

Abstract
Adolescent sexually transmitted infection (STI) and birth rates indicate a need for effective middle school HIV/STI, and pregnancy prevention curricula to delay, or mitigate consequences of, early sexual activity. Individual and organizational barriers to adoption, implementation, and maintenance, however, can hamper dissemination of evidence-based sexual health curricula, adversely impacting fidelity and reach. Internet-based approaches may help mitigate these barriers. This paper describes the development and feasibility testing of It’s Your Game (IYG)-Tech, a stand-alone 13-lesson Internet-based sexual health life-skills curriculum adapted from an existing effective sexual health curriculum—It’s Your Game… Keep it Real (IYG). IYG-Tech development adaptation steps were to: 1) Select a suitable effective program and gather the original program materials; 2) Develop “proof of concept” lessons and test usability and impact; 3) Develop the program design document describing the core content, scope, and methods and strategies; and 4) produce the new program. Lab- and school-based tests with middle school students demonstrated high ratings on usability parameters and immediate impact on selected psychosocial factors related to sexual behavior—perceptions of friends’ beliefs, reasons for not having sex, condom use self-efficacy, abstinence intentions, negotiating with others to protect personal rules, and improved knowledge about what constitutes healthy relationships (all p < .05). Youth rated IYG-Tech is favorably compared to other learning channels (>76.2% agreement) and rated the lessons as helpful in making healthy choices, selecting personal rules, detecting challenges to those rules, and protecting personal rules through negotiation and refusal skills (89.5% – 100%). Further efficacy testing is indicated for IYG-Tech as a potential strategy to deliver effective HIV/STI, and pregnancy prevention to middle school youth.
Keywords: Adolescents, Web-Based Health Education, Computer-Based Health Education, Health Communications, School-Based Health, Sexual Health
1. Introduction
Adolescent births and sexually transmitted infections (STIs) represent serious public health concerns in the United States. Despite recent declines, the 2012 birth rate of women 15 – 19 years of age is 29.4 births per 1000 in the United States (Martin et al., 2013). The prevalence rate for at least one STI is 24.1% among adolescent females (aged 14 – 19 years) (Forhan et al., 2009) and 37.7% among those who are sexually experienced. These statistics substantiate the need for effective HIV, STI, and pregnancy prevention interventions for adolescents, beginning at the middle school level. There are at least five sexual health programs developed for use in the middle school setting with demonstrated effectiveness at delaying sexual behavior among middle school students (USDHHS, 2013). Despite this, many students are not receiving timely sexual health education (Martinez et al., 2010; Darroch et al., 2000) and many middle and high schools are not implementing evidence-based programs (Kirby, 2002) or requiring pregnancy and HIV prevention as health topics (Kann et al., 2007). Irrespective of their effectiveness, dissemination of such programs may be hampered due to barriers at the level of the program, individual, or organization (Kirby, 2007; Rolleri, et al., 2008; Noar et al., 2009).
Program barriers may include the difficulty to locate, obtain, and implement programs (Johnson, unpublished; Burlingame, 2011) or lack of sufficient training from program developers (Schaalma, 2004: 32; CDC, 2011: 57). Individual instructor barriers may include lack of awareness or confusion regarding education policies (Levesque, 2000; Peskin 2011), length of service in teaching related to resignation to attempt implementation (Markham, 2002: 40), lack of skills and self-efficacy for teaching and adapting programs with fidelity or negative attitudes towards “science-based” approaches (Rolleri et al., 2008; Buston, 2002). Organizational barriers include concerns of school officials about negative community reactions and perceived controversy of sex education (Landry et al., 2003), perceived lack of support from internal (e.g. administrator) or external (e.g. parent) stakeholders to teach sexual health (Rolleri et al., 2008; Peskin, 2014), pressure to devote class time to academic priorities rather than health topics, and lack of funds for purchasing, training, and implementing programs (Rolleri et al., 2008). A curriculum accessed through the Internet that includes individual interactive student activities can potentially address these program, individual, and organizational barriers by providing a channel to confidentially address sensitive material in a way that optimizes program fidelity (provided all lessons are received) in an easily accessible way that requires minimal teacher training and cost.
Policy and infrastructure initiatives are improving Internet connectivity to schools. Despite variability in reliable connectivity and bandwidth the Internet is a timely dissemination channel for sexual health interventions that promise to be educationally effective, cost-effective, and of high fidelity (National Center for Education Statistics, 2008). Evaluations of a computer-based sexual health intervention for high school students have demonstrated significant increases in knowledge regarding pregnancy, condom self-efficacy, attitudes toward abstinence, and perceived HIV susceptibility (Roberto et al., 2005), as well as decreases in frequency of sexual intercourse and number of sexual partners (Lightfoot et al., 2007). Recent literature reviews have indicated the efficacy of computer-based applications in impacting health behavior change in youth (Papastergiou, 2009; Primack et al., 2012; Hieftje et al., 2013). Methods describing the adaptation of effective group-based programs into programs delivered primarily by computer have been described (Card et al., 2011a, 2011b). The push for dissemination of evidence-based programs and the concurrent up swell in the potential of eHealth applications for behavioral change suggests the utility of adapting existing conventional programs to electronic channels.
IYG-Tech, a 13-lesson Internet-based curriculum, was adapted from It’s Your Game… Keep it Real (IYG), an effective middle school sexual health curriculum that has been shown to delay sexual behavior in two randomized trials (Tortolero, 2010; Markham, 2012). Adaptation challenges included ensuring that original learning objectives were fully represented, that a new Internet-based functionality of the original computer-based lessons could be achieved, and that the newly developed “proof-of-concept” lessons and prototype curriculum were acceptable to end users, feasible for delivery in the middle school setting, and impactful of determinants of sexual behavior. The purpose of this article is to describe a pragmatic and empirically-based adaptive development of IYG-Tech and results of usability and feasibility testing to determine readiness for school-based dissemination for efficacy testing. The empirical process described has broader implications for those interested in adapting existing evidence-based sexual health programs into computer-based applications.
2. Developmental Process: Methods and Results
Systematic translation frameworks informed our adaptation and development process, providing guidance on the incorporation of theoretically and empirically-based evidence (Bartholomew, 2006; Card, 2011b; Wingood & DiClemente, 2008). The development of the Internet-based HIV, STI, and pregnancy prevention curriculum (IYG-Tech) comprised two phases: 1) Adaptation of an existing hybrid (classroom/computer) evidence-based program (It’s Your Game… Keep it Real) into a completely Internet-based curriculum, and 2) Evaluation of the new program in a feasibility pilot test. The Adaptation phase approximated the stepped sequence described by Card et al. (2011) and the development of behavioral change matrices in the Intervention Mapping approach described by Bartholomew et al. (2006). An active participatory research process was instituted in accordance with the adaptation frameworks where a teen-advisory board provided information and advice regarding the translation of existing lessons and the development of new activities in consecutive meetings throughout the development phases.
2.1. PHASE 1: Adaptation
In the context of IYG-Tech Project the adaptation steps included to (Figure 1):
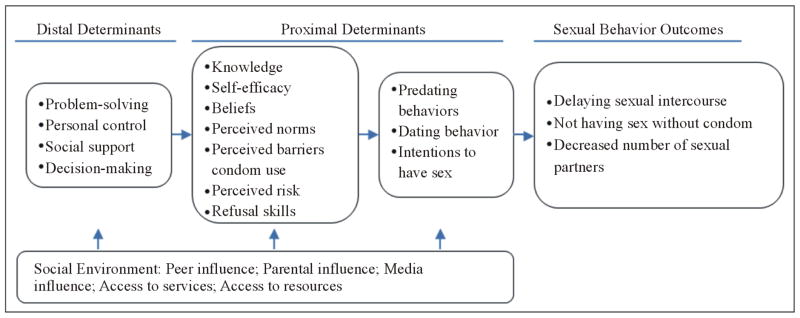
Figure 1.

Conceptual framework of behavioral determinants and outcomes for IYG.
Select a suitable effective program and gather the original program materials;
Develop “proof of concept” lessons and testing usability and impact;
Develop the program design document describing the core content, scope, and methods and strategies; and
Produce the new program.
Step 1. Select a suitable effective program and gather the original program materials
Adaptation is optimized through consultation with the original developers and assets of the original intervention (Card, 2011). The IYG-Tech curriculum was adapted from It’s Your Game… Keep It Real (IYG), an effective HIV, STI, and pregnancy prevention curriculum designed for middle school youth. IYG had demonstrated effectiveness in significantly delaying sexual initiation among sexually inexperienced students in two randomized controlled trials (Markham et al., 2012; Tortolero et al., 2010). Based on social cognitive theory (Bandura, 1985), social influence models (Komro et al., 2001; Perry, 1999; Story et al., 2002), and the theory of triadic influence (Flay & Petratis, 1994), IYG comprises 24 lessons—12 lessons each in 7th and 8th grade (Figure 2). For each grade level, IYG integrates 8 lessons of group-based classroom activities (e.g., role plays, small group discussion, and personalized journaling) and 4 lessons of computer-based, tailored multimedia activities (Shegog et al., 2007). A life-skills decision-making paradigm (Select, Detect, Protect) underlies all IYG activities, teaching students to select personal rules regarding risk behaviors, to detect signs or situations that might challenge these rules, and to use refusal skills to protect these rules. The IYG curriculum research and development team worked on the adaptation process for IYG Tech, following validated development protocols, informed by empirical findings from the target population, and existing computer lesson assets.
Figure 2.
Conceptual framework of behavioral determinants and outcomes for IYG.
Step 2. Develop “proof of concept” lessons and test usability and impact
A proof-of-concept is the demonstration of a preliminary design and/or prototype used to test the feasibility of a program or product before it is more fully developed. While shown effective, the randomized controlled trials of IYG were unable to provide information on the relative effects of program components such as group process, individual computer lessons, and journaling activities. Prior to developing IYG-Tech, a usability study was conducted to determine the immediate psychosocial impact of the original 8 IYG computer-based lessons in order to understand the needed scope for a broader computer-based curriculum. These lessons were redesigned as a “proof-of-concept” for an Internet-based application to determine acceptability and feasibility of adjustments in look, feel, and functionality.
2.2. Translation of Existing Computer-Based Activities to an Internet Delivery Platform
The original computer-based lessons of the IYG curriculum had been delivered from the hard drives of dedicated laptop computers. The original IYG interface featured a 3-dimensional (3-D) virtual “mall” with first-person “shooter” navigation game dynamics. Increasing the dissemination potential of the program necessitated changes to the lesson interface, file compression, and image resolution. A “proof-of-concept” was developed to establish that original lesson content could be translated to minimize platform and bandwidth and to optimize Internet accessibility to schools. The look and feel of the original 3-D IYG mall interface and the active user control over navigation was replaced with a 2-dimensional (2-D) Flash-based interface and passive automatic user relocation within the IYG “mall” environment. Video components were compressed in size and embedded in Adobe Flash format to optimize accessibility, with some degradation of resolution, and interactive 3-D elements were replaced with 2-D Flash interactive elements.
2.3. Usability Testing
Study Design and Participants
A single-group, pre-test/post-test usability study of the 8 “proof-of-concept” Internet-adapted IYG lessons was conducted at two local community organizations and at a large university in southeast Texas, with a convenience sample of 7th- and 8th-grade students (N = 33), 12 – 14 years of age (Mage = 13.9 ± 1.14 years), primarily female (58%), and African American (70%), recruited through local public middle schools in a large, urban school district in southeast Texas and through the university. The sample size was consistent with usability testing protocols that do not require statistical significance to determine major usability problems (Nielsen, 1993). Participation was voluntary; written parental consent and child assent were obtained. The study was approved by The University of Texas Health Science Center at Houston institutional review board (HSC-SPH-07-0251).
Study Protocol
The youth accessed all 8 lessons in a single day (one of three consecutive Saturdays) in a simulated classroom setting using laptop computers with headphones. Youth completed pre-tests (demographic, psychosocial, and attitudinal surveys) and then completed each lesson individually. At the end of each lesson, each student completed usability questionnaires regarding that lesson. Students also completed usability assessments of the lessons as a whole. Upon completion of all lesson activities, students also completed psychosocial and attitudinal surveys (post-tests) that were administered via the same laptop computers. Sessions were observed by study personnel who documented any problems (technical or content-related) and provided assistance as required. Students received a $50 gift card for their participation. Breakfast, lunch, and between-lesson breaks were provided. Compensation was also provided to external staff whose presence was needed at community organization sites.
Measures and analysis
Usability
Usability parameters including likability, credibility, acceptability, understandability, ease of use, motivational appeal, and perceived impact were assessed using adapted Likert scale ratings and open-ended response formats (Shegog et al., 2007). Likability was based on how much the youth liked different lesson activities and program elements entire program, pictures/colors, sounds, buttons, cartoons, videos, transitions using 5-point Likert scale ratings, ranging from “dislike a lot” to “like a lot”. Credibility was based on the perceived correctness of the content presented using a 3-point Likert scale rating of “right,” “wrong”, and “don’t know” and whether the content could be trusted (“yes”, “no”, and “don’t know”). Ease of use was based on perceived difficulty of the entire program and directions within the program (very easy, kind of easy, kind of hard, very hard) and if youth needed help from the teacher or another adult to use the Internet-adapted IYG lessons (yes, no). Understandability was based on whether youth could understand the words used (yes, no). Acceptability was based on the pace of Internet-adapted IYG activities (“too fast”, “just right”, “too slow”). Parameters of understandability of words used, motivational appeal (if youth would use these lessons again and recommend it to others), ease of use (if youth needed help from the teacher or another adult to use the adapted lessons), and perceived impact (if youth thought these lessons would help them make healthy decisions about friends and sexual relationships) were rated using a 3-point Likert scale (“yes”, “no”, and “don’t know”).
Psychosocial variables
Psychosocial mediators of sexual behavior were assessed to conduct exploratory tests of the impact of IYG-Tech and to establish feasibility for data collection and analysis for any impending efficacy field trial. The study sample, while sufficient for usability testing, is insufficiently powered to detect impact. However, exploratory analysis of mediators (which are the proximal targets of change) immediately subsequent to IYG-Tech provides an indication of the need for further lesson content above those in the original computer lessons. Psychosocial measures included beliefs about abstinence until marriage, beliefs about waiting to have sex, perceived friends’ beliefs about waiting to have sex, perceived friends’ sexual behaviors, reasons for and against having sex, self-efficacy to refuse sex, condom knowledge, condom attitudes, perceived friends’ beliefs about condoms, self-efficacy to use condoms, and perceived likelihood of having sex. All these psychosocial measures have been validated among multi-ethnic, urban-dwelling public school student populations (Basen-Engquist et al., 1999; Borawski et al., 2005; Coyle et al., 2004; Markham et al., 2012; Tortolero et al., 2010).
Attitudes toward computers for learning
Attitudes to computers were assessed to explore the impact of the IYG-Tech learning experience on global acceptance of computers as an educational medium. This is a broader measure of the motivational appeal of IYG-Tech, influencing the potential of seeing CAI in a new light. These attitudes were assessed using a 10-item survey, with a 3-point response scale and reported Cronbach’s alpha of .81 (Askar et al., 1992).
Usability measures were administered via paper-pencil surveys upon completion of relevant lessons. Psychosocial and attitudinal measures were administered via an audio-computer-assisted self-interview on laptop computers to enhance privacy and confidentiality. Data were analyzed using descriptive and inferential statistics (paired t-tests and sign tests), according to distribution assumptions, using SAS software (version 9.2).
Usability testing results
The resultant Internet-based lessons were 35 minutes in length and retained the original educational strategies of interactive 2-D exercises, quizzes, animations, peer videos, and fact sheets.
Usability
The Internet-adapted IYG lessons were rated as enjoyable (94%), easy to use (88%), and understandable (88%), with most students requiring no assistance (76%) (Table 1). Most students rated the lessons as credible (91%), useful in helping them to make healthy choices (91%), and of appropriate duration (66%). The ease of program directions, movement, and navigation were all highly rated (>90%). Most students indicated they would recommend the lessons to their classmates (79%), and some indicated they would do these lessons again (45%).
Table 1.
Participant usability ratings for the “proof-of-concept” lessons adapted for the Internet from the original 8 IYG computer lessons.
| Construct | Item | Feasibility results (range of rounded % agreement) |
|---|---|---|
| Likability (Like a little or a lot) | Entire program | 94 |
| Activities (n = 79 across all lessons) | n/a | |
| Pictures/colors | 94 | |
| Sounds | 88 | |
| Buttons | 94 | |
| Cartoons | 97 | |
| Videos | 97 | |
| Transitions | 94 | |
|
| ||
| Ease of use (kind of easy or very easy) | Entire program | 88 |
| Directions | 100 | |
|
| ||
| Credibility | Information is right (correct) | 91 |
| Information is trustworthy | 97 | |
|
| ||
| Acceptability | Duration/Time-on-task was “just right” | 66 |
|
| ||
| Understandability | Understands words | 88 |
| Needs help | 24 | |
|
| ||
| Motivational Appeal | Would recommend to my class | 79 |
| Would play again | 45 | |
|
| ||
| Perceived Impact | Helps make healthy choices | 91 |
Psychosocial Impact
Immediately after completing the Internet-adapted IYG lessons, students perceived their friends as having more positive beliefs about waiting to have sex, cited more reasons for not having sex, had greater self-efficacy to use condoms, and had greater intentions to abstain from sex until marriage (t(23 to 30) = 2.390 to 3.589, p < .05). Students also reported that learning from computers increased their confidence and was very enjoyable (t(22) = 2.121 to 2.912, p < .05), but they also reported that using computers did not make the time pass more quickly nor allow them to learn more quickly (t(22) = −2.237 to −2.206, p < .05; Table 2).
Table 2.
Change in psychosocial determinants of sexual behavior and attitudes toward computers for learning following exposure to internet-based IYG computer lessons.
| Psychosocial variable | n | Pre-test M (SD) |
Post-test M (SD) |
Change M (SD) |
t |
|---|---|---|---|---|---|
| Beliefs about abstinence until marriage | 28 | 3.01 (.65) | 2.94 (.78) | −.07 (.57) | −.664 |
| Beliefs about waiting to have sex | 31 | 3.20 (.61) | 3.22 (.61) | .02 (.55) | .163 |
| Perceived friends’ beliefs about waiting to have sex | 31 | 2.45 (.69) | 2.74 (.52) | .29 (.68) | 2.390* |
| Perceived friends’ sexual behaviors | 29 | 1.64 (.71) | 1.66 (.78) | .03 (.64) | .219 |
| Reasons for not having sex | 31 | 4.00 (2.38) | 5.19 (2.88) | 1.19 (1.85) | 3.589** |
| Reasons for having sex | 30 | .73 (.83) | .73 (1.43) | .00 (1.68) | .000 |
| Self-efficacy to refuse having sex | 26 | 3.19 (.65) | 3.24 (.73) | .05 (.69) | .407 |
| Condom knowledge | 31 | .68 (.35) | .75 (.33) | .08 (.36) | 1.157 |
| Condom attitudes | 30 | 3.28 (.68) | 3.14 (.98) | −.13 (.72) | −1.015 |
| Perceived friends’ beliefs about condoms | 29 | 2.87 (.81) | 3.03 (.92) | .16 (.89) | .097 |
| Self-efficacy to use condoms | 24 | 1.31 (.56) | 1.52 (.47) | .21 (.44) | 2.345* |
| Perceived likelihood of having oral sex in the next year | 31 | 1.90 (1.14) | 1.71 (1.24) | −.19 (.83) | −1.293 |
| Perceived likelihood of having vaginal sex in the next year | 31 | 1.84 (1.13) | 1.81 (1.33) | −.03 (.91) | −.197 |
| Perceived likelihood of abstaining until the end of high school | 29 | 3.12 (1.52) | 3.48 (1.72) | .28 (1.56) | .955 |
| Perceived likelihood of abstaining until marriage | 29 | 2.83 (1.61) | 3.59 (1.34) | .76 (1.22) | 3.363** |
|
| |||||
|
Attitude toward computers for learning
| |||||
| While studying computers, the time passes quickly. | 23 | 2.76 (.59) | 2.275 (.88) | −.39 (.84) | −2.237* |
| I learn quickly while studying with computers. | 23 | 2.80 (.77) | 2.448 (.78) | −.43 (.95) | −2.206* |
| I feel comfortable while studying with computers. | 23 | 2.76 (.52) | 2.586 (.68) | −.17 (.78) | −1.073 |
| Learning with computers increases my success. | 23 | 2.44 (.71) | 2.310 (.81) | −.13 (.87) | −.720 |
| Learning from computers increases my confidence. | 23 | 2.00 (.76) | 2.344 (.72) | .35 (.57) | 2.912** |
| Computers make me eager to study more. | 23 | 2.08 (.91) | 2.366 (.81) | .13 (.76) | .826 |
| At first, learning with computers seems enjoyable but later I am bored. | 23 | 2.12 (.78) | 2.266 (.78) | .04 (.71) | .295 |
| Instruction with computers is very enjoyable. | 23 | 1.92 (.86) | 2.413 (.78) | .48 (1.08) | 2.121* |
| I would like to learn all my school courses with computers. | 23 | 2.28 (.76) | 2.233 (.89) | −.04 (.93) | −.225 |
| I learn easily with colorful graphics and animation. | 23 | 2.44 (.82) | 2.466 (.78) | −.04 (.93) | −.225 |
Note:
All scales positively coded, except likelihood to have oral and vaginal sex.
p < .05,
p < .01.
The significant change observed in psychosocial mediators demonstrated the potential of the Internet adapted lessons. While positive, delivery of the Internet-based lessons impacted fewer psychosocial mediators than observed in the original field trial of the IYG curriculum (Tortolero, 2010). Additional mediators positively impacted in the field trial at 8th grade follow-up included more positive beliefs about abstinence, greater confidence in refusing sex, greater general knowledge about HIV and STIs, their symptoms, and using condoms to prevent them, exposure to fewer risky situations, fewer intentions to have oral sex in the next year, and greater intentions to remain abstinent through high school when compared to the comparison group (Tortolero, 2010).
Results of usability testing suggested that the “proof-of-concept” Internet-based lessons could be developed with acceptable usability ratings and positive impact despite down-grade from a 3-D interface in favor of reduced bandwidth. Usability ratings were similar to those of the original IYG computer program for credibility (91% vs. 92.9% for IYG), perceived effect of the program in helping make healthy choices (91% vs. 93% for IYG), and ease of use (88% – 100% vs. 78% – 100% for IYG). The adapted lessons rated lower on understandability (88% vs. 100% for IYG) with more students requiring assistance (24% vs. 0% for IYG). Conversely, appropriateness of time on task rated lower than the original IYG computer lessons (66% vs. 85.7% – 100% for IYG). A positive “by-product” of the current usability testing was the impact on attitudes toward technology for education in the classroom, a desirable but unexpected result from youth who are already sophisticated technology end-users. Collectively, these findings suggested the potential for the adapted Internet-based lessons as a feasible channel for sexual health education but that the original 8 IYG computer lessons would require supplemental content development to at least approximate the immediate impact of the original 24 lesson curriculum.
Step 3. Develop the program design document describing the core content, scope, and methods and strategies
A design document outlines the specifications (content, function, and flow) of a software product or, in the case of IYG-Tech, the proposed Internet-based curriculum. The design document, developed for the original IYG curriculum, to describe the program’s functionality, look and feel, screen maps, and scripts, was reviewed and amended to provide the “blue print” for production.
Content analysis of the original IYG curriculum helped to determine the scope of IYG-Tech. In the original IYG curriculum, the core content, scope, and best practice characteristics had been delineated using an Intervention Mapping (IM) process (Tortolero, 2010). These were represented in a series of behavioral change matrices, a product of the IM process, which cross-referenced targeted behavioral outcomes, performance objectives, behavioral mediators, and learning objectives (Bartholomew et al., 2006). Targeted behavioral outcomes for the original IYG curriculum included 1) abstinence from sex, and 2) maintenance of healthy relationships. These outcomes were also appropriate for all students, those who had not initiated sex, and also those who were sexually experienced but who could choose abstinence and healthy friendships in the future. Additionally, for sexually active youth, targeted behavioral outcomes included 3) correct use of condoms, 4) birth control, and 5) testing for HIV, STI, and pregnancy (Table 3). The original IYG curriculum was designed to impact psychosocial mediators related to these five behaviors which included knowledge, skills, self-efficacy, outcome expectations, perceived norms, normative beliefs, and social support. The IM matrices were reviewed by the IYG-Tech research team to determine the relevance and validity of the targeted behavioral outcomes and component behaviors (performance objectives), and behavioral mediators to current sexual health behaviors and determine whether modification or amendment would be required for the IYG-Tech version. The original matrices were found to be relevant to the new IYG-Tech program.
Table 3.
Targeted behavioral determinants of IYG-Tech.
All students
|
The learning objectives from the original IYG program (n = 193) were also reviewed by the research team to determine the extent to which each learning objective was covered in the original IYG lessons (whether full, partial, or limited/none) and in which types of lesson activities the learning objectives were covered (i.e. classroom and/or computer-based lessons). This analysis provided information on what content needed to be adapted to supplement the existing 8 IYG computer-based lessons. Of the 193 learning objectives listed in the original IYG planning matrices, 158 (88.9%) were covered in the 8 existing IYG computer lessons, either solely in the computer lessons (n = 82; 42.5%), more comprehensively in the computer lessons than the classroom (n = 23; 11.9%), or of equal comprehensiveness in the computer as in the classroom (n = 53; 27.5%) (Table 4). The classroom lessons provided the only content for 9 objectives (4.7%) and more comprehensive content for 26 objectives (13.5%) than provided on the computer. Learning objectives that were listed in the original IYG curriculum but required further focus in computer-based activity included skills training in refusing to have sex and avoiding unhealthy relationships (behavioral objectives 1 and 2), values clarification (e.g., setting one’s own personal limit with regard to sex, behavioral objectives 1 and 2), negotiating risk reduction strategies (e.g. negotiating condom use; behavioral objective 3), and health service utilization (e.g. getting STI testing if sexually active, behavioral objective 5).
Table 4.
Curriculum content analysis. Learning obectives covered by each lesson type.
| # | Category | Definition | Objectives n (%) |
|---|---|---|---|
| 1 | Classroom = computer | Equally in classroom and computer lessons | 53 (27.5) |
| 2 | Classroom only | In classroom but NOT in the computer | 9 ( 4.7) |
| 3 | Computer only | In the computer but NOT in the classroom | 82 (42.5) |
| 4 | Classroom > computer | More comprehensively in the classroom than in the computer | 26 (13.5) |
| 5 | Computer > classroom | More comprehensively in the computer than in the classroom | 23 (11.9) |
| Total | 193 (100.0) |
Specifications for IYG-Tech lesson activities were listed in one of four categories: 1) as computer-based activities from the original IYG curriculum that were already adapted for the Internet and needed no change (n = 95), 2) computer activities from the original IYG curriculum that were already adapted for the Internet but required some minimal modification (n = 73), 3) computer activities adapted from pre-existing classroom activities in the original IYG curriculum that would be new Internet-based activities (n = 13), and 4) newly created Internet-based activities (n = 158).
Theoretical methods (e.g. modeling and guided practice to address skills and self-efficacy) and practical strategies (e.g. interactive and non-interactive animations, role model video, serials, video-based and photo-based interactive activities) informed activity content. Dynamic between-activity transitions and fact sheets were developed where more expansive content focus was required (e.g., skills practice for using condoms). Other design document specifications included lesson number and format, flow charts, storyboards, and interface design. The IYG-Tech lessons included branched logic to tailor content based on student gender, sexual experience, and sexual intentions. For students who are not sexually experienced or have few intentions to engage in sexual activity peer videos were framed to include messages reinforcing continued abstinence. For students who are sexually experienced, peer videos were framed to reinforce initiation of abstinence, risk reduction strategies, and STI testing.
Development of the design documents was an iterative process with components being presented to the teen advisory board for review and feedback on the appropriateness of activity content and language for credibility, authenticity, and appropriateness. For example, youth feedback assisted in the development of more realistic refusal skills simulations that portrayed more persistent peer pressure than originally scripted.
Step 4. Produce the new program
IYG-Tech comprises 13 lessons designed to be accessible to 8th grade students. The curriculum length was guided by the need to provide adequate content, suitability of implementation in a typical school semester, and prior empirical data suggesting minimal optimal dose for behavior change to be 13 lessons (Markham et al., 2012). Lessons are developed in HTML5, are approximately 35 minutes in length, and include interactive 2D exercises, quizzes, animations, peer video, and fact sheets that target mediators of sexual risk-taking. Selected lesson activities are tailored on gender, self-reported sexual experience and intentions. IYG-Tech is housed on a secure server in the University of Texas School of Public Health, public access pending results of efficacy field testing.
IYG-Tech lessons progress through a logical content sequence including characteristics of healthy friendships, setting and protecting personal limits, puberty and reproduction, characteristics of healthy dating relationships, consequences of sex (HIV, STI, and pregnancy), refusal skills training, the importance of testing if a person is sexually active, and skills training in condom and contraceptive use (Figure 3 and Table 5). The curriculum can be monitored by teachers who use a content management system (CMS) to list students and monitor progress and quiz scores and pre-post data. No sensitive information (entered by students in temporary journals or in interactive tailored activities) is available to the teacher. In-house alpha testing of the new Internet-based activities and full IYG-Tech program were conducted to ensure it conformed to the intentions of the designers and function appropriately prior to feasibility pilot testing. This included local and distance (Internet) access to the program.
Figure 3.
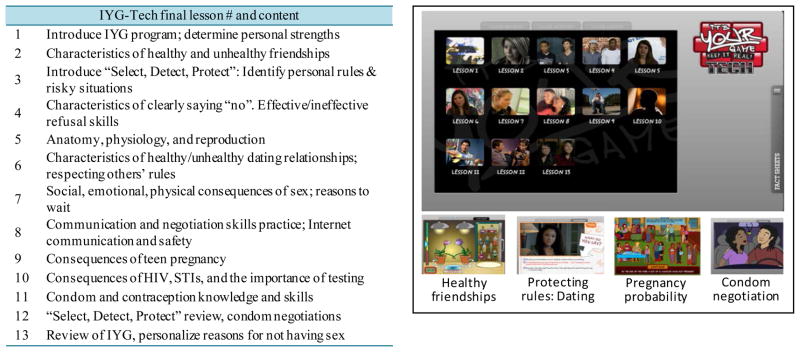
IYG-Tech final lesson content (tabled) and IYG-Tech screen captures illustrating lesson menu and selected new activities.
Table 5.
IYG -Tech final lesson learning objectives by outcome behaviors and mediators.
| Mediator | Learning objectives covered in IYG-Tech |
|---|---|
| 1. Students will not have sex | |
| Knowledge of… | Reproductive system (functional anatomy)/Types of sex (oral, anal, vaginal)/Consequences of sex (physical, emotional, social)/“Personal limits or rules”/Situations (places, peers, times) & signs (loss of “control”, pressure, feelings) that may make it hard to say no to sex;/Characteristics of clear refusal skills/Abstinence as being the only 100% effective way of avoiding HIV, STD, or getting pregnant./Pressures/influences (social, peer, partner, media) to have and not have sex/Communicating your rules to friends &/or partner & reasons why this is important/Alternate activities (e.g. movies, pizza, meet friends) and ways to suggest these/Avoidance strategies/Signs as cues to use refusal strategies/Personal rules regarding sex & intimate behaviors. |
| Skills and self-efficacy to… | Decide to not have sex/Identify signs & situations that may make it hard to say no to sex (e.g., peer pressure, social situations, when you really like the person) & use refusal skills/Communicate your personal rules to friends &/or partner/Identify & listen to signs and situations that may make it hard to say no to sex & avoid those situations (e.g. physically avoid the situation; use refusal/negotiation skills)/Suggest an appropriate alternative activity to sex. |
| Outcome expectations that… | The decision to not have sex will reduce the risk of getting HIV, STDs or becoming pregnant/Communicating your personal intentions and limits will lead to a better relationship with your partner/Communicating personal rules & intentions will decrease risk of HIV/STD & pregnancy/A healthy relationship is not predicated on sexual activity/Avoiding a high risk situation, alternative activities, &/or use of appropriate refusal skills will lead to successful abstinence without jeopardizing interpersonal relationships & reduce the risk of getting HIV, STDs or becoming pregnant./Deciding to not have sex will lead to increased self-respect/Use of refusal skills will keep you from doing things you don’t want to do (non-sex related) without jeopardizing friendships. |
| Perceived norms that… | Teens communicate their personal limits to friends/Teens communicate their personal limits regarding sex to their partners/Most middle school students do not have sex/Most middle school students feel it is important to not have sex. |
| Normative beliefs that… | Significant others approve and respect your refusing to have sex/People may have different personal rules regarding different behaviors/Friends approve of you communicating your personal rules/Your partner approves of you communicating your limits/Others approve of you recommending alternate activities to sex/Significant others approve and respect you refusing to do things that you choose not to do (non-sex related behaviors)/Significant others approve and respect your decision to avoid situations that may make it hard to say no to sex/Most parents feel it is important to practice refusal strategies to not have sex. |
| Social support to… | Use alternate activities/Decide to not have sex/Establish and communicate your personal intentions and limits/Avoid and/or help identify signs of risky situations/Use refusal strategies to not have sex. |
| 2. Students Will Have Healthy Relationships With Their Friends, Girlfriends, or Boyfriends | |
| Knowledge of… | Characteristics of healthy & unhealthy relationships/Healthy & unhealthy ways you behave in a relationship/Pressures & influences (social, peer, media) to have and not have healthy relationships/Expectations about healthy relationships/Ways to communicate expectations about relationships to friends & partner/Relationships with friends & partners that are not healthy/Situations where you come in contact with friends or partners that are not healthy/Strategies to avoid friends or partners that are not healthy/Alternative activities to being in unhealthy relationships. |
| Skills and self-efficacy to… | Evaluate relationships/Recognizing signs of unhealthy relationships/Have healthy relationships/Listen to your friends’ or partner’s expectations in relationships/Avoid unhealthy relationships/Communicate expectations in relationships/Engage in alternative activities to being in unhealthy relationships. |
| Perceived norms that… | Most peers can have healthy relationships. |
| Social support to… | Set and communicate expectations for healthy relationships./Evaluate relationships/Decide to have a healthy relationship/Avoid unhealthy relationships. |
| For students who ARE sexually active OR considering having sex.
| |
|---|---|
| Mediator | Learning objectives covered in IYG-Tech |
| 3: Students will use condoms correctly and consistently when having sex. | |
| Knowledge of… | Reproductive system (functional anatomy)/HIV/STDs (Transmission & symptoms)/Consequences of not using a condom if you have sex/Condoms in reducing the risk of HIV, STDs, & pregnancy/Types of condoms and relative pros & cons/Condom evaluation, application, & safe removal/Pressures & influences (peer, media, social) for condom use & none use/Places to obtain or buy condoms/Reasons for, and importance of, communication of intentions to use a condom to a partner/Protected and unprotected sex/Legality of condom purchase/Ways to purchase, carry, & protect a condom/Communication about intentions & negotiation to use condoms/Personal rules about condom use/Reasons that condoms are important with regular as well as casual partners. |
| Skills and self-efficacy to… | Evaluate, apply, and safely remove a condom/Decide to use condoms/Buy or obtain a free condom/Carry a condom/Negotiating condom use: Communicate intentions to use condoms, hear partner’s intentions, negotiate condom use, agree on condom use or to not have sex/Apply a condom correctly/Use a condom with regular partners as well as with casual partners. |
| Outcome expectations that… | Deciding to use condoms & using them correctly reduces the risk of getting HIV, STIs, pregnancy/A-priori agreements about using condoms (or not having sex) will increase the chances that these occur/Condom negotiation increases condom use with sex/Communicating intentions to use condoms with sex increases their use/Using condoms every time you have sex (even with regular partners) reduces the risk of getting HIV, STD’s, & pregnancy/Carrying a condom increases the chances of using one when having sex. |
| Perceived norms that… | Most sexually active teens buy or obtain free condoms, carry condoms, feel it is important to carry condoms, communicate their intentions to use condoms with their partners, & choose to not have sex if a condom is not used/Most sexually active teens who decide to use condoms are more likely to use them & to successfully negotiate their use/Partners should be willing to use condoms/Teens use condoms with regular & casual partners and feel this is important. |
| Perceived barriers to… | Recognizing that the benefits of using condoms outweigh the risks and side effects of not using condoms/Buying or obtaining a free condom (e.g., money, transportation), carrying a condom, and using condoms consistently over time. |
| Social support to… | Buy or obtain a free condom/Support your decision to use condoms/Support your decision to carry a condom, negotiate the use of a condom, making an agreement to use condoms or not have sex, & use condoms consistently over time. |
| 4: Students will use birth control correctly and consistently when having sex. | |
| Knowledge of… | Birth control options & methods (including advantages and disadvantages)/Guidelines for effective and consistent use of chosen birth control (plan ahead, take every day)/Both partners being responsible for use of non-hormonal birth control when sexually active. |
| Outcome expectations that… | Making an informed choice about birth control will decrease risk of pregnancy/Effective use of birth control along with condoms decreases risk of pregnancy. |
| For students who ARE sexually active.
| |
|---|---|
| Mediator | Learning objectives covered in IYG-Tech |
| 5: Students will get tested and counseled for HIV, STDs, and Pregnancy | |
| Knowledge of… | Types of STDs & modes of transmission/Types of tests available (different procedures; home/clinic)/Time taken to get test results./Limitations of tests (e.g., timing premature to detect HIV, pregnancy; false negative/positive; no counseling with home tests)./Places to get testing & counseling (incl. business hours, phone numbers)/Healthcare needs addressed & appropriate provider/Making an appointment (time & date)/Obtaining results (e.g. phone, in person)/Way to contact partners you have had (e.g. phone #, address). |
| Skills and self-efficacy to… | Decide to get tested and rationale for decision./Make and keep an appointment/Obtain test results/Cope with results/Engage in conversation w/your healthcare provider & get healthcare/Notify partner(s)/Plan ahead (use reminders)/Maintain testing behavior. |
| Perceived susceptibility that… | Any sexually active teen can get HIV/STD or become pregnant/impregnate partner/Current absence of symptoms does not ensure that you are not infected or pregnant/If you continue to be sexually active, you need to maintain testing behavior/Teens have a certain prevalence of HIV/STD & pregnancy. |
| Perceived severity of… | Consequences of teen pregnancy, STDs, & HIV/Consequences of particular STDs if you don’t obtain healthcare follow up. |
| Perceived norms that… | It is normal, expected, and responsible for teens who have sex to get tested for HIV/STD and pregnancy/People who are sexually active maintain testing behavior over time./Individuals who have HIV/STD or who are pregnant obtain healthcare/It is an individual’s responsibility to make past & future partners aware of their status. |
| Perceived benefits of… | The importance of knowing your status (& overcoming barriers such as denial or not wanting to know)/That getting tested outweighs barriers/That knowing your status is beneficial for health & peace of mind of self & partner, can result in early treatment (if positive results), & helps to reduce progression of symptoms (HIV/STD) or to have a healthier baby (if pregnant)/That taking responsibility for health of self & partner by getting tested over time is helpful, worthwhile, useful, the mature thing to do./Feeling mature and responsible for keeping the appointment, getting the test results, and notifying partner(s). |
| Perceived barriers to… | Getting tested that include cost, access, confidentiality, type of test, stigma, and embarrassment/Develop mitigating strategies/List free or low-cost testing sites (cost)/Recognize that testing is not a one-time occurrence/List your available times for testing/Be aware of your schedule (don’t double book)/Notify past and future partners/Identify ways to overcome barriers. |
| Social support to… | Your decision to get tested/Helping you make appointment, keep the appointment, and accompany you to get the results/Accompanying you to get treatment/Help you cope with treatment/Help and support you to notify partners/Help and support continued testing behavior. |
2.4. PHASE 2: Feasibility Evaluation of IYG-Tech
A school-based pilot test of IYG-Tech was conducted to determine the feasibility of delivery in a typical school setting and its impact to inform readiness for further efficacy testing.
Study Design and Participants
A single group, pre-test post-test usability study of the IYG-Tech computer lessons was conducted at a Southeast Texas middle school with a convenience sample comprised of 7th and 8th grade students (n = 22), 13 – 15 years of age (14.4 ± .46 years), female (50%), and minority (91% Hispanic and 9% African American). Participation was voluntary; written parental permission and child assent were obtained. The study was approved by the University of Texas Institutional Review Board (HSC-SPH-09-0413).
Study Protocol
Students were recruited and participated in the usability testing during P.E or an elective class period at their school. Students tested the 13 IYG-Tech computer lessons over approximately a two week period (testing two lessons during a 90 minute class period each day). The students accessed the program in a classroom setting using laptop computers. Prior to accessing the program activities, students completed a demographic survey. Each student was then provided with a laptop computer containing the IYG-Tech lessons and head-phones and asked to complete each of the 35-minute Internet-based lessons individually. At the end of each lesson, each student completed a usability survey regarding that lesson. Lessons were observed by study personnel who logged problems (technical or content related) and provided assistance as required. Students received $50 for their participation. Students completed a demographic form, a usability survey for each lesson, and pre/post slider bar questions within the lessons.
Measurement and analysis
Usability parameters were as previously described for the lab-based usability study. Motivational appeal was also assessed on whether youth compared IYG-Tech favorably against their favorite computer game, other school lessons, and other computer-based school lessons, and other health lessons (less fun, as much fun, more fun). Perceived impact was assessed by asking youth if IYG-Tech would help them make healthy decisions on 29 parameters specific to the content of IYG-Tech including friendships, selecting and protecting personal rules, enabling better risk reduction communication and negotiation (clear no’s and alternative actions), increasing understanding of reproduction and the developing body, and lowering risk of pregnancy and STD’s using a 3-point Likert scale (“yes”, “no”, “don’t know”).
Psychosocial impact variables included perceived importance and self-efficacy in 6 sexual health domains including healthy dating relationships, protecting personal rules about sex, negotiating with others to protect your personal rules, consequence of pregnancy, consequence of getting HIV or STDs, protecting personal rules about sex. Importance and self-efficacy items were embedded in the IYG-Tech program as text questions accompanied by audio and provided immediately before and after each lesson. The response set was a 10-point Likert scale slider bar adapted from previously reported motivational enhancement methods (Velasquez et al., 2001). Youth were asked to rate how important each issue was (e.g. how important to you is PROTECTING your personal rules about sex, how important to you is avoiding getting HIV or sexually transmitted diseases?) on the scale ranging from “0” (not important at all) to 10 (extremely important). Youth were asked to rate their self-efficacy (e.g. How sure are you that you can PROTECT your personal rules about sex? How sure are you that you can negotiate with others to protect your personal rules?) on the scale ranging from “0” (not at all sure) to 10 (very sure). Data analysis is as previously described for usability testing.
Feasibility testing results
Usability
Usability ratings across all 13 IYG-Tech lessons indicated high agreement on likability for the entire program (91.8% – 100%) and for all individual activities (62.5% – 100%) (Table 6). Program components (graphic, audio, and transition features) were similarly highly rated (73.0% – 100%). Youth rated the program as easy to use (68.4% – 100%), of credible and correct content (80% – 100%), of acceptable duration (81.3% – 100%), and that the words were understandable (89.4% – 100%). However, youth also reported requiring assistance in using the program (up to 43% for a given lesson). IYG-Tech rated highly compared to other school lessons, health lessons, and school computer lessons (76.2% – 100%) but less so when compared to favorite computer games (36.9% – 81.2%). Youth indicated they would recommend IYG-Tech lessons to their class (72.2% – 94.7%) but provided lower agreement on playing lessons again (31.3% – 70%).
Table 6.
Participant usability ratings for 13-lesson IYG-Tech prototype Internet-based curriculum.
| Construct | Item | Feasibility results (range of rounded % agreement) |
|---|---|---|
| Likability (Like a little or a lot) | Entire program | 92 – 100 |
| Activities (n = 79 across all lessons) | 63 – 100 | |
| Pictures/colors | 84 – 100 | |
| Sounds | 80 – 100 | |
| Buttons | 83 – 100 | |
| Buildings and people | 88 – 100 | |
| Cartoons | 81 – 100 | |
| Videos | 73 – 100 | |
| Transitions | 88 – 100 | |
|
| ||
| Ease of use (kind of easy or very easy) | Entire program | 100 |
| Activities (n = 79 across all lessons) | 69 – 100 | |
| Directions | 94 – 100 | |
|
| ||
| Credibility | Information is right (correct) | 88 – 100 |
| Information is trustworthy | 80 – 100 | |
|
| ||
| Acceptability | Duration/Time-on-task was “just right” | 81 – 100 |
|
| ||
| Understandability | Understands words | 89 – 100 |
| Needs help | 0 – 44 | |
|
| ||
| Motivational Appeal | Would recommend to my class | 72 – 95 |
| Would play again | 31 – 70 | |
| As much or more fun as my favorite computer game | 37 – 81 | |
| As much or more fun as other school lessons | 77 – 100 | |
| As much or more fun as other school computer lessons | 78 – 100 | |
| As much or more fun as other health lessons | 88 – 100 | |
|
| ||
| Perceived Impact | Helps make healthy choices | 89 – 100 |
Perceived impact
Youth rated the lessons as being helpful in preparing them in a range of sexual health behaviors to reduce the risk of pregnancy and STD’s including making healthy choices, selecting personal rules, detecting challenges, protecting personal rules through negotiation, using clear “no’s” and alternative actions of avoidance and refusal (89.5% – 100%) (Table 7). Psychosocial determinants: As a result of lesson exposure students increased their perceived importance of, and confidence in, negotiating with others to protect their personal rules (p < .05) and significantly increased knowledge about what constitutes a healthy relationship (p < .05) (Table 8).
Table 7.
IYG curriculum content by lesson and percent agreement on perceived impact.
| Lesson # and content | The information provided in this lesson will help me… | n (%)*
|
||
|---|---|---|---|---|
| n | % | |||
| 1 | Introduction, determine personal strengths. | make healthy choices | 15 | 93.8 |
|
| ||||
| 2 | Characteristics of healthy and unhealthy relationships. | know how to tell real friends | 10 | 100.0 |
| be a real friend | 10 | 100.0 | ||
| 3 | Introduce “Select, Detect, Protect”: Identify personal rules & risky situations. | select personal rules regarding healthy friendship | 17 | 89.5 |
| detect challenges to my personal rules | 18 | 94.7 | ||
| protect my personal rules | 18 | 94.7 | ||
|
| ||||
| 4 | Characteristics of clearly saying “no”. Effective/ineffective refusal skills. | use clear “no’s” | 18 | 100.0 |
| use alternate actions | 10 | 100.0 | ||
| avoid/refuse | 17 | 100.0 | ||
|
| ||||
| 5 | Anatomy, physiology, and reproduction. | know how my body develops | 19 | 95.0 |
| know how reproduction works | 19 | 95.0 | ||
| know what sex is | 20 | 100.0 | ||
| know the consequences of sex | 19 | 95.0 | ||
|
| ||||
| 6 | Characteristics of healthy and unhealthy dating relationships; respecting others rules. | have healthy relations | 18 | 100.0 |
| play by my “rules” | 18 | 100.0 | ||
|
| ||||
| 7 | Social, emotional, physical consequences of sex; reasons to wait. | protect my “rules” | 14 | 100.0 |
|
| ||||
| 8 | Communication & negotiation skills practice; Internet communication & safety. | to negotiate to protect my rules | 19 | 100.0 |
|
| ||||
| 9 | Consequences of teen pregnancy. | reduce pregnancy risk | 18 | 100.0 |
| make responsible decisions | 18 | 100.0 | ||
|
| ||||
| 10 | Consequences of STI/HIV & the importance of testing. | make responsible decisions | 21 | 100.0 |
| reduce STD risks | 20 | 95.2 | ||
|
| ||||
| 11 | Condom and contraception knowledge and skills. | make responsible decisions | 18 | 100.0 |
| reduce pregnancy & STD risk | 18 | 100.0 | ||
|
| ||||
| 12 | “Select, Detect, Protect” review; condom negotiations. | select my personal rules | 18 | 100.0 |
| detect challenges to my personal rules | 18 | 100.0 | ||
| protect my personal rules | 18 | 100.0 | ||
| to negotiate to protect my rules | 16 | 94.1 | ||
|
| ||||
| 13 | Review of IYG; personalize reasons for not having sex. | make safe choices | 20 | 100.0 |
| remember | 20 | 100.0 | ||
Note:
Remainder responses were “don’t know”.
Table 8.
Immediate within-lesson psychosocial impact (importance of topic and self-efficacy) by content domain1–3.
| Psychosocial variables | n | Pre-test Mean (SD) |
Post-test Mean (SD) |
Change Mean (SD) |
t | p | Delta Signed Rank | Sign Rank p |
|---|---|---|---|---|---|---|---|---|
| Healthy Dating Relationships (Lesson 6) | ||||||||
| How sure are you that you know what makes a healthy dating relationship? | 19 | 7.79 (2.52) | 9.81 (.77) | 2.01 (2.31) | 3.80 | .0013 | 39 | .0005 |
| How important to you is understanding what makes a healthy dating relationship? | 19 | 9.23 (1.34) | 9.82 (.54) | .53 (1.23) | 1.86 | .0753 | 18.5 | .0234 |
| Protecting personal rules about sex (Lesson 7) | ||||||||
| How sure are you that you can PROTECT your personal rules about sex? | 13 | 7.95 (3.56) | 9.53 (.89) | 1.58 (3.01) | 1.90 | .082 | 7.5 | .1563 |
| How important to you is PROTECTING your personal rules about sex? | 13 | 8.75 (2.97) | 9.31 (1.86) | .56 (1.79) | 1.13 | .2806 | 4.5 | .4375 |
| Negotiating with others to protect your personal rules (Lesson 8) | ||||||||
| How sure are you that you can negotiate with others to protect your personal rules? | 16 | 8.34 (1.92) | 9.94 (.25) | 1.59 (1.82) | 3.52 | .0039** | 22.5 | .0039 |
| How important to you is negotiating with others to protect your personal rules? | 16 | 8.72 (1.98) | 10.00 (.00) | 1.28 (1.98) | 2.58 | .0210 | 14 | .0156 |
| Consequence of pregnancy (Lesson 9) | ||||||||
| How sure are you that you understand the consequences of pregnancy? | 11 | 8.98 (3.00) | 9.88 (.33) | .89 (3.06) | .97 | .3558 | 2 | .6250 |
| How important to you is avoiding the consequences of pregnancy? | 11 | 9.65 (1.15) | 9.53 (1.50) | −.119 (1.96) | −.20 | .8444 | −.5 | 1.0000 |
| Consequence of getting HIV or STDs (Lesson 10) | ||||||||
| How sure are you that you understand the consequences of getting HIV or sexually transmitted diseases? | 9 | 8.78 (1.72) | 10.00 (.00) | 1.22 (1.72) | 2.12 | .0668 | 5 | .1250 |
| How important to you is avoiding getting HIV or sexually transmitted diseases? | 9 | 8.62 (2.17) | 10.00 (.00) | 1.38 (2.16) | 1.92 | .0915 | 5 | .1250 |
| Protecting personal rules about sex (Lesson 12) | ||||||||
| How sure are you that you can PROTECT your personal rules about sex? | 19 | 9.39 (1.77) | 9.99 (.03) | .61 (1.77) | 1.49 | .1547 | 8.5 | .0938 |
| How important to you is PROTECTING your personal rules about sex? | 19 | 9.79 (.44) | 9.47 (1.57) | −.32 (1.50) | −.93 | .3623 | −1.5 | .8125 |
Note:
All scales positively coded except likelihood to have oral and vaginal sex.
Sample is restricted to subjects with valid responses for both pre- and post-sliders for a given item.
Sample size was 1 or 2 for the following items: know what makes a good friend? (lesson 1), having good friendships to you? (lesson 2), that you have personals rule to live by? (lesson 3), that you can PROTECT your personal rules? (lesson 4), that you understand how reproduction works? (lesson 5), that you can reduce your risk of pregnancy or getting HIV and other sexually transmitted diseases? (lesson 11).
3. Discussion
After a program has been shown to be effective, a logical next step is its dissemination. Failure in dissemination, however, limits effective programs from reaching their full public health potential. Until recently, minimal progress had been made in the widespread dissemination of effective HIV, STI, and pregnancy prevention programs to youth, especially those targeted to middle schoolers (Kirby, 2007; Morrison, 2007; Lesesne et al., 2008; Rolleri, et al., 2008; Ingram et al., 2008; Noar et al., 2009). More recent initiatives are changing this landscape. These include the Office of Adolescent Health demonstration projects for the dissemination of evidence-based sexual health curricula (USDHHS, 2010) and the Administration for Children and Families (ACF) Family and Youth Services Bureau (FYSB) Care Act Personal Responsibility Education Program (PREP) funded trials (USDHHS, 2014). These initiatives are exploring the factors that facilitate successful implementation of evidence-based sexual health curriculum and the barriers that may prevent it.
IYG-Tech is an innovative contribution to sexual health education in that it is a completely online interactive curriculum, adapted from the effective IYG program. As an online curriculum, it is designed to mitigate conventional dissemination challenges of classroom-based curricula that can occur at the program, individual, and organizational level. While an Internet-based solution does not eradicate program level barriers, it does greatly optimize a facilitator’s ability to locate and acquire the program. Implementation of computer-based lessons can also vastly simplify facilitation, provided that school computer specifications meet broadband and connectivity requirements for the program.
Continued and repeated trainings and technical assistance have been the conventional method to overcome cited individual level barriers to classroom-based program implementation. These methods are designed to raise awareness, and reduce confusion about education policies (Levesque, 2000; Peskin 2011), increase skills and self-efficacy for teaching and adapting programs with fidelity, and reduce negative attitudes towards “science-based” approaches (Rolleri et al., 2008; Buston, 2002). To date, however, training has had limited effects on HIV program dissemination with adult populations (Rebchook et al., 2006; Harshbarger et al., 2006), requiring ongoing funding (Rolleri, et al., 2008; Philliber et al., 2008) and teacher willingness to attend trainings outside the school day (Basen-Engquist et al., 1994; Brink et al., 1991). A recent implementation trial of IYG in South Carolina, for example, reported 98.4% curriculum adherence and high quality implementation of the curriculum. However, this required an intensive technical assistance and training protocol with adequate funds to support these activities (Kershner et al., 2014). IYG-Tech is designed to provide high fidelity through a stand-alone curriculum requiring minimal-to-no facilitation. This delivery method may eliminate the barriers of teacher training and program fidelity. An Internet-based curriculum can provide confidential lesson content to students that are tailored on their sexual experience and intentions while reducing discomfort for facilitators who are not required to directly deliver what may be perceived as sensitive material.
An Internet-based delivery appears intuitively appealing as a channel to lower overhead and reduce costs (for purchasing, training, and implementing programs) to consumer school districts (Kirby, 2007; Landry et al., 2003; Noar et al., 2009; Rolleri et al., 2008) while also being a salient channel for “millennial” learners and timely channel given trends toward the adoption of technology by school districts in pursuit of great cost-effectiveness (National Center for Education Statistics, 2008). The upsurge of Internet connectivity in U.S. schools provides a natural substrate for the emergence of an eHealth curriculum like IYG-Tech. The adaptation of existing evidence-based programs (guided by well-established adaption frameworks) for access through interactive communication technology platforms (Card et al., 2011b; Wingood & DiClemente, 2008) provides precedent and guidance for developers to pursue this dissemination avenue without having to develop totally new programs.
The adaptation of IYG to IYG-Tech had a number of advantages including the strength of evidence of the original blended curriculum, the availability of the IYG creators in the adaptation process, and the existence of 8 original computer-based lessons and associated assets. Despite this, there were challenges in the creation of a digital version of the IYG curriculum that included ensuring that original learning objectives were fully represented, that a new Internet-based functionality of the original computer-based lessons could be achieved, and that the newly developed “proof-of-concept” lessons and prototype curriculum were acceptable to end users, feasible for delivery in the middle school setting, and impactful of mediators of sexual behavior.
The significant impact demonstrated in the evaluation of the Internet-adapted lessons included increased student perceptions of their friends having more positive beliefs about waiting to have sex, greater reasons for not having sex, greater self-efficacy for using condoms, and greater intentions to abstain from sex until marriage. These findings were also among the findings reported in the previous IYG field trials (Tortolero, 2010; Markham, 2012). Assessment of IYG-Tech impact was necessarily restricted to assessment of immediate pre-post change in psychosocial variables, but these results on psychosocial impact are encouraging, particularly considering the concatenated exposure to IYG-Tech necessitated in this study.
Advantages of the IYG-Tech learning experience include a one-to-one student-instructor (computer) ratio and a triangulation of strategies to target behavioral determinants including numerous examples of modeling of skilled behavior (e.g., saying no to having unprotected sex) and situational behaviors (e.g., making a choice to avoid high-risk situations and seeing the results of the choice) that influence normative perceptions as well as skills; confidential and personalized management of sensitive and potentially embarrassing issues; and individualized (tailored) intervention messages to specific characteristics of the users such as gender and sexual experience. Research studies have reported the potential of technology to impact sexual health knowledge (regarding decision-making, assertiveness, and communication), attitudes (regarding communication), self-efficacy, intentions, and self-reported behavior (Kann, 1987; Thomas et al., 1997; Lightfoot et al., 2007; Roberto et al., 2007; Kiene et al., 2006; Di et al., 2004). In a 3-arm evaluation (computer-based, small group, and control) of programs for delinquent youths in the juvenile justice system, Lightfoot and colleagues (2007) reported that the computer-based intervention was significantly more effective, at 3-month follow-up, in lowering frequency of sexual intercourse and that both conditions (computer-based and small group) significantly reduced the number of sex partners than the control condition. In an evaluation of 6 computer-based activities in 9 rural high schools, Roberto and colleagues (2008) found significant effects on knowledge about pregnancy and STIs, condom self-efficacy, attitudes toward waiting to have sex, and perceived susceptibility to HIV compared to controls. Such findings have prompted calls for the continued development, testing, and ultimate dissemination of digital (computer-based and social media) interventions to push the research agenda forward (Noar, 2009; Allison et al., 2012).
Positive ratings across usability parameters and perceived benefits of IYG-Tech to sexual health were commensurate with those of usability testing of the original IYG computer-based lessons (Shegog et al., 2007). The positive effect on attitudes to using computers in the classroom and the positive acceptability of IYG-Tech are likely related, at least in part, to the purposeful use of game strategies that have been successful in enhancing knowledge, self-efficacy, attitudes, and behaviors in varied education and health domains. The IYG computer lessons, purposefully designed to be immersive and motivational, include multiple gaming and edutainment elements in support of current initiatives for the development and formal research of socially conscious games for health (Health Games Research, 2013), and extend a growing body of evidence indicating the efficacy of computer-based applications in impacting health behavior change in youth (Papastergiou, 2009; Primack et al., 2012; Hieftje et al., 2013) and, more specifically, the early research on games for pregnancy prevention (“The Baby Game!” and “Romance!”) shown to enhance motivational appeal, knowledge, and intentions (Paperny & Starn, 1989).
While encouraging, the results reported here need to be interpreted in the context of study limitations that include artificially abbreviated exposure to the 8 Internet-adapted IYG computer-based lessons (lab-based “proof-of-concept” usability test) or the full IYG-Tech curriculum (school-based feasibility test) with immediate post-test; the single-group pre-test/post-test study design without a control group to mitigate threats to internal validity; the purposive sampling of participants; and the potential of demand characteristics to influence youth responses and feedback. Pilot feasibility studies of the type reported here are necessarily limited and designed to provide a measure of confidence that broader field trials are warranted and to highlight “red flags” (ranging from program bugs to deleterious usability or psychosocial impact) that suggest field testing is premature. Further, while most schools have internet connectivity, they vary in the number of available computers, Internet reliability, and bandwidth. The study described here cannot adequately address these challenges which may become apparent in broader efficacy trials. Of course, the digital approach to sexual health may provide an insufficient solution to organizational barriers. These barriers include the concern of school officials about negative community reactions and perceived controversy of sex education (Landry et al., 2000), a perceived lack of support from outside stakeholders (e.g. parents) for teaching this topic (Rolleri, et al., 2008; Paulussen et al., 1994; Buston et al., 2002) and pressure to devote class time to academic priorities rather than health topics. It is important to note that a successful implementation (whether it is Internet or conventional classroom lessons, or a blended approach) needs to address such organizational barriers to be successful. IYG-Tech is being evaluated in a randomized controlled trial in a large urban school district. Research results will be important to demonstrate the relative efficacy of this innovative technology-based curriculum compared with usual care, as well as to determine the cost-effectiveness implications of this implementation and dissemination strategy.
4. Conclusion
The development and testing of IYG-Tech reported here have demonstrated the usability and appeal of this curriculum among middle school students, suggesting that it may be a feasible delivery channel. Features of this approach include adherence to a rigorous, stepped adaptation protocol with adaptation steps informed by iterative prototype testing (usability, feasibility, impact), providing empirical evidence to inform each subsequent development step. This work provides a guide for future work on adaptation of evidence-based programs onto a communication technology platform.
Acknowledgments
This study was made possible through a grant from the City of Houston Department of Health and Human Services: HIV/STD Prevention Services—Category 5, School-Based Prevention Programs (Award Number: B10-021-5) and National Institutes of Mental Health grant #3R01MH085594-03S1.
References
- Allison S, Bauermeister JA, Bull S, Lightfoot M, Mustanski B, Shegog R, Levine D. The Intersection of Youth, Technology, and New Media with Sexual Health: Moving the Research Agenda Forward. The Journal of Adolescent Health. 2012;51:207–212. doi: 10.1016/j.jadohealth.2012.06.012. http://dx.doi.org/10.1016/j.jadohealth.2012.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Askar P, Yavuz H, Köksal M. Students’ Perceptions of Computer-Assisted Instruction Environment and Their Attitudes towards Computer-Assisted Learning. Educational Research. 1992;34:133–139. http://dx.doi.org/10.1080/0013188920340204. [Google Scholar]
- Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall; 1985. [Google Scholar]
- Bartholomew LK, Parcel GS, Kok G, Gottlieb N. Planning Health Promotion Programs: An Intervention Mapping Approach. 2. San Francisco: Jossey-Bass; 2006. [Google Scholar]
- Basen-Engquist K, O’Hara-Tompkins N, Lovato CY, Lewis MJ, Parcel GS, Gingiss P. The Effect of Two Types of Teacher Training on Implementation of Smart Choices: A Tobacco Prevention Curriculum. Journal of School Health. 1994;64:334–339. doi: 10.1111/j.1746-1561.1994.tb03323.x. http://dx.doi.org/10.1111/j.1746-1561.1994.tb03323.x. [DOI] [PubMed] [Google Scholar]
- Basen-Engquist K, Mâsse LC, Coyle K, Kirby D, Parcel GS, Banspach S, Nodora J. Validity of Scales Measuring the Psychosocial Determinants of HIV/STD-Related Risk Behavior in Adolescents. Health Education Research. 1999;14:25–38. doi: 10.1093/her/14.1.25. http://dx.doi.org/10.1093/her/14.1.25. [DOI] [PubMed] [Google Scholar]
- Borawski EA, Trapl ES, Lovegreen LD, Colabianchi N, Block T. Effectiveness of Abstinence-Only Intervention in Middle School Teens. American Journal of Health Behavior. 2005;29:423–434. doi: 10.5555/ajhb.2005.29.5.423. http://dx.doi.org/10.5993/AJHB.29.5.5. [DOI] [PubMed] [Google Scholar]
- Brink SG, Levenson-Gingiss P, Gottlieb NH. An Evaluation of the Effectiveness of a Planned Diffusion Process: The Smoke-Free Class of 2000 Project in Texas. Health Education Research. 1991;6:353–362. doi: 10.1093/her/6.3.353. http://dx.doi.org/10.1093/her/6.3.353. [DOI] [PubMed] [Google Scholar]
- Buston K, Wight D, Hart G, Scott S. Implementation of a Teacher-Delivered Sex Education Programme: Obstacles and Facilitating Factors. Health Education Research. 2002;17:59–72. doi: 10.1093/her/17.1.59. http://dx.doi.org/10.1093/her/17.1.59. [DOI] [PubMed] [Google Scholar]
- Card JJ, Kuhn T, Solomon J, Benner TA, Wingood GM, DiClemente RJ. Translating an Effective Group-Based HIV Prevention Program to a Program Delivered Primarily by Computer: Methods and Outcomes. AIDS Education and Prevention. 2011a;23:159–174. doi: 10.1521/aeap.2011.23.2.159. http://dx.doi.org/10.1521/aeap.2011.23.2.159. [DOI] [PubMed] [Google Scholar]
- Card JJ, Solomon J, Cunningham D. How to Adapt Effective Programs for Use in New Contexts. Health Promotion Practice. 2011b;12:25–35. doi: 10.1177/1524839909348592. http://dx.doi.org/10.1177/1524839909348592. [DOI] [PubMed] [Google Scholar]
- Coyle KK, Kirby DB, Marín BV, Gómez CA, Gregorich SE. Draw the Line/Respect the Line: A Randomized Trial of a Middle School Intervention to Reduce Sexual Risk Behaviors. American Journal of Public Health. 2004;94:843–851. doi: 10.2105/ajph.94.5.843. http://dx.doi.org/10.2105/AJPH.94.5.843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darroch JE, Landry DJ, Singh S. Changing Emphases in Sexuality Education in U.S. Public Secondary Schools, 1988–1999. Family Planning Perspectives. 2000;32:204–211. 265. http://dx.doi.org/10.2307/2648173. [PubMed] [Google Scholar]
- Di NJ, Schinke SP, Pena JB, Schwinn TM. Evaluation of a Brief Computer-Mediated Intervention to Reduce HIV Risk among Early Adolescent Females. Journal of Adolescent Health. 2004;35:62–64. doi: 10.1016/j.jadohealth.2003.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flay BR, Petratis J. The Theory of Triadic Influence: A New Theory of Health Behavior with Implications for Preventive Interventions. In: Albrecht GS, editor. Advances in Medical Sociology, A Reconsideration of Models of Behavior Change. IV. Greenwich, CT: JAI Press; 1994. pp. 19–44. [Google Scholar]
- Forhan SE, Gottlieb SL, Sternberg MR, Xu F, Datta SD, McQuillan GM, Berman SM, Markowitz LE. Prevalence of Sexually Transmitted Infections among Female Adolescents Aged 14 to 19 in the United States. Pediatrics. 2009;124:1505–1512. doi: 10.1542/peds.2009-0674. http://dx.doi.org/10.1542/peds.2009-0674. [DOI] [PubMed] [Google Scholar]
- Harshbarger C, Simmons G, Coelho H, Sloop K, Collins C. An Empirical Assessment of Implementation, Adaptation, and Tailoring: The Evaluation of CDC’s National Diffusion of VOICES/VOCES. AIDS Education and Prevention. 2006;18:184–197. doi: 10.1521/aeap.2006.18.supp.184. http://dx.doi.org/10.1521/aeap.2006.18.supp.184. [DOI] [PubMed] [Google Scholar]
- Health Games Research. Health Games Research: Advancing Effectiveness of Interactive Games for Health. 2013 http://www.healthgamesresearch.org.
- Hieftje K, Edelman J, Camenga DR, Fiellin LE. Electronic Media-Based Health Interventions Promoting Behavior Change in Youth: A Systematic Review. JAMA Pediatrics. 2013;167:574–580. doi: 10.1001/jamapediatrics.2013.1095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ingram BL, Flannery D, Elkavich A, Rotheram-Borus MJ. Common Processes in Evidence-Based Adolescent HIV Prevention Programs. AIDS and Behavior. 2008;12:374–383. doi: 10.1007/s10461-008-9369-1. http://dx.doi.org/10.1007/s10461-008-9369-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kann L, Telljohann SK, Wooley SF. Health Education: Results from the School Health Policies and Programs Study 2006. Journal of School Health. 2007;77:408–434. doi: 10.1111/j.1746-1561.2007.00228.x. http://dx.doi.org/10.1111/j.1746-1561.2007.00228.x. [DOI] [PubMed] [Google Scholar]
- Kann LK. Effects of Computer-Assisted Instruction on Selected Interaction Skills Related to Responsible Sexuality. Journal of School Health. 1987;57:282–287. doi: 10.1111/j.1746-1561.1987.tb03203.x. [DOI] [PubMed] [Google Scholar]
- Kiene SM, Barta WD. A Brief Individualized Computer-Delivered Sexual Risk Reduction Intervention Increases HIV/AIDS Preventive Behavior. Journal of Adolescent Health. 2006;39:404–410. doi: 10.1016/j.jadohealth.2005.12.029. http://dx.doi.org/10.1016/j.jadohealth.2005.12.029. [DOI] [PubMed] [Google Scholar]
- Kirby D. The Impact of Schools and School Programs upon Adolescent Sexual Behavior. Journal of Sex Research. 2002;39:27–33. doi: 10.1080/00224490209552116. http://dx.doi.org/10.1080/00224490209552116. [DOI] [PubMed] [Google Scholar]
- Kirby D. Emerging Answers 2007: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted Diseases. Washington DC: National Campaign to Prevent Teen and Unplanned Pregnancy; 2007. [Google Scholar]
- Komro KA, Perry CL, Williams CL, Stigler MH, Farbakhsh K, Veblen-Mortenson S. How Did Project Northland Reduce Alcohol Use among Young Adolescents? Analysis of Mediating Variables. Health Education Research. 2001;16:59–70. doi: 10.1093/her/16.1.59. http://dx.doi.org/10.1093/her/16.1.59. [DOI] [PubMed] [Google Scholar]
- Landry DJ, Singh S, Darroch JE. Sexuality Education in Fifth and Sixth Grades in U.S. Public Schools, 1999. Family Planning Perspectives. 2000;32:212–219. http://dx.doi.org/10.2307/2648174. [PubMed] [Google Scholar]
- Lesesne CA, Lewis KM, White CP, Green DC, Duffy JL, Wandersman A. Promoting Science Based Approaches to Teen Pregnancy Prevention: Proactively Engaging the Three Systems of the Interactive Systems Framework. American Journal of Community Psychology. 2008;41:379–392. doi: 10.1007/s10464-008-9175-y. http://dx.doi.org/10.1007/s10464-008-9175-y. [DOI] [PubMed] [Google Scholar]
- Levesque RJR. Sexuality Education: What Adolescents’ Educational Rights Require. Psychology, Public Policy, and Law. 2000;6:953–988. http://dx.doi.org/10.1037/1076-8971.6.4.953. [Google Scholar]
- Lightfoot M, Comulada WS, Stover G. Computerized HIV Preventive Intervention for Adolescents: Indications of Efficacy. American Journal of Public Health. 2007;97:1027–1030. doi: 10.2105/AJPH.2005.072652. http://dx.doi.org/10.2105/AJPH.2005.072652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markham CM, Basen-Engquist K, Coyle KK, Addy RC, Parcel GS. Safer Choices, a School-Based HIV, STD, and Pregnancy Prevention Program for Adolescents: Process Evaluation Issues Related to Curriculum Implementation. In: Steckler A, Linnan L, editors. Process Evaluation for Public Health Interventions and Research. San Francisco, CA: Jossey-Bass; 2002. pp. 209–248. [Google Scholar]
- Markham CM, Tortolero SR, Peskin MF, Shegog R, Thiel M, Baumler ER, Addy RC, Escobar-Chaves SL, Reininger B, Robin L. Sexual Risk Avoidance and Sexual Risk Reduction Interventions for Middle School Youth: A Randomized Controlled Trial. Journal of Adolescent Health. 2012;50:279–288. doi: 10.1016/j.jadohealth.2011.07.010. http://dx.doi.org/10.1016/j.jadohealth.2011.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: Final Data for 2012. USDHHS National Vital Statistics Reports. 2013:62. [PubMed] [Google Scholar]
- Martinez G, Abma J, Copen C. Educating Teenagers about Sex in the United States. NCHS Data Brief, No 44. 2010:1–8. [PubMed] [Google Scholar]
- Morrison DM, Hoppe MJ, Wells EA, Beadnell BA, Wilsdon A, Higa D, Gillmore MR, Casey EA. Replicating a Teen HIV/STD Preventive Intervention in a Multicultural City. AIDS Education and Prevention. 2007;19:258–273. doi: 10.1521/aeap.2007.19.3.258. http://dx.doi.org/10.1521/aeap.2007.19.3.258. [DOI] [PubMed] [Google Scholar]
- National Center for Education Statistics. Digest of Education Statistics, 2007. Washington, DC: U.S. Department of Education; 2008. [Google Scholar]
- Nielsen J. Usability Engineering. San Diego, CA: Morgan Kaufmann; 1993. [Google Scholar]
- Noar SM, Black HG, Pierce LB. Efficacy of Computer Technology-Based HIV Prevention Interventions: A Meta-Analysis. AIDS. 2009;23:107–115. doi: 10.1097/QAD.0b013e32831c5500. http://dx.doi.org/10.1097/QAD.0b013e32831c5500. [DOI] [PubMed] [Google Scholar]
- Papastergiou M. Exploring the Potential of Computer and Video Games for Health and Physical Activity Education: A Literature Review. Computers & Education. 2009;53:603–622. http://dx.doi.org/10.1016/j.compedu.2009.04.001. [Google Scholar]
- Paperny DM, Starn JR. Adolescent Pregnancy Prevention by Health Education Computer Games: Computer-Assisted Instruction of Knowledge and Attitudes. Pediatrics. 1989;83:742–752. [PubMed] [Google Scholar]
- Paulussen T, Kok G, Schaalma H. Antecedents to Adoption of Classroom-Based AIDS Education in Secondary Schools. Health Education Research. 1994;9:485–496. http://dx.doi.org/10.1093/her/9.4.485. [Google Scholar]
- Perry CL. Creating Health Behavior Change: How to Develop Community-Wide Programs for Youth. Thousand Oaks, CA: Sage; 1999. [Google Scholar]
- Peskin MF, Hernandez BF, Johnson K, Addy RC, Markham CM, Shegog R, Tortolero SR. Sexual Health Education from the Perspective of School Staff: Implications for Adoption and Implementation of Effective Programs in Middle School. Journal of Applied Research on Children: Informing Policy for Children at Risk. 2011;2:Article 9. http://digitalcommons.library.tmc.edu/childrenatrisk/vol2/iss2/9. [Google Scholar]
- Philliber S, Nolte K. Implementation Science: Promoting Science-Based Approaches to Prevent Teen Pregnancy. Prevention Science. 2008;9:166–177. doi: 10.1007/s11121-008-0094-9. http://dx.doi.org/10.1007/s11121-008-0094-9. [DOI] [PubMed] [Google Scholar]
- Primack BA, Carroll MV, McNamara M, Klem ML, King B, Rich M, Chan CW, Nayak S. Role of Video Games in Improving Health-Related Outcomes. American Journal of Preventive Medicine. 2012;42:630–638. doi: 10.1016/j.amepre.2012.02.023. http://dx.doi.org/10.1016/j.amepre.2012.02.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rebchook GM, Kegeles SM, Huebner D TRIP Research Team. Translating Research into Practice: The Dissemination and Initial Implementation of an Evidence-Based HIV Prevention Program. AIDS Education and Prevention. 2006;18:119–136. doi: 10.1521/aeap.2006.18.supp.119. http://dx.doi.org/10.1521/aeap.2006.18.supp.119. [DOI] [PubMed] [Google Scholar]
- Roberto A, Zimmerman RS, Carlyle K, Abner E, Cupp P, Hansen GL. The Effects of a Computer-Based HIV, STD, and Pregnancy Prevention Intervention: A Nine-School Trial. Health Communication. 2007;21:115–124. doi: 10.1080/10410230701306990. http://dx.doi.org/10.1080/10410230701306990. [DOI] [PubMed] [Google Scholar]
- Rolleri LA, Wilson MM, Paluzzi PA, Sedivy VJ. Building Capacity of State Adolescent Pregnancy Prevention Coalitions to Implement Science-Based Approaches. American Journal of Community Psychology. 2008;41:225–234. doi: 10.1007/s10464-008-9177-9. http://dx.doi.org/10.1007/s10464-008-9177-9. [DOI] [PubMed] [Google Scholar]
- Schaalma HP, Abraham C, Gillmore MR, Kok G. Sex Education as Health Promotion: What Does It Take? Archives of Sexual Behavior. 2004;33:259–269. doi: 10.1023/B:ASEB.0000026625.65171.1d. http://dx.doi.org/10.1023/B:ASEB.0000026625.65171.1d. [DOI] [PubMed] [Google Scholar]
- Shegog R, Markham C, Peskin M, Dancel M, Coton C, Tortolero S. “It’s Your Game”: An Innovative Multimedia Virtual World to Prevent HIV/STI and Pregnancy in Middle School Youth. Studies in Health Technology and Informatics. 2007;129:983–987. [PubMed] [Google Scholar]
- Story M, Lytle LA, Birnbaum AS, Perry CL. Peer-Led, School-Based Nutrition Education for Young Adolescents: Feasibility and Process Evaluation of the TEENS Study. The Journal of School Health. 2002;72:121–127. doi: 10.1111/j.1746-1561.2002.tb06529.x. http://dx.doi.org/10.1111/j.1746-1561.2002.tb06529.x. [DOI] [PubMed] [Google Scholar]
- Thomas R, Cahill J, Santilli L. Using an Interactive Computer Game to Increase Skill and Self-Efficacy Regarding Safer Sex Negotiation: Field Test Results. Health Education and Behavior. 1997;24:54–70. doi: 10.1177/109019819702400108. http://dx.doi.org/10.1177/109019819702400108. [DOI] [PubMed] [Google Scholar]
- Tortolero SR, Markham CM, Peskin MF, Shegog R, Addy RC, Escobar-Chaves SL, Baumler ER. It’s Your Game: Keep It Real: Delaying Sexual Behavior with an Effective Middle School Program. Journal of Adolescent Health. 2010;46:169–179. doi: 10.1016/j.jadohealth.2009.06.008. http://dx.doi.org/10.1016/j.jadohealth.2009.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- USDHHS & ACF. PREP Grants. 2014 http://www.acf.hhs.gov/programs/fysb/resource/prep-fact-sheet.
- Velasquez MM, Gaddy-Maurer G, Crouch C, DiClemente CC. Group Treatment for Substance Abuse: A Stages-of-Change Therapy Manual. New York: The Guilford Press; 2001. [Google Scholar]
- Wikipedia. Proof of Concept. http://en.wikipedia.org/wiki/Proof_of_concept.
- Wikipedia. Software Design Document. http://en.wikipedia.org/wiki/Software_design_document.
- Wingood GM, DiClemente RJ. The ADAPT-ITT Model. A Novel Strategy of Adapting Evidence-Based HIV Interventions. Journal of Acquired Immune Deficiency Syndrome. 2008;47:S40–S46. doi: 10.1097/QAI.0b013e3181605df1. http://dx.doi.org/10.1097/QAI.0b013e3181605df1. [DOI] [PubMed] [Google Scholar]