

Highlights
-
•
Subacromial impingement syndrome is one of the most common disorders of shoulder.
-
•
Osteochondromas arising under the acromion rarely cause impingement syndrome.
-
•
The diagnosis of subacromial osteochondroma should be considered in any patient with shoulder impingement syndrome and good functional results can be expected following total excision.
Keywords: Osteochondroma, Shoulder impingement syndrome, Shoulder, Acromion, Scapula
Abstract
Introduction
Subacromial impingement syndrome is one of the most common disorders of shoulder. Scapula is a very rare site for osteochondromas, and osteochondromas arising under the acromion cause impingement syndrome.
Presentation of case
We presented 34-year old female patient with subacromial impingement syndrome secondary to osteochondroma. She had received conservative treatment several times in other clinics. The osteochondroma causing impingement was not diagnosed. Physical examination of the right shoulder revealed 90° flexion, 70° abduction, 20° external rotation and internal rotation to sacrum. X-ray, CT and MRI of the shoulder was obtained. Osteochondroma of the acromion (35 × 33 × 25 mm) causing impingement was detected. The osteochondroma of acromion compressed, displaced and ruptured the supraspinatus tendon. Also an osseous prominence of glenoid was detected during shoulder arthroscopy, and it was removed arthroscopically. The giant osteochondroma of acromion could not remove arthroscopically due to the size of the lesion, and it was removed totally through a mini open approach. Histopathological examination confirmed the diagnosis of osteochondroma.
Discussion
Scapular, clavicular and humeral osteochondromas cause impingement syndrome. Osteochondroma should be treated with total excision. Recurrences can be seen due to insufficient removal of osteochondromas. We think that, total excision is important to prevent recurrence. Subacromial osteochondroma is a very rare cause of impingement syndrome, and if it isn’t diagnosed early it limits shoulder movements, causes severe shoulder impingement and rotator cuff tear.
Conclusion
The diagnosis of subacromial osteochondroma should be considered in any patient with shoulder impingement syndrome and good functional results can be expected following total excision.
1. Introduction
Subacromial impingement syndrome is one of the most common disorders of shoulder [1]. It causes pain which is thought to be caused by encroachment of coracoacromial arch on the bursa and cuff [2,3]. Impingement may originate from acromion, coracoacromial ligament, acromioclavicular joint, biceps tendon or coracoid process [2,4]. On the other hand, osteochondromas are common benign bone tumors, but scapula is a very rare site [5]. Osteochondromas arising under the acromion rarely cause impingement syndrome [6,7].
In this report, we presented a neglected scapular acromial osteochondroma. The osteochondroma with a large mass causing shoulder impingement syndrome was located under the acromion.
2. Presentation of case
A 34 year-old woman admitted to our clinic because of pain and limitation of right shoulder movements for eighteen years. She was a housewife. The pain has been increasing during shoulder movements for several years. She had received conservative treatment several times in other clinics. There was no weight loss, fewer and night sweats. In family history, no bone tumor was detected.
No atrophy, swelling, tenderness and deformity were detected around the shoulder. Physical examination revealed 90° flexion, 70° abduction, 20° external rotation and internal rotation to sacrum. Mild supraspinatus weakness was observed and no sign of shoulder instability was seen. Neer and Hawking signs were positive.
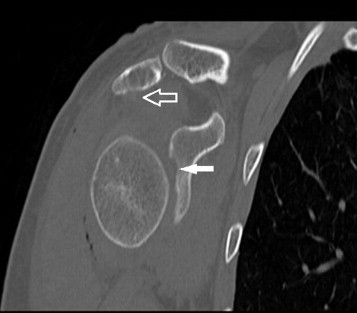
Plain radiography of the shoulder showed a bony prominence protruded inferiorly from the undersurface of the acromion. CT (computed tomography) images showed the osseous prominence under the acromion and a lesion on the the glenoid (Fig. 1). MRI (Magnetic resonance images) revealed the cartilage cap of the exostosis (35 × 33 × 25 mm) arising from the acromion. The osteochondroma compressed and displaced the supraspinatus tendon. The other lesion was seen on the superior part of the glenoid. The bone marrow of the osteochondroma was continuous with the bone marrow of the scapula (Fig. 2).
Fig. 1.

Preoperative coronal reformatted CT images show the lesion of the glenoid fossa (arrow) and the osteochondroma of the acromion (open arrow).
Fig. 2.

MR image shows the giant osteochondroma arising from the acromion (white arrow) and lesion of the glenoid (black arrow). Supraspinatus tendon (open arrow).
At surgery, arthroscopic examination of glenohumeral joint and subacromial space was planned first. During the glenohumeral joint examination, supraspinatus rupture and a small osseous prominence was detected on the anterosuperior part of the glenoid that was removed arthroscopically. The giant osteochondroma causing impingement syndrome was seen under the acromion. It was very big to remove arthroscopically, so it was removed totally through a mini open approach by using osteotome. Supraspinatus tendon was repaired and skin was closed in proper fashion (Fig. 3).
Fig. 3.
Postoperative coronal reformatted CT image shows the ostechondroma of the acromion (open arrow) and osseous prominence of glenoid (arrow) was removed totaly.
Histopathological examination confirmed the diagnosis of osteochondroma. It showed osteocartilagineous mass with hyaline cartilage on the laminar bone, no cellular atypia or malignant differentiation was observed. The histopathological examination of the osseous prominence of the glenoid showed osseous tissue covered with cartilage.
At first postoperative day, physiotherapy for shoulder and elbow joint was started. At the end of the third month, the patient gained full range of motion without pain and no recurrences was detected in control imaging studies.
3. Discussion
Osteochondroma is the most common benign bone tumor of scapula, although scapula accounts only 4.4 percent of all osteochondromas [8,9]. Scapular osteochondromas are painless, but mechanical effect of the tumor causes symptoms such as pseudo-winging, snapping and pain [5,10,11]. The pain of the osteochondroma can be originate from the mechanical irritation of the rotator cuff [12]. In our case, supraspinatus tendon was ruptured due to pressure of the giant osteochondroma on rotator cuff.
It has been reported that scapular, clavicular and humeral osteochondromas cause impingement syndrome [7,12,13]. Pimpalnerkar et al. reported dual osteochondroma of coronoid and glenoid causing double impingement [14]. Osteochondromas can be intraarticular or extraarticular [7,13]. Space occupying lesions cause subacromial impingement syndrome. In our case, scapular subacromial extraarticular osteocondroma was causing impingement syndrome.
Osteochondroma should be treated with total excision. Arthroscopic or endoscopically assisted excision of osteochondromas were reported previously [7,10]. Recurrences can be seen due to insufficient removal of osteochondromas, recurrence rate was over 2% [9]. Arthroscopic total excision of the tumor may not always be possible. Surgeon’s experience, localization and size of the lesion are important factors for appropriate excision with arthroscopy. In our case, osseous prominence of glenoid was removed arthroscopically, and acromial osteochondroma was excised through a mini open approach due to the size. We think that, total excision is important to prevent recurrence. In our case we totally excised the osteochondroma, so we don't expect recurrences.
Impingement due to space occupying lesion is a rare condition. We determined neglected subacromial osteochondroma causing impingement syndrome. Subacromial osteochondroma is a rare cause of impingement syndrome, and if it is not diagnosed early, it limits shoulder movements, causes severe impingement and rotator cuff tear.
4. Conclusion
The diagnosis of subacromial osteochondroma should be considered in any patient with shoulder impingement syndrome and good functional results can be expected following total excision.
Conflict of interests
There is no conflict of interest.
Funding
No funding for this study.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Atilla Çıtlak contributed study concept, data collection, writing the paper. Ulaş Akgün and Tugrul Bulut contributed data collection and data analysis. Cihan Aslan contributed study design. Berna Dirim Mete contributed data analysis and detailed radiological evaluation. Muhittin Şener contributed study design, data analysis, writing the paper.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Guarantor
Atilla Çıtlak is the corresponding author and gurantor.
Contributor Information
Atilla Çıtlak, Email: atillacitlak@yahoo.com.
Ulaş Akgün, Email: ulasakgun@gmail.com.
Tugrul Bulut, Email: drtugrulbulut@yahoo.com.
Cihan Aslan, Email: chnaslan@yahoo.com.
Berna Dirim Mete, Email: bernadirim@gmail.com.
Muhittin Şener, Email: msener@yahoo.com.
References
- 1.Balke M., Schmidt C., Dedy N., Banerjee M., Bouillon B., Liem D. Correlation of acromial morphology with impingement syndrome and rotator cuff tears. Acta Orthop. 2013;84(2):178–183. doi: 10.3109/17453674.2013.773413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lunsjö K., Bengtsson M., Nordqvist A., Abu-Zidan F.M. Patients with shoulder impingement remain satisfied 6 years after arthroscopic subacromial decompression: a prospective study of 46 patients. Arch. Orthop. Trauma Surg. 2009;129(5):679–683. doi: 10.3109/17453674.2011.623571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Min K.S., St Pierre P., Ryan P.M., Marchant B.G., Wilson C.J., Arrington E.D. A double-blind randomized controlled trial comparing the effects of subacromial injection with corticosteroid versus NSAID in patients with shoulder impingement syndrome. J. Shoulder Elbow Surg. 2013;22(5):595–601. doi: 10.1016/j.jse.2012.08.026. [DOI] [PubMed] [Google Scholar]
- 4.Relwani J., Ogufere W., Orakwe S. Subacromial lipoma causing impingement syndrome of the shoulder: a case report. J. Shoulder Elbow Surg. 2003;12(2):202–203. doi: 10.1067/mse.2003.45. [DOI] [PubMed] [Google Scholar]
- 5.Frost N.L., Parada S.A., Manoso M.W., Arrington E., Benfanti P. Scapular osteochondromas treated with surgical excision. Orthopedics. 2010;33(11):804. doi: 10.3928/01477447-20100924-09. [DOI] [PubMed] [Google Scholar]
- 6.Craig E.V. Subacromial impingement syndrome in hereditary multiple exostoses. Clin. Orthop. Relat. Res. 1986;209:182–184. [PubMed] [Google Scholar]
- 7.Lu M.T., Abboud J.A. Subacromial osteochondroma. Orthopedics. 2011;34(9):e581–e583. doi: 10.3928/01477447-20110714-19. [DOI] [PubMed] [Google Scholar]
- 8.Cleeman E., Auerbach J.D., Springfield D.S. Tumors of the shoulder girdle: a review of 194 cases. J. Shoulder Elbow Surg. 2005;14(5):460–465. doi: 10.1016/j.jse.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 9.Unni K.K. Osteochondroma. In: Unni K.K., editor. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. 5th ed. Lippincott–Raven; Philadelphia: 1996. pp. 11–23. [Google Scholar]
- 10.Kumar N., Ramakrishnan V., Johnson G.V., Southern S. Endoscopically-assisted excision of scapular osteochondroma. Acta Orthop. Scand. 1999;70(4):394–396. doi: 10.3109/17453679908997832. [DOI] [PubMed] [Google Scholar]
- 11.Tomo H., Ito Y., Aono M., Takaoka K. Chest wall deformity associated with osteochondroma of the scapula: a case report and review of the literature. J. Shoulder Elbow Surg. 2005;14(1):103–106. doi: 10.1016/j.jse.2004.03.007. [DOI] [PubMed] [Google Scholar]
- 12.Ogawa K., Yoshida A., Ui M. Symptomatic osteochondroma of the clavicle: a report of two cases. J. Bone Joint Surg. Am. 1999;81(3):404–408. doi: 10.2106/00004623-199903000-00014. [DOI] [PubMed] [Google Scholar]
- 13.Padua R., Castagna A., Ceccarelli E., Bondì R., Alviti F., Padua L. Intracapsular osteochondroma of the humeral head in an adult causing restriction of motion: a case report. J. Shoulder Elbow Surg. 2009;18(4):e30–e31. doi: 10.1016/j.jse.2008.09.008. [DOI] [PubMed] [Google Scholar]
- 14.Pimpalnerkar A., Anand A., Anand A., Thimmegowda A.H., Mehr A., Kanona H. Double impingement of the rotator cuff – an unusual presentation of dual osteochondromas. Eur. Orthop. Traumatol. 2013;4:169–171. [Google Scholar]