

Abstract
Objective:
We aimed to evaluate the association between comorbidity and rates of hospitalization in the multiple sclerosis (MS) population as compared to a matched cohort from the general population.
Methods:
Using population-based administrative data from the Canadian province of Manitoba, we identified 4,875 persons with MS and a matched general population cohort of 24,533 persons. We identified all acute care hospitalizations in the period 2007–2011. Using general linear models, we evaluated the association between comorbidity status and hospitalization rates (all-cause, non-MS-related, MS-related) in the 2 populations, adjusting for age, sex, and socioeconomic status.
Results:
Comorbidity was common in both cohorts. Over the 5-year study period, the MS population had a 1.5-fold higher hospitalization rate (adjusted rate ratio [aRR] 1.56; 95% confidence interval [CI] 1.44–1.68) than the matched population. Any comorbidity was associated with a 2-fold increased risk of non-MS-related hospitalization rates (aRR 2.21; 95% CI 1.73–2.82) in the MS population, but a nearly 4-fold increase in hospitalization rates in the matched population (aRR 3.85; 95% CI 3.40–4.35). Comorbidity was not associated with rates of hospitalization for MS-related reasons, regardless of how comorbidity status was defined.
Conclusions:
In the MS population, comorbidity is associated with an increased risk of all-cause hospitalizations, suggesting that the prevention and management of comorbidity may reduce hospitalizations.
Comorbidity is common in the multiple sclerosis (MS) population. Physical comorbidities, such as hypertension, affect more than one-third of persons with MS.1 Psychiatric comorbidities, such as depression, affect more than 50% of persons with MS over their lifetime.2 Comorbidity is associated with longer diagnostic delays and greater disability at diagnosis and lower quality of life in MS.3,4
The impact of comorbidity on health care utilization in MS is unknown, but is identified as a key knowledge gap for clinicians and decision-makers.5 Health care utilization is high in the MS population,6 with up to 25.8% of the MS population being hospitalized annually,7 exceeding the rate of hospitalizations in the general population.8 The mean number of physician visits per year is also higher in the MS population.9 In other diseases, persons with multiple chronic health conditions have higher rates of health care utilization than persons with a single condition.10
Hospitalizations constitute the largest component of resource use in Canada and other industrialized countries,11 and costs of hospitalizations for MS are rising.12 In other chronic diseases, comorbidity is often undertreated,13 potentially leading to increased hospitalizations. Therefore, we aimed to evaluate the association between comorbidity and rates of hospitalization in the MS population as compared to a matched cohort from the general population. We hypothesized that the presence of comorbidities increases the rates of hospitalization for MS-related and non-MS-related reasons.
METHODS
Data source.
We used administrative (health claims) data from Manitoba, a Canadian province with a population of approximately 1.2 million residents. Ninety-eight percent of the population receives health care coverage through Manitoba Health, thus records of health care utilization are available for nearly all services for all Manitobans.14,15 All health services claims include a unique personal health identification number (PHIN), which identifies the person to whom the service was delivered. Hospital discharge abstracts include the PHIN, admission and discharge dates, and up to 25 discharge diagnoses listed using ICD-10-CA codes. Before 2004, discharge diagnoses were recorded using 5-digit ICD-9 codes. The first discharge diagnosis is considered the primary reason for the hospitalization. Each physician claim includes the PHIN, service date, and 3-digit ICD-9-CM code for one physician-assigned diagnosis. The Drug Programs Information Network is a pharmaceutical database that captures all outpatient prescription drug dispensations. A population registry includes the PHIN, sex, date of birth, region of residence (postal code), dates of health coverage, and date of death for all residents. To protect confidentiality data, linkage was performed via scrambled PHIN, using anonymized versions of these databases.
Standard protocol approvals, registrations, and patient consents.
The University of Manitoba Health Research Ethics Board approved the study, and the Manitoba Health Information Privacy Committee approved administrative data access.
Study populations.
Identification of the study population and outcomes is detailed in appendix e-1 on the Neurology® Web site at Neurology.org. Briefly, we identified all Manitobans with MS from 1984 through 2011 using a validated case definition.16 Specifically, we defined persons with ≥3 hospital, physician, or prescription claims for MS or MS-specific medications as having MS. To identify controls from the remaining members of the general (not healthy) population, we excluded anyone with ≥1 ICD-9-CM/ICD-10-CA diagnostic codes for any demyelinating disease (see appendix e-1). This ensured that individuals with one demyelinating event who might ultimately meet the case definition for MS were not misclassified as controls and allowed a distinct comparison between the MS and general populations. We identified up to 5 controls for each MS case, matched on sex, exact year of birth, and region of residence (postal code). For each MS case, we assigned the date of diagnosis (index date) as the date of the first claim for demyelinating disease. The same date was assigned to their matched controls.
Outcome.
We focused on acute care hospitalizations because these constitute the biggest component of health resource use in industrialized countries.11,17 Using hospital claims, we identified inpatient hospitalizations after excluding admissions related to pregnancy, respite, or long-term care because the factors associated with those admissions may differ from the factors associated with admissions for acute illness. To minimize double-counting of hospitalizations related to transfers between facilities for continued care, overnight hospitalizations beginning within ±1 day of another hospital discharge with the same primary or secondary diagnosis codes were considered to be part of the same hospitalization.18
For the MS population, we classified hospitalizations as MS-related, possibly MS-related, and not MS-related as described previously (appendix e-1).19
Comorbidity.
We selected comorbidities for study based on our prior work indicating they were associated with other outcomes in MS or affected at least 5% of the MS population,3,4,20 or were important causes of hospitalization in the general population,21 and could be accurately identified using administrative case definitions.22–26 The comorbidities included hypertension, diabetes, hyperlipidemia, ischemic heart disease, chronic lung disease, fibromyalgia, autoimmune thyroid disease, migraine, depression, anxiety, and bipolar disorder. We applied validated administrative case definitions based on hospital, physician, and prescription claims for these comorbidities to the MS and matched populations.22–26
Analysis.
To identify possible excess hospital utilization in the MS population, we compared all-cause hospitalization rates between the MS and matched populations without adjusting for comorbidities using Poisson regression with generalized estimating equations with an exchangeable correlation to account for repeated hospitalizations by individuals. We included the log of person-years as an offset in the models. We restricted these analyses to the years 2007 through 2011 (the latest date available) (1) because hospitalization rates were more stable in both populations over this time period as compared to earlier years, when there were dramatic and differential declines in the rates19; (2) because of the difficulty in accurately identifying some comorbidities, such as autoimmune thyroid disease, before the availability of prescription claims27; and (3) to minimize the impact of temporal changes in the diagnosis and management of MS and comorbidity.
We then repeated our regression analyses with adjustment for comorbidity, using 3 outcomes: (1) all-cause hospitalizations in the MS and matched populations; (2) non-MS-related hospitalizations in the MS population to more closely match all-cause hospitalizations in the matched population; and (3) MS-related hospitalizations in the MS population. We used a staged approach beginning with any comorbidity, followed by a count of comorbidities, and then included individual comorbidities as indicated above. Covariates included sex (female as reference group); age at observation year categorized as <40 years (reference group), 40–60 years, and >60 years to ensure adequate cell sizes; and socioeconomic status (SES) in quintiles. We established SES by linking forward sortation area (first 3 digits of postal code) to Canadian census data to obtain the median household income, and then generated quintiles.28 We did not include a separate variable for region because forward sortation area was already being used to determine SES. Findings from the regression models are reported as adjusted rate ratios (aRRs) with 95% confidence intervals (CIs). Additional analyses included (1) additional adjustment for the annual number of physician visits; (2) restricting MS-related admissions to those identified solely by the primary discharge diagnosis; and (3) including admissions for long-term care and respite.
Analyses were conducted using SAS v9.3 (SAS Institute, Cary, NC).
RESULTS
During the study period, we observed 4,875 persons with MS and 24,533 controls. Seventy-one percent of both cohorts were female, and the cohorts were well-matched with respect to age at the index date (table 1). We focused on hospitalizations after the index date, excluding those related to long-term care, respite, and pregnancy, leaving 2,551 hospitalizations for analysis in the MS population and 8,531 in the matched population.
Table 1.
Characteristics of the study population (2007–2011)
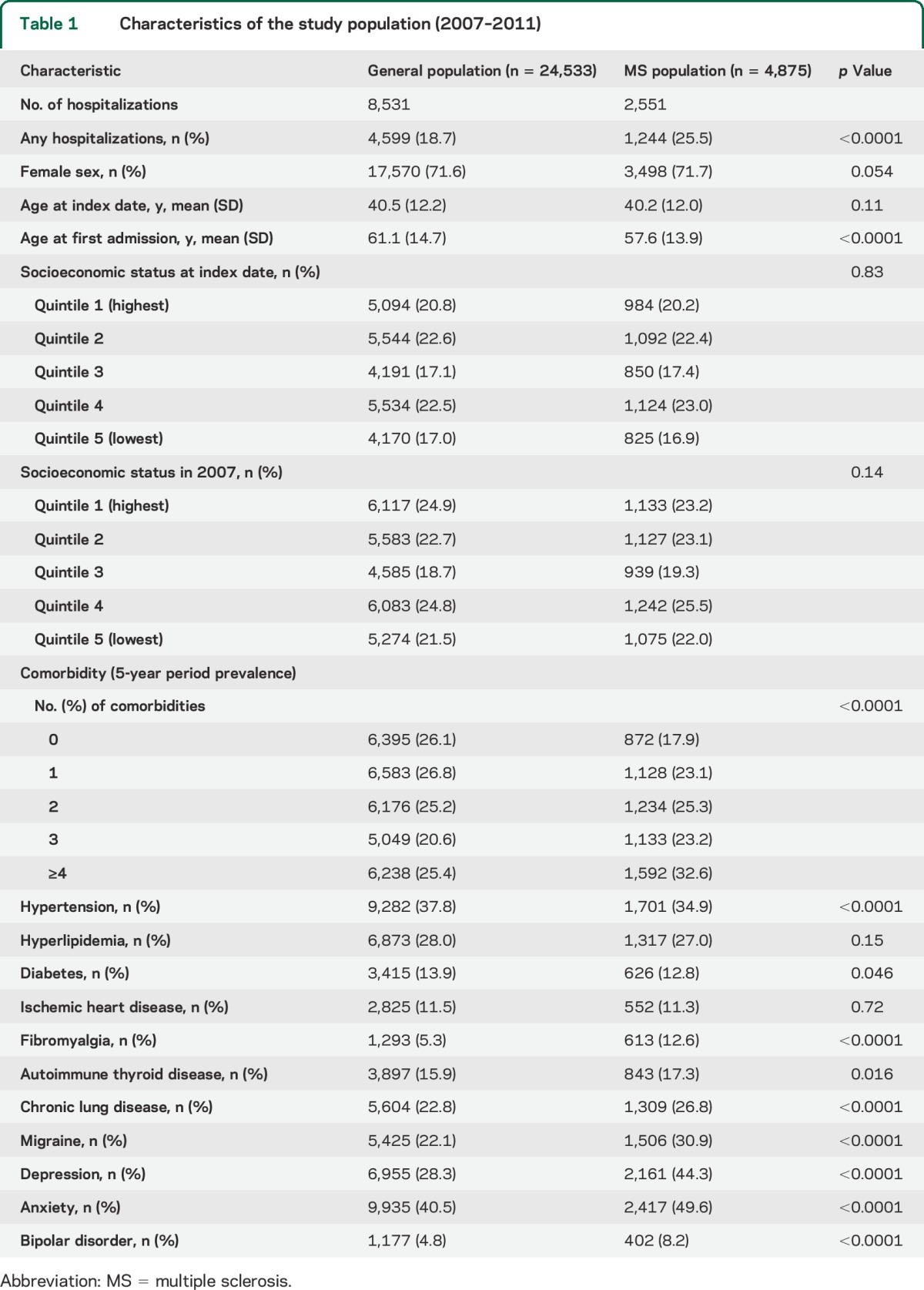
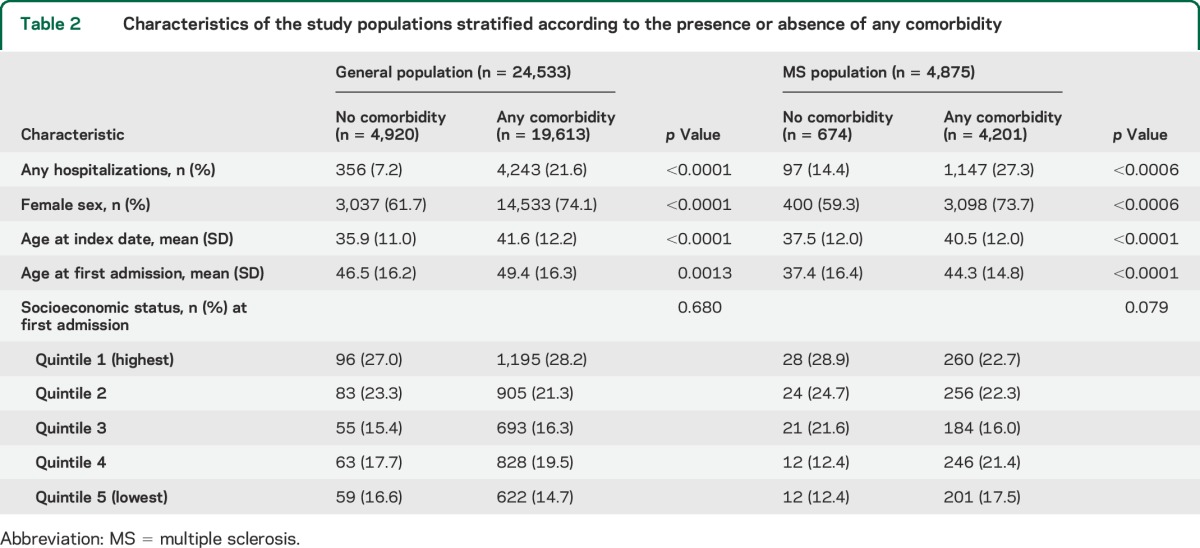
Comorbidity was common in both cohorts (table 1). Fibromyalgia, autoimmune thyroid disease, chronic lung disease, migraine, depression, anxiety, and bipolar disorder were all more common in the MS population than in the matched population. Individuals with any comorbidity were more likely to be female and older than those without comorbidity in both populations (table 2).
Table 2.
Characteristics of the study populations stratified according to the presence or absence of any comorbidity
Hospitalizations.
The proportion of the MS population who were hospitalized annually for any cause was 7.11% in 2007 and declined to 6.42% in 2011.19 The annual rate of hospitalizations also declined slightly from 9.67 (95% CI 9.66–9.68) per 100 person-years in 2007 to 8.58 (95% CI 8.57–8.59) in 2011 (p = 0.0028 for linear trend). From 2007 through 2011, 8.9% of hospitalizations were MS-related, 3.7% were possibly MS-related, and 87.4% were not MS-related.
The proportion of the matched population who were hospitalized was 4.73% in 2007 and remained similar at 4.53% in 2011. The annual rate of hospitalizations was 6.55 (95% CI 6.54–6.56) per 100 person-years in 2007 and 6.19 (95% CI 5.92–6.48) in 2011 (p = 0.56 for linear trend).
Over the 5-year study period, the MS population had a 1.5-fold higher hospitalization rate than the matched population (unadjusted rate ratio [RR] 1.52; 95% CI 1.41–1.65). On average, the MS population was 3.5 years younger at the time of their first hospital admission than the matched population.
Hospitalization rates were higher in men than women (figure 1) and with increasing age and SES (data not shown). After adjustment for age, sex, and SES, the MS population still had a 1.5-fold higher hospitalization rate than the general population (aRR 1.56; 95% CI 1.44–1.68).
Figure 1. Sex-stratified annual rate of hospitalizations in the multiple sclerosis (MS) and matched populations from 2007 to 2011.

Comorbidity and hospitalizations.
When we evaluated crude rates of all-cause hospitalizations, individuals with any comorbidity had higher hospitalization rates than those without any comorbidity in both populations (figure 2). In the MS population, individuals with any comorbidity had a nearly 3-fold increased rate of hospitalization (unadjusted RR 2.88; 95% CI 1.41–3.43). In the matched population, however, any comorbidity was associated with a nearly 6-fold increased rate of hospitalization (unadjusted RR 5.57; 95% CI 5.04–6.16). We also observed a dose-response relationship in which the hospitalization rates increased with an increasing number of comorbidities (data not shown).
Figure 2. Annual age-standardized hospitalization rates in the multiple sclerosis (MS) and matched populations by comorbidity status from 2007 to 2011.

Given the observed interaction between population (MS vs matched) and the associations of comorbidity with all-cause hospitalization rates (p < 0.0001), we stratified the multivariable analyses by population. After adjusting for sex, age, and SES, any comorbidity was associated with increased all-cause hospitalization rates in both populations but the magnitude of the effect differed. Any comorbidity was associated with a 2-fold increased risk of all-cause hospitalizations (aRR 2.21; 95% CI 1.73–2.82, table e-1) in the MS population vs a nearly 4-fold increased risk in the matched population (aRR 3.85; 95% CI 3.40–4.35).
To better compare the association of comorbidity with hospitalizations in the MS population and the matched population, we evaluated the association of any comorbidity with non-MS-related hospitalizations. Any comorbidity was associated with a 2-fold increased risk of non-MS-related hospitalizations (aRR 2.50; 95% CI 1.88–3.27). The association of any comorbidity with hospitalization rates in the matched population was higher (aRR 3.85; 95% CI 3.40–4.35). After also adjusting for annual number of physician visits, the associations between comorbidity and hospitalization rates were attenuated in the MS population (aRR 1.48; 95% CI 1.14–1.92) and in the matched population (aRR 1.87; 95% CI 1.54–1.96).
Because of the observed association between any comorbidity and hospitalization rates, we proceeded to evaluate the association between the number of comorbidities and hospitalization rates. We observed a dose-response relationship wherein all-cause and non-MS-related hospitalization rates increased as the number of comorbidities increased (table e-2), but the dose-response relationship was steeper in the matched population than in the MS population. Although these differences persisted after further adjustment for number of physician visits, they were attenuated substantially (table e-3).
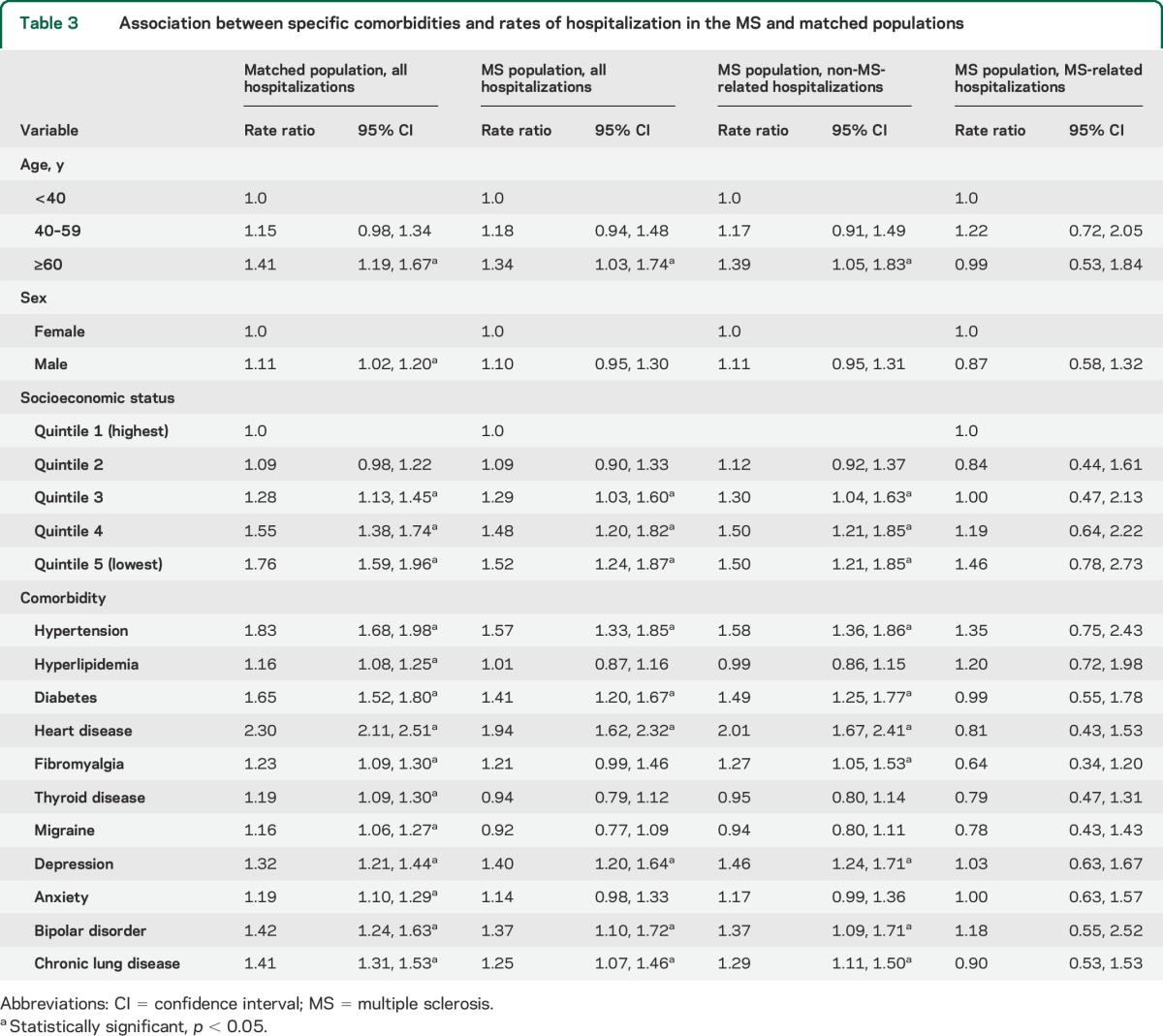
When we then evaluated the association of specific comorbidities and hospitalization rates, hypertension, diabetes, ischemic heart disease, chronic lung disease, depression, and bipolar disorder were associated with higher hospitalization rates in both populations (table 3). However, we also observed several differences between the 2 populations. Although hyperlipidemia, thyroid disease, and migraine were associated with higher rates of hospitalization in the matched population, this was not observed in the MS population. These differences persisted after adjusting for number of physician visits (data not shown).
Table 3.
Association between specific comorbidities and rates of hospitalization in the MS and matched populations
Comorbidity and MS-related hospitalizations.
Comorbidity was not associated with rates of hospitalization for MS-related reasons, regardless of how comorbidity status was defined (tables e-1, e-2, and 3). Adjustment for duration of MS did not alter the findings, nor did defining MS-related admissions solely by the primary discharge diagnosis (data not shown). The findings were also unchanged when we included admissions for long-term care and respite (table e-4).
DISCUSSION
Using population-based administrative data, we found that at least one comorbidity affected 85.9% of the MS population and 77.3% of the matched population. The psychiatric comorbidities of depression and anxiety affected more than 50% of the MS population over the study period. Several physical comorbidities affected more 25% of the MS population, including hypertension, hyperlipidemia, chronic lung disease, and migraine. In both populations, comorbidity was associated with increased hospitalization rates, in a dose-response relationship. In the MS population, comorbidity was associated with increased rates of hospitalization only for non-MS-related reasons.
We previously reported a declining rate of hospitalizations in the Manitoba MS population over a 25-year period ending in 2011.19 This may reflect changes in care, such as administration of relapse treatment in the outpatient rather than inpatient setting, or increased ascertainment of mild disease. As the delivery of health care has shifted many aspects of care from the inpatient to the outpatient setting, and chronic disease management has improved for some conditions, hospitalization rates in the general population have also declined but less in the last few years.29 Our findings are consistent with these observations.
Consistent with expectations, the burden of chronic disease and comorbidity was high in both populations studied. In the 2005 Canadian Community Health Survey, one-third of Canadians had one or more “high-impact” conditions, including hypertension, heart disease, diabetes, chronic lung disease, arthritis, cancer, and depression.30 The one-third of Canadians with these conditions accounted for nearly three-quarters of hospital days. Several studies suggest that comorbidity is common in prevalent MS populations, and have consistently found that depression and hypertension are the most frequent comorbidities, as we observed in the present study.1,4
According to the Anderson Behavioral Model, health care utilization is driven by predisposing factors (e.g., age, sex, SES), enabling or impeding factors that influence access to services (e.g., universal access in Manitoba), and the need for services (due to symptoms and illness).31 Consistent with this model and findings in the general population,29 we found that older age was associated with increased risks of hospitalization. Lower SES was also associated with increased hospitalization rates in a dose-response relationship, again consistent with published findings.32 After adjusting for the predisposing factors of age, sex, and SES, comorbidity was associated with increased hospitalization rates, and the risk of hospitalization increased with the number of comorbidities in both populations.
We observed several differences in the association of comorbidity with hospitalizations between the MS and matched populations. First, the presence of any comorbidity conferred a greater risk of hospitalization in the matched population than in the MS population and the dose-response relationship between number of comorbidities and hospitalization rates was not as steep in the MS population as in the matched population; in fact for 3 and 4 or more comorbidities the RR was 40% lower in the MS population than in the matched population. Second, some comorbidities that were common in the MS population, such as migraine and autoimmune thyroid disease, were associated with hospitalizations in the matched population but not the MS population. It is unlikely that these differences were simply due to the smaller size of the MS population and they were only partially attenuated when we accounted for physician services utilization. We can speculate as to why these differences were observed. Potential explanations include increased ascertainment of (possibly milder) comorbidity in the MS population due to the increased health care utilization occurring as a consequence of MS-related care, improved care of comorbidity in the MS population due to increased health care contacts,33 or some misclassification of hospitalizations as non-MS-related rather than MS-related.
In other chronic disease populations, such as congestive heart failure and epilepsy, comorbidity confers an increased risk of hospitalization overall.34,35 Comorbidity may also increase the risk of disease-specific hospitalizations. Further, psychiatric comorbidity is associated with reduced adherence to treatment in the general population,36 and to disease-modifying therapy in MS.37 Therefore, we had hypothesized that in the MS population, comorbidity would increase hospitalization rates for MS-related and non-MS-related reasons. Contrary to our hypothesis, comorbidity was associated only with increased risks of non-MS-related hospitalizations. We could not determine the specific reasons for MS-related admissions but if most MS-related hospitalizations were for relapses, our findings would be consistent with recent observations that dyslipidemia is not associated with relapses.38,39 Since several studies suggest that comorbidity adversely affects disability progression, comorbidity may not have the same effects on all aspects of MS. Alternatively, the adverse effects of comorbidity on MS may not be severe enough to increase the risk of hospitalization, or individuals with comorbidity and MS may receive better care of their MS due to increased health care contacts. Different comorbidities than those studied might also have different effects. This warrants further investigation.
Limitations of this study should be noted. We lacked clinical data for both study populations regarding functional status. We did not evaluate all possible comorbidities but we evaluated the comorbidities associated with adverse clinical outcomes in MS, and those for which we had carefully validated administrative case definitions. We used area-based rather than individual level measures of SES, but area-based measures provide similar findings as individual level measures when geographic units are small and capture a homogenous population.40 We did not evaluate outcomes after hospitalization, but outcomes and the influence of comorbidity on those outcomes deserve investigation in future studies. Replication of our findings in other jurisdictions is also needed. This study had several strengths including the population-based design, use of a matched cohort from the general population, and adjustment for age, sex, and SES, factors most strongly associated with health care utilization.
In the MS population, comorbidity is associated with an increased risk of all-cause hospitalizations, suggesting that the prevention and management of comorbidity may reduce hospitalizations. Comorbidities of particular interest based on their prevalence and associations with hospitalization include hypertension, heart disease, diabetes, and psychiatric conditions, for which effective therapies are available.
Supplementary Material
GLOSSARY
- aRR
adjusted rate ratio
- CI
confidence interval
- ICD-9
International Classification of Diseases–9
- MS
multiple sclerosis
- PHIN
personal health identification number
- RR
rate ratio
- SES
socioeconomic status
Footnotes
Editorial, page 335
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
The corresponding author (R.A.M.) and analyst (A.T.) had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Ruth Ann Marrie, Nancy Yu, and Lawrence Elliott designed the study and obtained funding. All authors contributed to the analysis and interpretation of the data. Ruth Ann Marrie drafted the manuscript. All authors revised the manuscript and approved of the final version to be published.
STUDY FUNDING
Supported by operating grants and a Don Paty Career Development Award from the MS Society of Canada. The funding sources had no role in the study design, collection, analysis or interpretation of the data, nor in the decision to submit the article for publication. The results and conclusions presented are those of the authors. No official endorsement by Manitoba Health is intended or should be inferred.
DISCLOSURE
R.A. Marrie receives research funding from the Canadian Institutes of Health Research, Public Health Agency of Canada, Manitoba Health Research Council, Health Sciences Centre Foundation, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, and Rx & D Health Research Foundation, and has conducted clinical trials funded by sanofi-aventis. L. Elliott receives research support from the Canadian Institutes of Health Research, Public Health Agency of Canada, and the Multiple Sclerosis Society of Canada. J. Marriott received research support for MS trials from Biogen Idec, Roche, and sanofi-aventis and honoraria from Biogen Idec, Roche, and EMD Serono. He has received research support from the Consortium of MS Centers and the Manitoba Medical Service Foundation. M. Cossoy has received an honorarium for educational activities from EMD Serono. A. Tennakoon reports no disclosures relevant to the manuscript. N. Yu receives research support from the Canadian International Development Agency, the Multiple Sclerosis Society of Canada, CIHR, and Manitoba Health. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Marrie RA, Horwitz R, Cutter G, Tyry T, Campagnolo D, Vollmer T. Comorbidity, socioeconomic status, and multiple sclerosis. Mult Scler 2008;14:1091–1098. [DOI] [PubMed] [Google Scholar]
- 2.Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328–337. [DOI] [PubMed] [Google Scholar]
- 3.Marrie RA, Horwitz RI, Cutter G, Tyry T, Campagnolo D, Vollmer T. Comorbidity delays diagnosis and increases disability at diagnosis in MS. Neurology 2009;72:117–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Warren SA, Turpin KV, Pohar SL, Jones CA, Warren KG. Comorbidity and health-related quality of life in people with multiple sclerosis. Int J MS Care 2009;11:6–16. [Google Scholar]
- 5.Canadian Institute for Health Information. The Burden of Neurological Diseases, Disorders and Injuries in Canada. Ottawa: Canadian Institute for Health Information; 2007. [Google Scholar]
- 6.McCrone P, Heslin M, Knapp M, Bull P, Thompson A. Multiple sclerosis in the UK: service use, costs, quality of life and disability. Pharmacoeconomics 2008;26:847–860. [DOI] [PubMed] [Google Scholar]
- 7.Kobelt G, Berg J, Lindgren P, Fredrikson S, Jonsson B. Costs and quality of life of patients with multiple sclerosis in Europe. J Neurol Neurosurg Psychiatry 2006;77:918–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pohar SL, Jones CA, Warren S, Turpin KV, Warren K. Health status and health care utilization of multiple sclerosis in Canada. Can J Neurol Sci 2007;34:167–174. [DOI] [PubMed] [Google Scholar]
- 9.Marrie RA, Yu N, Wei Y, Elliott L, Blanchard J. High rates of physician services utilization at least five years before multiple sclerosis diagnosis. Mult Scler 2013;19:1113–1119. [DOI] [PubMed] [Google Scholar]
- 10.Finlayson G, Ekuma O, Yogendran M, Burland E, Forget E. The Additional Cost of Chronic Disease in Manitoba. Winnipeg: Manitoba Centre for Health Policy; 2010. [Google Scholar]
- 11.Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med 2008;36:2787–2793. [DOI] [PubMed] [Google Scholar]
- 12.Lad S, Chapman C, Vaninetti M, Steinman L, Green A, Boakye M. Socioeconomic trends in hospitalization for multiple sclerosis. Neuroepidemiology 2010;35:93–99. [DOI] [PubMed] [Google Scholar]
- 13.Redelmeier DA, Tan SH, Booth GL. The treatment of unrelated disorders in patients with chronic medical diseases. N Engl J Med 1998;338:1516–1520. [DOI] [PubMed] [Google Scholar]
- 14.Manitoba Bureau of Statistics. Manitoba's Population Trends Past, Present and Future. Winnipeg: Manitoba Bureau of Statistics; 2008. [Google Scholar]
- 15.Health Information Management Branch. Population Report. Winnipeg: Manitoba Health and Healthy Living; 2008. [Google Scholar]
- 16.Marrie RA, Yu N, Blanchard JF, Leung S, Elliott L. The rising prevalence and changing age distribution of multiple sclerosis in Manitoba. Neurology 2010;74:465–471. [DOI] [PubMed] [Google Scholar]
- 17.Halpern NA, Bettes L, Greenstein R. Federal and nationwide intensive care units and healthcare costs: 1986-1992. Crit Care Med 1994;22:2001–2007. [PubMed] [Google Scholar]
- 18.Longobardi T, Bernstein CN. Health care resource utilization in IBD. Clin Gastroenterol Hepatol 2006;4:731–743. [DOI] [PubMed] [Google Scholar]
- 19.Marrie R, Elliott L, Marriott JJ, et al. Dramatically changing rates and reasons for hospitalization in multiple sclerosis. Neurology 2014;83:929–937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dallmeijer AJ, Beckerman H, de Groot V, van de Port IGL, Lankhorst GJ, Dekker J. Long-term effect of comorbidity on the course of physical functioning in patients after stroke and with multiple sclerosis. J Rehabil Med 2009;41:322–326. [DOI] [PubMed] [Google Scholar]
- 21.Fransoo R, Martens P, Burland E, Prior H, Burchill C; The Need to Know Team. Manitoba RHA Indicators Atlas 2009. Winnipeg: Manitoba Centre for Health Policy; 2009. [Google Scholar]
- 22.Marrie RA, Yu B, Leung S, et al. Rising prevalence of vascular comorbidities in MS: validation of administrative definitions for diabetes, hypertension, hyperlipidemia. Mult Scler 2012;18:1310–1319. [DOI] [PubMed] [Google Scholar]
- 23.Marrie RA, Yu BN, Leung S, et al. The Utility of administrative data for surveillance of comorbidity in multiple sclerosis: a validation study. Neuroepidemiology 2013;40:85–92. [DOI] [PubMed] [Google Scholar]
- 24.Marrie RA, Fisk JD, Yu BN, et al. Mental comorbidity and multiple sclerosis: validating administrative data to support population-based surveillance. BMC Neurol 2013;13:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Marrie RA, Yu BN, Leung S, et al. Prevalence and incidence of ischemic heart disease in multiple sclerosis: a population-based validation study. Mult Scler Relat Disord 2013;2:355–361. [DOI] [PubMed] [Google Scholar]
- 26.Marrie RA, Yu BN, Leung S, et al. The incidence and prevalence of fibromyalgia are higher in multiple sclerosis than the general population: a population-based study. Mult Scler Relat Disord 2012;1:162–167. [DOI] [PubMed] [Google Scholar]
- 27.Marrie RA, Yu BN, Leung S, et al. The incidence and prevalence of thyroid disease do not differ in the multiple sclerosis and general populations: a validation study using administrative data. Neuroepidemiology 2012;39:135–142. [DOI] [PubMed] [Google Scholar]
- 28.Booth GL, Hux JE. Relationship between avoidable hospitalizations for diabetes mellitus and income level. Arch Intern Med 2003;163:101–106. [DOI] [PubMed] [Google Scholar]
- 29.Canadian Institute for Health Information. Highlights of 2008–2009 Inpatient Hospitalizations and Emergency Department Visits. Ottawa: CIHI; 2010. [Google Scholar]
- 30.Broemeling A, Watson DE, Prebtani F; on behalf of the Councillors of the Health Outcomes Steering Committee of the Health Council of Canada. Population patterns of chronic health conditions, co-morbidity and health care use in Canada: implications for policy and practice. Healthc Q 2008;11:70–76. [DOI] [PubMed] [Google Scholar]
- 31.Andersen RM. National health surveys and the behavioral model of health services use. Med Care 2008;46:647–653. [DOI] [PubMed] [Google Scholar]
- 32.Alter DA, Naylor CD, Austin P, Tu JV. Effects of socioeconomic status on access to invasive cardiac procedures and on mortality after acute myocardial infarction. N Engl J Med 1999;341:1359–1367. [DOI] [PubMed] [Google Scholar]
- 33.Higashi T, Wenger NS, Adams JL, et al. Relationship between number of medical conditions and quality of care. N Engl J Med 2007;356:2496–2504. [DOI] [PubMed] [Google Scholar]
- 34.Braunstein JB, Anderson GF, Gerstenblith G, et al. Noncardiac comorbidity increases preventable hospitalizations and mortality among Medicare beneficiaries with chronic heart failure. J Am Coll Cardiol 2003;42:1226–1233. [DOI] [PubMed] [Google Scholar]
- 35.Lacey CJ, Salzberg MR, Roberts H, Trauer T, D'Souza WJ. Psychiatric comorbidity and impact on health service utilization in a community sample of patients with epilepsy. Epilepsia 2009;50:1991–1994. [DOI] [PubMed] [Google Scholar]
- 36.DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med 2000;160:2101–2107. [DOI] [PubMed] [Google Scholar]
- 37.Mohr DC, Goodkin DE, Likosky W, Gatto N, Baumann KA, Rudick RA. Treatment of depression improves adherence to interferon beta-1b therapy for multiple sclerosis. Arch Neurol 1997;54:531–533. [DOI] [PubMed] [Google Scholar]
- 38.Weinstock-Guttman B, Zivadinov R, Horakova D, et al. Lipid profiles are associated with lesion formation over 24 months in interferon-β treated patients following the first demyelinating event. J Neurol Neurosurg Psychiatry 2013;84:1186–1191. [DOI] [PubMed] [Google Scholar]
- 39.Tettey P, Simpson S, Jr, Taylor B, et al. Adverse lipid profile is not associated with relapse risk in MS: results from an observational cohort study. J Neurol Sci 2014;340:230–232. [DOI] [PubMed] [Google Scholar]
- 40.Mustard CA, Derksen S, Berthelot J-M, Wolfson M. Assessing ecologic proxies for household income: a comparison of household and neighbourhood level income measures in the study of population health status. Health Place 1999;5:157–171. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.