

Abstract
Introduction:
Delivering drugs to ocular region is a challenging task. Eye physiological barriers lead to relatively less therapeutic and bioavailability effect by the conventional eye drops. This may be overcome by the use of in situ gel delivery system.
Objective:
The objective of our work was to formulate an ocular delivery system of levofloxacin, based on the concept of ion (sodium alginate) and pH (chitosan) activated in situ gelation concept. Due to its elastic properties, in situ gels resist the ocular drainage of drug leading to longer contact times with ocular surface.
Materials and Methods:
The formulation was evaluated for physicochemical characteristics, in vitro drug release. Ocular retention studies were carried out by Gamma scintigraphy. Time activity curve was plotted between marketed formulation and developed formulation for comparing drug drainage from the eye with time. Ocular tolerance test was performed by handheld infra-red camera.
Results and Discussion:
The formulations showed a first-order release pattern over 12 h. Both in vitro release studies and in vivo gamma scintigraphy precorneal retention studies indicated better therapeutic efficacy compared with standard eye drops.
Conclusion:
The results demonstrated that the developed in situ gel of levofloxacin is nonirritant, has prolonged action and is a better option in terms of retention, ocular bioavailability and patient compliance when compared with plain eye drops formulation.
KEY WORDS: Chitosan, gamma scintigraphy, in situ gel, levofloxacin, ocular tolerance, radiolabelling
In ocular delivery of medicaments, the physiological constraints imparted by the protective mechanisms of the eye lead to drainage from the eye, resulting in a short duration of the therapeutic effect. When a conventional eye drops is applied into the eye, the blinking action and effective tear drainage of the eye result in at least a 10-fold reduction in the drug concentration within 4–20 min.[1] We can improve the ocular therapy by improving the precorneal residence time of drugs. In order to slow down drug elimination and to prolong the resident time on the ocular surface, several new preparations have been developed for ocular use.[2,3] In situ gel-forming ocular drug delivery systems are one of them. In situ gel exhibits reversible phase transitions (sol–gel–sol) and pseudoplastic behavior to minimize drainage from blinking.[4] In situ gel is formulated as a liquid dosage form which is suitable to be administered as conventional eye drops which, upon exposure to eye physiological conditions, changes to the gel phase, thus increasing the precorneal residence time of the delivery system and enhancing ocular bioavailability.
There are different smart polymers, which convert to gel by various mechanisms. A combination of such polymers can provide better results than single polymer. However, in the present study, combination of sodium alginate and chitosan was prepared for use as ocular in situ gel-forming system. Alginate is a natural polysaccharide obtained from brown sea algae. It forms stable hydrogels in the presence of certain divalent cations present in tear secretion (e.g. Ca2+, Sr2+, and Ba2+) at low concentrations.[5,6] Sodium alginate is highly hydrophilic and biocompatible polymer, utilized in drug delivery.[7,8] It exhibits osmotically induced gelation, that is, gelling of the solution instilled is triggered by change in the ionic strength.[9] Chitosan is obtained naturally by deacetylation of chitin. It is nontoxic, biocompatible, mucoadhesive permeation enhancer and biodegradable polysaccharide.[10,11]
Levofloxacin, the active L-isomer of ofloxacin, is a fourth generation fluoroquinolone derivative and is used to treat acute and subacute conjunctivitis, bacterial keratitis, and keratoconjunctivitis.[12] Levofloxacin is available in the market as solid oral dosage form, oral solution, ophthalmic solution and an intravenous preparation. Its 0.5% and 1.5% solution is available as a sterile topical ophthalmic solution and is indicated for the treatment of corneal ulcer and bacterial ocular infections caused by susceptible strains.
The objective of the present study is to develop an ion and pH activated in situ gelling system of sodium alginate, and chitosan for levofloxacin, and its comparison with a plain eye drops formulation. The developed formulation was evaluated for physicochemical parameters such as clarity, viscosity, gelation pH along with in vitro drug release. The retention time and drug clearance rate of developed formulation were determined by gamma scintigraphy on albino rabbits. For studying gamma scintigraphy, the radiolabeling protocol for labeling levofloxacin with Tc-99m is also discussed.
Materials and Methods
The drug levofloxacin was received as a gift sample from Micro Labs Ltd., Bangalore, India. Chitosan (practical grade, 75–85% deacetylated, and molecular weight [MW] 150 kDa) was obtained as a kind gift from M/s, India Sea Foods, Cochin, India. Sodium alginate (MW 75–100 kDa) was purchased from CDH Labs, India. All other chemicals and solvents used were purchased from local suppliers and of analytical grade unless mentioned.
Preparation of levofloxacin in situ gel
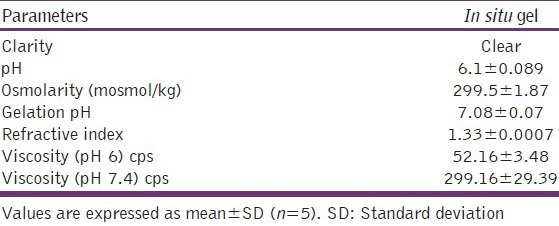
Different combinations of chitosan and sodium alginate were tested, and optimized composition was selected based on gelation and clarity [Table 1]. For antibacterial activity levofloxacin was prescribed in the dose range of 0.5–1.5% as solution. Hence, a dose of 0.5% was used in the formulation. The weighed quantity of drug was placed in a small beaker and dissolved primarily in 1–2 drops of acetone. Required quantity of polymer chitosan and sodium alginate were taken and mixed together with drug. A 0.1% of methyl paraben was added as a preservative [Table 2]. Osmolarity of the formulation was calculated by osmometer (Fiske Associates, USA) and required amount of sodium chloride was added and mixed thoroughly to make an isotonic solution. Formula of the complete developed formulation is given in Table 2. The physicochemical characterization of the formulation, that is, clarity, gelation pH, osmolarity and viscosity were measured and are tabulated in Table 3.
Table 1.
Different combinations evaluated for placebo in situ hydrogel formulation of levofloxacin
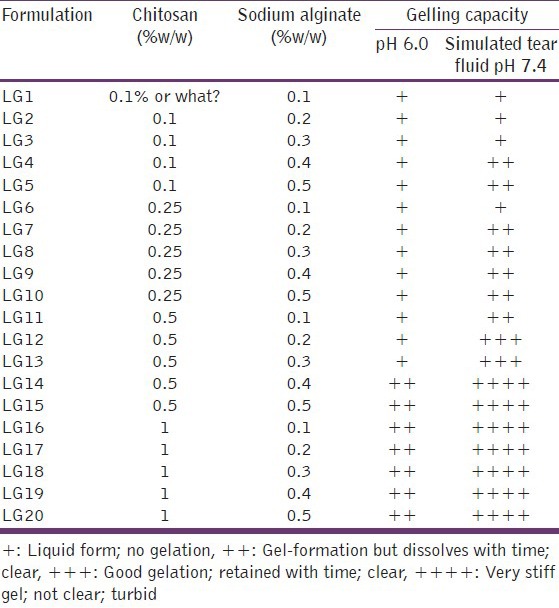
Table 2.
Ingredients of medicated formulation

Table 3.
Physicochemical properties of medicated in situ gel
In vitro drug release profile
In vitro drug, release was determined by the modified dialysis membrane technique. The 1 ml aliquots of the developed formulation and plain drug formulation were taken in the dialysis tube (Sigma Chemicals, USA), which were suspended in separate beakers. The beakers were then filled with 100 ml of the simulated tear fluid (STF), pH 7.4 with continuous stirring at 75 rpm at 37°C ± 0.5°C. Aliquots of 1 ml samples were withdrawn from the release medium at different time intervals and replaced with equal volumes of fresh media. Withdrawn samples were filtered and quantified for the drug content by ultraviolet spectrophotometry at 288 nm. Cumulative percent drug released was calculated. Results are shown in Figure 1.
Figure 1.
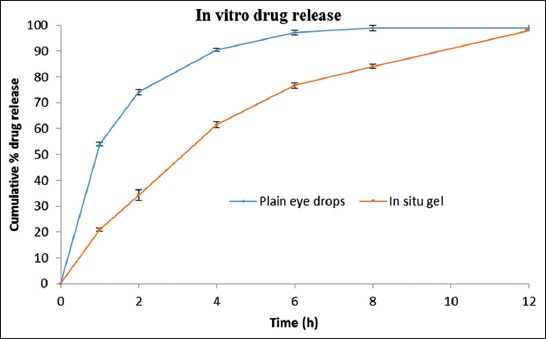
In vitro drug release of (blue) plain eye drops (orange) in situ gel
Ocular inflammation (infra-red camera)
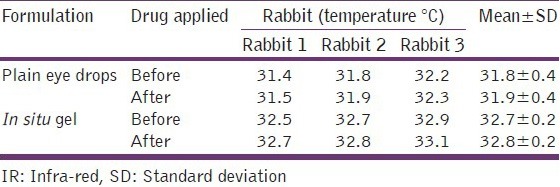
Ocular inflammation was evaluated using handheld infra-red (IR) camera. IR camera helps in evaluation of temperature increase on the surface if there is any inflammation after application. The temperature of the ocular surface was noted using hand operated IR camera before and after application of the formulation into the rabbit eye [Table 4].
Table 4.
IR camera readings for levofloxacin in situ gel-formulations
Gamma scintigraphy
Radiolabeling of levofloxacin with Tc-99m
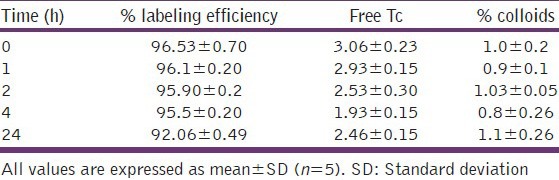
Radioactive nuclide 99mTc was attained as sodium pertechnetate in normal saline eluted from molybdenum generator was obtained from the regional center of the Board of Radiation and Isotopes Technology, INMAS, Delhi, India. For labeling purpose, a 2.5 mg of the levofloxacin was dissolved in normal saline and mixed with stannous tartrate (1 mg/ml in 10% acetic acid). The pH of the solution was adjusted by NaHCO3. 99mTc (2–3 mci) was added and mixed properly. All the labeling operation was carried out in hot laboratory under lead shielding. Labeling efficiency was evaluated using instant thin-layer chromatography (ITLC) as per our previously reported method.[13] Briefly, a drop of formulation was applied on ITLC silica-gel-coated strips and run in 100% acetone as mobile phase. While pyridine–acetic acid–water (PAW = 3:5:1.5 v/v) was used as mobile phase for reduced/hydrolyzed 99mTc (colloids). The strips were dried and cut into two equal halves and radioactivity was counted in each half using well-type gamma counter (CAPRAC-R, Capintec, USA). Amount of reducing agent stannous tartrate (SnC4H4O6 concentration) and the pH of the solution are the two factors on which labeling efficiency of drug molecules depend. Therefore, to attain maximum labeling efficiency, the two process variables were optimized. Labeling operation was carried out using different concentrations of stannous tartrate while keeping the pH constant. Labeling efficiency was determined as described previously [Table 5]. In another set of experiments, the amount of stannous tartrate was kept constant and the pH of the solution was varied from 5 to 7.5 by adding 0.5-M NaHCO3 solution. The labeling efficiency at different pH was determined and optimum pH was selected [Table 6]. In vitro stability of the labeled formulations was evaluated by ITLC. A 100 ml aliquot of the labeled formulation was mixed with 2.0 ml of phosphate-buffered saline (pH 7.4) and incubated at room temperature; change in labeling efficiency was monitored over a period of 24 h by ITLC as described above [Table 7].[13]
Table 5.
Effect of SnC4H4O6 on labeling efficiency of levofloxacin
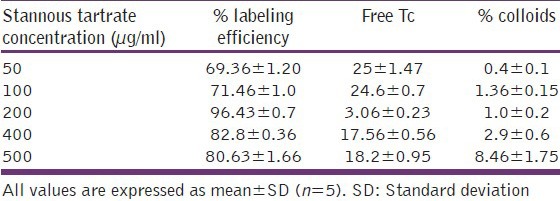
Table 6.
Effect of pH on labeling efficiency of levofloxacin
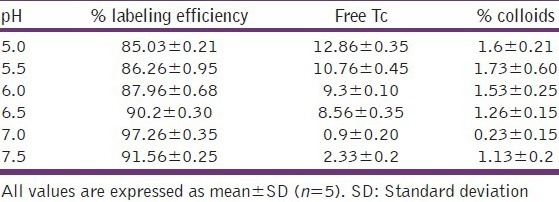
Table 7.
In vitro stability of levofloxacin labeled formulation
Gamma scintigraphy
In vivo precorneal drainage of the developed formulation was assessed by gamma scintigraphy. Albino rabbits of either sex weighing 2–3 kg were used for the study. Animals were procured from the animal house of INMAS (Delhi, India) and having free access to food and water. The study was carried out under the guidelines compiled by CPCSEA (Committee for the Purpose of Control and Supervision of Experiments on Animals, Ministry of Culture, Govt. of India) and all the study protocols were approved by local institutional Animal Ethics committee. Utmost care was taken to ensure that animals were treated in the most human and ethically acceptable manner. Weighed amount of levofloxacin was radiolabeled with Tc-99m by direct labeling method using stannous tartrate as the reducing agent. This radiolabelled drug solution was then mixed with other ingredients in such a way that the final solution would contain 0.5% w/v levofloxacin and required concentration of polymers. Gamma camera (Millenium VG, USA), autotuned to detect the 140 KeV radiation of Tc99m was used for scintigraphic study. Rabbits were anaesthetized using ketamine HCl injection given intramuscularly in a dose of 15 mg/kg body weight. The rabbits were positioned 5 cm in front of the probe and 25 ml of the radiolabelled formulation (100 mci) was instilled onto the left corneal surface of the rabbits. Recording was started 5 s after instillation and continued for 30 min using 128 × 128 pixel matrix. Individual 60 frames (60 s × 30 s) were captured by dynamic imaging process. Region of interest was selected on the one frame of the image and time-activity curve was plotted to calculate the rate of drainage from eye. A single whole body static image was also taken after 2 h of instillation of formulations.
Stability studies
Stability studies were carried out on optimized formulation according to ICH Guidelines at 40°C, 75% relative humidity. Three packs of formulations were subjected to these stability studies. The samples were withdrawn at 0, 30, 60 and 90 days. Every time 0.1 ml of samples were withdrawn and analyzed for assay with UPLC.[14] The logarithms of percent drug remaining were calculated and plotted against time (in days). The degradation rate constant (K) was deduced with equation slope = K/2.303.
Results
Based on physical examination (for appropriate viscosity, clarity and flow property), among the different combination tested [Table 1], a combination of 0.5% chitosan with 0.2% of sodium alginate is selected in situ gel base. Levofloxacin is prescribed in a concentration of 0.5% in marketed formulation, so we also used the same concentration for developed in situ gel system and plain drug eye drops [Table 2]. The developed formulations were further characterized for various physiological parameters, like clarity, gelation pH, viscosity and osmolarity. The optimized formulation was iso-osmotic (~300 mosmol) and the gelation pH was found to be near 7 [Table 3].
In in vitro drug release study, the formulation demonstrates a slow release rate. Initially rapid release (burst effect) was observed, gradually approaching slow and constant release for the rest of the time [Figure 1]. The best fit kinetic model was matrix model (R = 0.9831, K = 4.174, t-test = 16.12 (passes). The IR camera readings [Table 4] do not show any sudden change in corneal surface temperature showing no signs of inflammation.
Gamma scintigraphy is a technique whereby the transit of a dosage form through its intended site of delivery can be noninvasively imaged in vivo via the judicious introduction of an appropriate short-lived gamma-emitting radioisotope. Levofloxacin was successfully labeled with 200 μg stannous tartrate at pH 7.0 with a labeling efficiency of 96.43% [Tables 5 and 6]. At these conditions minimum colloids (<1.2%) were produced. In vitro stability of the labeled complex was also checked, and the complex was found to be stable for up to 24 h [Table 7].
The observation of the acquired gamma camera images showed that the formulation distributed evenly over the entire precorneal area without spillage for developed in situ gelling system [Figure 2b] immediately after administration when compared with plain eye drop formulation [Figure 2a]. The curve of the remaining activity on the corneal surface as a function of time (time-activity curve) was generated as shown in [Figure 3]. Plain eye drops formulation cleared very rapidly from the corneal region and reached in to systemic circulation through nasolacrimal drainage system as significant activity was recorded in kidney and bladder after 2 h of ocular administration [Figure 2a], whereas Chitosan and sodium alginate based in situ gel was cleared at slow rate and retained at corneal surface for longer duration. No countable radioactivity was observed in the systemic circulation (kidney and bladder), [Figure 2b]. Further, viscosity of chitosan is increased as the pH of the formulation is raised (>7) upon instillation into eye as a result of buffering action of the tear fluid.
Figure 2.
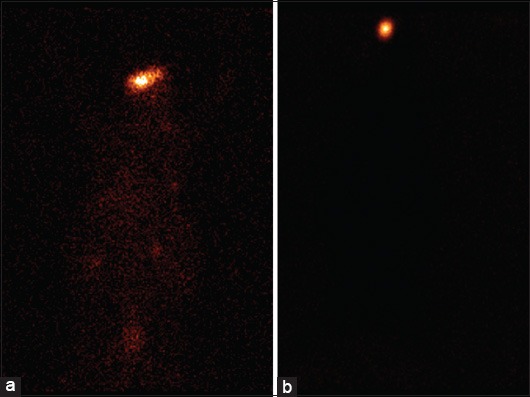
Static images of rabbits after formulation instillation (a) plain eye drops formulation (b) in situ gel
Figure 3.
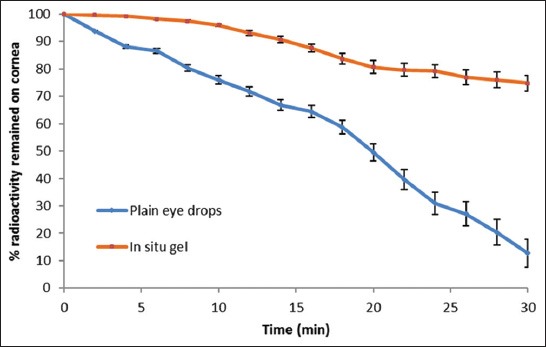
Gamma scintigraphy dynamic study (blue circle) plain eye drop formulation (orange square) developed in situ gel-formulation of levofloxacin
Stability studies
There were negligible alterations in the initial values of viscosity of the formulations over storage of 180 days. The samples were also analyzed for drug content by UPLC analysis.[14] Again the drug degraded to a negligible extent, and the percentage of drug degradation is < 5%. The degradation constant was found to be 1.13 × 10 − 4 at 40°C.
Discussion
Chitosan is a natural, biodegradable polymer and acts as a mucoadhesive permeation enhancer. Chitosan remains in the liquid state at pH 5–6 but gets converted to gel at pH 7.0. These properties make the chitosan as an ideal polymer for in situ formulation. Sodium alginate, the sodium salt of alginic acid, is a natural hydrophilic polysaccharide containing two types of monomers, β-d-mannuronic acid and α-l-guluronic acid. The polymer forms three dimensional hydrogel matrices and the high l-guluronic acid content alginate forms a low viscosity, free-flowing liquid at concentrations suitable for gel-formation in the lacrimal fluid.[15] Alginate transforms into a stable gel upon exposure to divalent cations, which is not easily eroded by tear fluid. A combination of 0.5% of chitosan and 0.2% of sodium alginate was used for preparation of the present formulation.
Different combination of chitosan and sodium alginate were developed which were evaluated for their physicochemical characteristics like physical appearance and gelling capacity at formulation pH 6.0 and at ocular pH 7.0 [Table 1]. It is prerequisite for an in situ gel system that it allows easy instillation into the eye as liquid drops and undergoes sol–to–gel transition, triggered by the rise in pH and presence of ions. A concentration of 0.5% of chitosan and 0.2% sodium alginate was selected as it gives a colorless and transparent formulation at formulation pH [Table 1], and provides good gelling formulation at ocular pH imparting prolong resident time in cul-de-sac with no compromise with vision.
A medicated formulation was prepared from the selected placebo formulation. A dose of 0.5% of levofloxacin is prescribed for ocular antibacterial therapy hence we also used the same concentration in our present formulation. 0.1% methyl paraben was added as preservative and NaCl was added in calculated amount to maintain isotonicity of the formulation. Final formula was given in Table 2.
Chitosan is insoluble at neutral and alkaline pH and converted into hydrogel when the pH of the formulation is raised from pH 6 to pH 7.4. On the other side sodium, alginate formed a stiff gel on interacting with divalent cations present in STF. This dual mechanism results in a good stiff gel upon providing eye physiologic conditions. Optimized formulation thus exhibited pseudoplastic viscosity that is dependent on the polymer concentration.
In vitro drug release profile of the marketed formulation and developed formulation were determined in STF (pH 7.4) and the formulation revealed a slow release rate. Initially rapid release (burst effect) was observed, gradually approaching slow and constant release for the rest of time. This pattern confirms the controlled release behavior of the formulation. The initial burst effect is beneficial for antibiotics as it helps achieving the therapeutic concentration of drug in minimal time followed by constant release to maintain sustained and control release of the drug. Developed formulation displayed 34.18% cumulative drug release after 2 h. 76.68% after 6 h and 84.08% after 8 h as compared to rapid release of 74.13% release in first 2 h followed by 97.2% release in 6 h drug from the plain eye drops formulation, Figure 1. Burst effect might be due to initial migration of the drug toward the surface of the matrix. Curve fitting of in vitro release data of optimized formulation was compared with different release model to select best fitting model using PCP Disso V 3.0 software, confirming matrix release mechanism of drug release from in situ gel. Chitosan is a cationic polymer which forms bonds with anionic nature of conjunctiva. In vitro transcorneal permeation studies on developed formulation reveal the well-known bioadhesive and permeation enhancer property of chitosan. On the basis of IR camera analysis [Table 4], we can say that the formulation is nonirritant and is well tolerated.
For scintigraphic studies, levofloxacin was radiolabeled with radionuclide Tc-99m. It was selected as it emits low energy gamma rays which do not lead to serious health hazards. The complex was found to be stable for up to 24 h. Marketed formulation cleared very rapidly from the corneal region and reached into systemic circulation via nasolacrimal drainage system as detectable activity was recorded in kidney and bladder after 2 h of ocular administration [Figure 2a], whereas Chitosan and sodium alginate based formulation was cleared at slow rate and retained at corneal surface for longer duration. No significant radioactivity was observed in the systemic circulation (kidney and bladder), [Figure 2b]. The curve of the remaining activity on the corneal surface as a function of time (time-activity curve) was plotted and is shown in Figure 3. Chitosan is both viscous and bioadhesive. Further, viscosity of chitosan/sodium alginate in situ gel is raised upon instillation into the eye due to the interaction with divalent cations present in the tear fluid and its pH (>7.2).
Many factors affect the stability of a pharmaceutical product, including the stability of the active ingredient (s); the potential interaction between active and inactive ingredients; to calculate shelf life of the formulation, extensive stability data are collected according to the ICH guidelines. Again the drug degraded to a negligible extent and the degradation rate constant for optimized formulation at 40°C was low (1.13 × 10 − 4). Because the overall degradation is <5%, a tentative shelf life of 2 years may be assigned to the optimized formulation.
Conclusion
The objective of the present research work was to develop a sustained release ocular drug delivery system with improved patient compliance and longer precorneal resistance time. Based on in vitro and in vivo characterization, we concluded that the developed in situ gelling formulation is a nonirritant, nontoxic sustained release formulation system for sustained topical drug delivery to eyes. This new formulation of levofloxacin is a viable option for effective and controlled management of conjunctivitis and other eye related disorders. The drug was intact and stable in the in situ gelling formulation during storage with the shelf life of ~ 2 years.
Acknowledgments
Authors are thankful to Council of Scientific and Industrial Research (CSIR), Govt. of India, New Delhi to provide Senior Research Fellowship to Mr. Himanshu Gupta.
Footnotes
Source of Support: Author Himanshu Gupta was awarded Senior Research Fellowship from Council of Scientific & Industrial Research (CSIR), Delhi, India to carried out this work
Conflict of Interest: None declared.
References
- 1.Maurice DM. Kinetics of topically applied drugs. In: Saettone MS, Bucci P, Speiser P, editors. Ophthalmic Drug Delivery: Biopharmaceutical, Technological and Clinical Aspects. Vol. 11. Padova: Fidia Research Series, Liviana Press; 1987. pp. 19–26. [Google Scholar]
- 2.Bourlais CL, Acar L, Zia H, Sado PA, Needham T, Leverge R. Ophthalmic drug delivery systems – Recent advances. Prog Retin Eye Res. 1998;17:33–58. doi: 10.1016/s1350-9462(97)00002-5. [DOI] [PubMed] [Google Scholar]
- 3.Ding S. Recent developments in ophthalmic drug delivery. Pharm Sci Technol Today. 1998;1:328–35. [Google Scholar]
- 4.Liu Z, Li J, Nie S, Liu H, Ding P, Pan W. Study of an alginate/HPMC-based in situ gelling ophthalmic delivery system for gatifloxacin. Int J Pharm. 2006;315:12–7. doi: 10.1016/j.ijpharm.2006.01.029. [DOI] [PubMed] [Google Scholar]
- 5.Wang ZY, Zhang QZ, Konno M, Saito S. Sol-gel transition of alginate solution by addition of various divalent cations: 13C-NMR spectroscopic study. Biopolymers. 1993;33:703–11. [Google Scholar]
- 6.Honghe Z. Interaction mechanism in sol-gel transition of alginate solutions by addition of divalent cations. Carbohydr Res. 1997;302:97–101. [Google Scholar]
- 7.Séchoy O, Tissié G, Sébastian C, Maurin F, Driot JY, Trinquand C. A new long acting ophthalmic formulation of carteolol containing alginic acid. Int J Pharm. 2000;207:109–16. doi: 10.1016/s0378-5173(00)00539-1. [DOI] [PubMed] [Google Scholar]
- 8.Hervas MJ, Holgado MA, Fini A, Fell JT. In vitro evaluation of alginate beads of a diclofenac salt. Int J Pharm. 1998;163:23–34. [Google Scholar]
- 9.Abraham S, Furtado S, Bharath S, Basavaraj BV, Deveswaran R, Madhavan V. Sustained ophthalmic delivery of ofloxacin from an ion-activated in situ gelling system. Pak J Pharm Sci. 2009;22:175–9. [PubMed] [Google Scholar]
- 10.George M, Abraham TE. Polyionic hydrocolloids for the intestinal delivery of protein drugs: Alginate and chitosan – A review. J Control Release. 2006;114:1–14. doi: 10.1016/j.jconrel.2006.04.017. [DOI] [PubMed] [Google Scholar]
- 11.Patel V, Patel M, Patel R. Chitosan: A unique pharmaceutical excipients. Drug Deliv Technol. 2005;5:1–12. [Google Scholar]
- 12.Chen T, Embree HD, Brown EM, Taylor MM, Payne GF. Enzyme-catalyzed gel formation of gelatin and chitosan: Potential for in situ applications. Biomaterials. 2003;24:2831–41. doi: 10.1016/s0142-9612(03)00096-6. [DOI] [PubMed] [Google Scholar]
- 13.Gupta H, Aqil M, Khar RK, Ali A, Bhatnagar A, Mittal G, et al. Development and characterization of 99mTc-timolol maleate for evaluating efficacy of in situ ocular drug delivery system. AAPS Pharm Sci Tech. 2009;10:540–6. doi: 10.1208/s12249-009-9238-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gupta H, Aqil M, Khar RK, Ali A, Chander P. A single reversed-phase UPLC method for quantification of levofloxacin in aqueous humour and pharmaceutical dosage forms. J Chromatogr Sci. 2010;48:484–90. doi: 10.1093/chromsci/48.6.484. [DOI] [PubMed] [Google Scholar]
- 15.Nagarwal RC, Kant S, Singh PN, Maiti P, Pandit JK. Polymeric nanoparticulate system: A potential approach for ocular drug delivery. J Control Release. 2009;136:2–13. doi: 10.1016/j.jconrel.2008.12.018. [DOI] [PubMed] [Google Scholar]