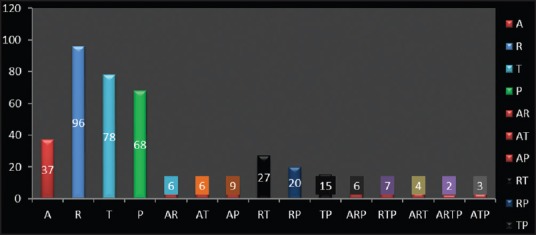
Trends of single and combined learning style(s) among the students (n = 384). A; Activists, R; Reflector, T; Theorist, P; Pragmatist, AR; Activist Reflector, AT; Activist Theorist, AP; Activist Pragmatist, RT; Reflector Theorist, RP; Reflector Pragmatist, TP Theorist Pragmatist, ARP; Activist Reflector Pragmatist, RTP; Reflector Theorist Pragmatist, ART; Activist Reflector Theorist, ATP; Activist Theorist Pragmatist
Table 1.
Frequency and percentage of learning styles
The different attributes of learning styles, as shown by descriptive statistics, are depicted in Table 2. Activists had median of 12 and standard deviation of 3.857, which shows dispersion of this style from 8.003 to 15.72 (12.00 + 3.857). The lowest value of this style was 0 and the highest was 20. Likewise, descriptive statistics of reflector, theorist and pragmatist learning styles are outlined in Table 2 with pictorial presentation in Figure 2.
Table 2.
Descriptive statistics of learning styles
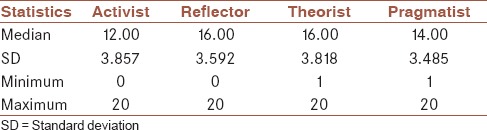
Figure 2.
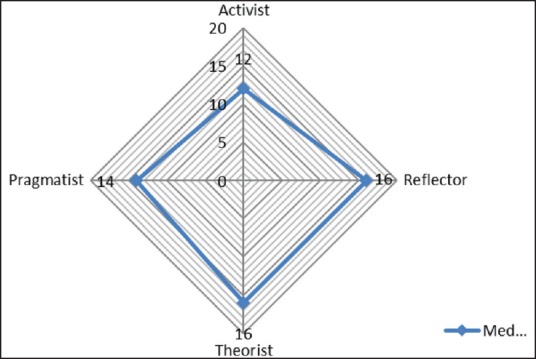
Learning styles profile in the study (384)
Before the application of inferential analysis, normality of the data was evaluated by one-sample Kolmogorov-Smirnov test. Results of this test showed that data of all learning styles was not normal [Table 3]. Each learning style has significant Z value, which is <0.05 and rejects the null hypothesis that “data is normally distributed”. Consequently, Kruskal-Wallis test was applied to compare learning styles and their preferences across 1st-5th year students which reported that theorist and pragmatist learning styles and preferences had statistically significant values [Table 4].
Table 3.
One sample Kolmogorov-Smirnov test

Table 4.
Description of student's learning styles and their preferences by Kruskal-Wallis test
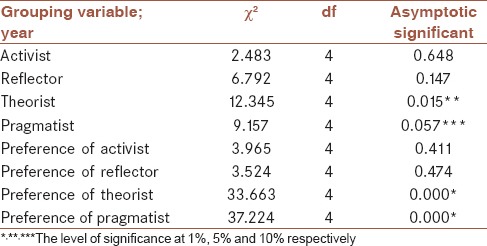
Figure 3 illustrates boxplots of significant learning styles and preferences by years. Dark lines in boxes indicate median of each year [Figure 3]. For the theorists boxplot, the dark lines show that theorists have median value of 14 in the 1st year, 16 in the 2nd year, remained unaffected in the 3rd and 4th year, and decreased to 14 in the 5th year. This shows that theorists had significantly different preference in 2nd year when compared to other years. The upper and lower whiskers, representing scores outside the middle 50%, also show yearly variations. The dots below the boxplots show the outliers or smallest values in the data. Significant differences in the learning styles and preferences were analyzed among male and female students as shown in Figure 4. The top left component is the boxplot of theorists, which shows that among female students, theorists had a median value of 16, compared with male students’ value of 14. This signifies that male students had less variant opinions when compared with female students. The dots below the boxplots indicate the outliers or smallest values in the data. Similarly, significant differences of preferences of other learning styles are portrayed in Figures 4.
Figure 3.
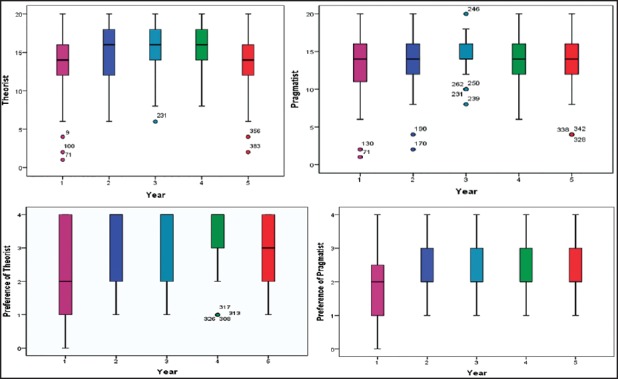
Boxplots of significant learning styles by years (n = 384)
Figure 4.
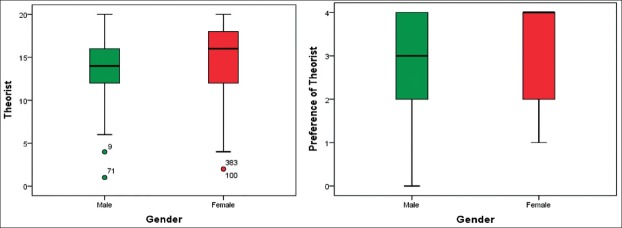
Boxplots of significant learning styles by gender (384)
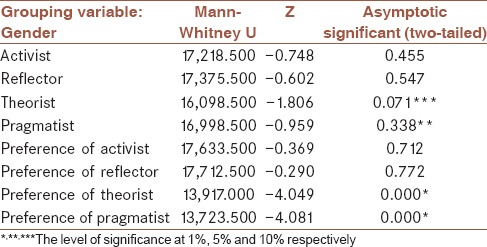
The results of Mann-Whitney U-test showed that only theorist learning style had significant variations of opinions (P = 0.071). On the other hand, preferences of theorists and pragmatists were significant and more preferred by male than female students [Table 5].
Table 5.
Analysis of student's learning styles and their preferences by Mann-Whitney U-test
DISCUSSION
The present study revealed reflector learning style to be the most common variant in 96 (25%) students. Reflectors are good observers, take time to assimilate evidence before commencing, and can reach a decision without pressure and influence.[10] On the other hand, reflectors are given insufficient data to clinch a conclusion, are pitched into doing something without notice, and they tend to postpone reaching a conclusion. Reflectors tend to be backseaters and passive participants in the meetings and discussions. In the present study by the 5th year, theorists dominated the learning styles in females (10/38; 26.3%), whereas pragmatists were dominant in male students (6/20; 30%). Overall, theorists (P < 0.015) and pragmatists (P < 0.057) had significant values. Theorists are traditionally rigid, don’t deviate from their typical mindset and avoid subjective judgments and anything flippant.[11] They involve analysis and synthesis of ideas with the help of basic assumptions, principles, and theories. Theorists and reflectors are inclined to abstract thinking and welcome text based materials.[12] This reflects the need to modify the instructional strategies for the undergraduate medical curriculum of Taibah University, which is seriously hampered by the absence of the university hospital. Clinical teaching is conducted at ministry of health hospitals with less desirable support and cooperation. This situation directs the faculty to tailor the course contents towards more theoretical and non-clinical side.
Our survey revealed 68 (17%) pragmatists in the cohort. Male students in 1st year were predominantly reflectors (27.5%), which shifted to pragmatist the style by the 5th year (30%). On the contrary, female students had persistently same learning styles of reflectors and theorists across the years. Pragmatists are keen practical learners and tend to conceptualize their ideas on concrete grounds.[13] They are essentially practical; ask open-ended questions in discussions and meetings, and always in the lookout for the best solution of the problems.
The study also illustrated that among genders, theorists had significant P = 0.071 indicating that this style varied among male and female students as they have different opinions. Learning style preferences of theorists and pragmatists also showed a significant result (P values of 0.000 each), which identifies that both genders had unique preferences. Across the years, learning styles of theorists and pragmatists showed significant P values of 0.015 and 0.057, respectively showing that all students differently perceived theorist and pragmatist learning styles. This trend indicates inconsistent learning styles of the students across the years and genders. One reason could be the nonintegrated curriculum of the medical school, which made the students switch to varying learning styles over the years. Slater et al. compared the learning preferences between 1st year male and female medical students, and found that female students tended to be more diverse than the male population, reporting a broader range of sensory modality combinations within their preference profiles.[14] Likewise, present research shows that male students had less variant opinions when compared to the female students.
In the present study, activists scored the lowest ranks across the groups (37; 9.6%). Activists are allowed to generate ideas and concepts without constraints of policy or feasibility, freely interact with people bouncing ideas and solving problems, and accept challenges with inadequate resources and adverse conditions. The desirable learning styles of medical students are pragmatist and activist, as they construct their knowledge framework on concrete issues and tend to manage their own learning process, leading to life-long and deep learning.[15] Such qualities of the learners glaringly lacked in the current situation, which is partly due to didactic lecture-based curriculum with little problem-solving exercises and the absence of the university hospital. The prerequisite for the delivery of an integrated spiral curriculum where basic and clinical disciplines are taught right from 1st year relies on a well-established university hospital. Currently, we are using ministry of health facilities for the clinical teaching and assessment venues in less desirable circumstances. Again, in this study, the most common dual learning style was reflector and theorist, reported in 27 (7%) students. Such findings necessitate an objective review of the curriculum and resources, with an attempt to move towards left side of the continuum on Student-centered, Problem-based, Integrated, Community-based, Elective driven, and Systematic as already suggested by Khoshhal and Giuraya.[16] In the present study, learning style of the medical students was not consistent across year levels; a finding against the results of a survey done on physiotherapy students.[17] Different science disciplines, ethnic groups, admission policies, or resources may reflect this variance. Due to cross-sectional nature of the study, we could not follow the same cohort of students across the years, which might have affected outcome.
Although LSQ has been applied for assessing medical students’ learning styles, to our knowledge, the present study is the first application of this instrument in the Middle East region. A number of inventories have been applied at various centers for identifying the students’ learning styles. Lujan and DiCarlo used the visual, auditory, reading/writing, kinesthetic questionnaire to identify student's preferences for particular modes of information presentation.[18] Only 36% of the students preferred a single mode and 64% preferred multiple modes of information presentation. With active learning strategies, visual learners are facilitated by models and demonstrations.[19] Auditory learners are helped through discussions during peer instruction,[20] collaborative testing,[21] debate, games,[22] and interactive sessions.[23] The interest of kinesthetic and tactile learners is stimulated and provoked by manipulating models[24] and role playing.[25]
Accumulating evidence suggests that the critique against the LSQ, used in the study, doubts whether it meaningfully measures learning preferences or is it more accurately a personality questionnaire?.[13] A study reported that college students who were tested on their learning styles and were provided with an instructional session on how to apply their strengths and weaknesses based on their learning style, achieved higher academic results than other students.[26] Another survey of students from five disciplines of health-care profession (nursing, physiotherapy, occupational therapy, physician assistants, medical technology) reported a significant relationship between the student's self-reported learning style, as measured by Marshall and Merritt's LSQ, and their readiness to undertake SDL, using the Self-Directed Learning Readiness Scale.[27] The results showed that students reporting preference for converger learning styles were significantly more self-directed than other learning style preferences (F = 25.43; df = 3; P < 0.001). Rezler and French Learning Preferences Inventory examined the learning styles of the medical students of United Arab Emirates University.[28] The students learning preferences were teacher-structured learning activities, a fact matching the results of the present study.
Learning by adopting new learning styles by the individual learners may be facilitated by SDL.[29] This distinct learning mode has been shown to be associated with increased curiosity, critical thinking, quality of understanding, retention and recall, motivation, competence and confidence.[30] SDL empowers a learner to become a free, mature, and authentic ‘self’.[31] SDL has been successfully applied in a variety of learning contracts, problem-based curricula and distance learning packages.[32] At our institution, encouraging and promoting self-learning can partly change the learning styles of the students, from reflectors and theorists to pragmatists and activists, which may be the first step in improving the learning process. In addition, reviewing the content and design of the instructional materials (study guides, concept maps, ask-based/problem solving approach, and integration) can harvest desired changes in the learning styles of the medical students.
CONCLUSION
Understanding of the students’ preferred modes can enrich learning and facilitate the learning process. This study revealed that undergraduate medical students have significantly different learning styles; necessitating diverse teaching strategies to address various learning styles. There is a need to promote SDL and to modify instructional strategies of the existing curriculum, which may, in turn, influence the learning styles of the students towards the desired activists and pragmatists categories.
AUTHOR'S CONTRIBUTION
SSG conceived the idea, conducted the survey, collected results; SYG conducted statistical analysis, wrote the initial and final drafts of the manuscript, FAH translated the Arabic version of questionnaire and conducted the survey; KIKh translated the Arabic version of questionnaire and conducted survey. All authors reviewed the submitted drafts and actively participated in replying to the reviewers comments.
ACKNOWLEDGMENTS
The authors appreciate the contributions of all the students who completed the questionnaires. We also recognize the efforts of the secretarial staff in compiling the data for this research.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Cassidy S. Learning styles: An overview of theories, models, and measures. Educ Psychol. 2004;24:419–44. [Google Scholar]
- 2.Hu PJ, Hui W, Clark TH, Tam KY. Technology-assisted learning and learning style: A longitudinal field experiment. Systems, man and cybernetics. IEEE Trans Syst Man Cybern A Syst Hum. 2007;37:1099–112. [Google Scholar]
- 3.Brown T, Zoghi M, Williams B, Jaberzadeh S, Roller L, Palermo C, et al. Are learning style preferences of health science students predictive of their attitudes towards e-learning. Australas J Educ Technol. 2009;25:524–43. [Google Scholar]
- 4.Mon AA, Fatini A, Ye CW, Barakat MA, Jen PL, Lin TK. Learning style preferences among pre-clinical medical students. J Med Allied Sci. 2014;4:22–7. [Google Scholar]
- 5.Pask G. Styles and strategies of learning. Br J Educ Psychol. 1976;46:128–48. [Google Scholar]
- 6.Kolb DA. Experiential learning theory and the learning style inventory: A reply to Freedman and Stumpf. Acad Manage Rev. 1981;6:289–96. [Google Scholar]
- 7.Duff A, Duffy T. Psychometric properties of Honey and Mumford's Learning Styles Questionnaire (LSQ) Pers Individ Dif. 2002;33:147–63. [Google Scholar]
- 8.Swailes S, Senior B. The dimensionality of Honey and Mumford's learning styles questionnaire. Int J Sel Assess. 1999;7:1–11. [Google Scholar]
- 9.Curry L, Adams C. Patterns of learning style across selected medical specialties. Educ Psychol. 1991;11:247–77. [Google Scholar]
- 10.Honey P, Mumford A. Maidenhead, UK: Peter Honey; 2000. The Learning Styles Helper's Guide. [Google Scholar]
- 11.Hawk TF, Shah AJ. Using learning style instruments to enhance student learning. Decis Sci J Innov Educ. 2007;5:1–19. [Google Scholar]
- 12.Edward N. Evaluation of a constructivist approach to student induction in relation to students’ learning styles. Eur J Eng Educ. 2001;26:429–40. [Google Scholar]
- 13.Caple J, Martin P. Reflections of two pragmatists: A critique of Honey and Mumford's learning styles. Ind Commer Train. 1994;26:16–20. [Google Scholar]
- 14.Slater JA, Lujan HL, DiCarlo SE. Does gender influence learning style preferences of first-year medical students? Adv Physiol Educ. 2007;31:336–42. doi: 10.1152/advan.00010.2007. [DOI] [PubMed] [Google Scholar]
- 15.Groat A, Musson T. Learning styles: Individualizing computer-based learning environments. Res Learn Technol. 1995;3:53–62. [Google Scholar]
- 16.Khoshhal KI, Giuraya SS. Time to change the undergraduate curriculum at the college of medicine Taibah University. Br J Educ Soc Behav Sci. 2012;2:419–29. [Google Scholar]
- 17.Milanese S, Gordon S, Pellatt A. Profiling physiotherapy student preferred learning styles within a clinical education context. Physiotherapy. 2013;99:146–52. doi: 10.1016/j.physio.2012.05.004. [DOI] [PubMed] [Google Scholar]
- 18.Lujan HL, DiCarlo SE. First-year medical students prefer multiple learning styles. Adv Physiol Educ. 2006;30:13–6. doi: 10.1152/advan.00045.2005. [DOI] [PubMed] [Google Scholar]
- 19.Mayer RE, Massa LJ. Three Facets of Visual and Verbal Learners: Cognitive Ability, Cognitive Style, and Learning Preference. J of Educ Psychol. 2003;95:833–46. [Google Scholar]
- 20.Rao SP, DiCarlo SE. Peer instruction improves performance on quizzes. Adv Physiol Educ. 2000;24:51–5. doi: 10.1152/advances.2000.24.1.51. [DOI] [PubMed] [Google Scholar]
- 21.Rao SP, Collins HL, DiCarlo SE. Collaborative testing enhances student learning. Adv Physiol Educ. 2002;26:37–41. doi: 10.1152/advan.00032.2001. [DOI] [PubMed] [Google Scholar]
- 22.Howard MG, Collins HL, DiCarlo SE. “Survivor” torches “Who Wants to Be a Physician?” in the educational games ratings war. Adv Physiol Educ. 2002;26:30–6. doi: 10.1152/advan.00014.2001. [DOI] [PubMed] [Google Scholar]
- 23.Cortright RN, Collins HL, Rodenbaugh DW, DiCarlo SE. Student retention of course content is improved by collaborative-group testing. Adv Physiol Educ. 2003;27:102–8. doi: 10.1152/advan.00041.2002. [DOI] [PubMed] [Google Scholar]
- 24.Tanner K, Allen D. Approaches to biology teaching and learning: Learning styles and the problem of instructional selection – engaging all students in science courses. Cell Biol Educ. 2004;3:197–201. doi: 10.1187/cbe.04-07-0050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kuipers JC, Clemens DL. Do I dare? Using role-play as a teaching strategy. J Psychosoc Nurs Ment Health Serv. 1998;36:12–7. doi: 10.3928/0279-3695-19980701-12. [DOI] [PubMed] [Google Scholar]
- 26.Nelson B, Dunn R, Griggs SA, Primavera L. Effects of learning style intervention on college students retention and achievement. J Coll Stud Dev. 1993:364–9. [Google Scholar]
- 27.Linares AZ. Learning styles of students and faculty in selected health care professions. J Nurs Educ. 1999;38:407–14. doi: 10.3928/0148-4834-19991201-07. [DOI] [PubMed] [Google Scholar]
- 28.Paul S, Bojanczyk M, Lanphear JH. Learning preferences of medical students. Med Educ. 1994;28:180–6. doi: 10.1111/j.1365-2923.1994.tb02696.x. [DOI] [PubMed] [Google Scholar]
- 29.Shen WQ, Chen HL, Hu Y. The validity and reliability of the self-directed learning instrument (SDLI) in mainland Chinese nursing students. BMC Med Educ. 2014;14:108. doi: 10.1186/1472-6920-14-108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jennings SF. Personal development plans and self-directed learning for healthcare professionals: Are they evidence based? Postgrad Med J. 2007;83:518–24. doi: 10.1136/pgmj.2006.053066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Savin-Baden M, Major CH. McGraw-Hill International; 2004. Foundations of Problem-Based Learning. ISBN No. 0335 21531 9 (PB) [Google Scholar]
- 32.Dornan T, Hadfield J, Brown M, Boshuizen H, Scherpbier A. How can medical students learn in a self-directed way in the clinical environment? Design-based research. Med Educ. 2005;39:356–64. doi: 10.1111/j.1365-2929.2005.02112.x. [DOI] [PubMed] [Google Scholar]