

Highlights
-
•
This is the first reported case in the literature describing a recurrent ectopic pregnancy with a fetal heartbeat after ipsilateral salpingectomy that led to tubal rupture.
-
•
Although exceptionally rare, recurrent ectopic pregnancy may occur after ipsilateral salpingectomy.
-
•
Physicians should be aware that ectopic pregnancies may not only occur repeatedly but may also present atypically.
-
•
We recommend when performing a salpingectomy that efforts be undertaken to minimize the length of the tubal remnant and to assure adequate coagulation of tissue so as to reduce the risk of recurrence.
Keywords: Tubal, Ectopic, Ipsilateral, Salpingectomy, Recurrent
Abstract
Introduction
Ectopic pregnancy accounts for 1–2% of all pregnancies in the United States. The most common site of implantation for an ectopic pregnancy is the fallopian tube. We present the first case describing a recurrent ectopic pregnancy with a fetal heartbeat after ipsilateral salpingectomy that led to tubal rupture.
Presentation of case
The patient presented with abdominal pain approximately six weeks after her last menstrual period. Seven years prior to presentation, a laparoscopic partial right salpingectomy had been performed for a tubal ectopic pregnancy. Physical exam was significant for diffuse abdominal tenderness and guarding. Ultrasonography revealed a right tubal pregnancy with a fetal pole and a fetal heart rate that was calculated to be 108 beats per minute. Free fluid was also noted. 1.5 l of hemoperitoneum was subsequently evacuated and the right fallopian tube remnant with the ectopic pregnancy was removed. Pathology of the tubal remnant showed immature chorionic villi and fetal parts.
Discussion
The mechanism by which a recurrent ectopic pregnancy after ipsilateral salpingectomy occurs is unclear, but is theorized to be secondary to contralateral fertilization and/or tubal recanalization that may occur due to inadequate diathermy.
Conclusion
Physicians should be aware that ectopic pregnancies may not only occur repeatedly but may also present a typically. We recommend when performing a salpingectomy that efforts be undertaken to minimize the length of the tubal remnant and to assure adequate coagulation of tissue so as to reduce the risk of recurrence.
1. Introduction
Ectopic pregnancy accounts for 1–2% of all pregnancies in the United States and has been associated with 75% of deaths in the first trimester of pregnancy and 9–13% of all pregnancy-related deaths [1]. The most common site of implantation for an ectopic pregnancy is the fallopian tube [2]. Current surgical management typically consists of salpingostomy, fimbrial evacuation or salpingectomy. Appropriate management is critical in preventing complications. Tubal surgery has been reported to be the greatest risk factor for ectopic pregnancy. Other important risk factors include prior pelvic inflammatory disease, history of multiple sexual partners, smoking, intrauterine device use, prior spontaneous or induced abortion and assisted reproductive technology [3].
In this report, we present a case of a spontaneously conceived pregnancy with a fetal heartbeat in the fallopian tube remnant after ipsilateral salpingectomy. The spontaneous occurrence of a pregnancy in a fallopian tube remnant after ipsilateral salpingectomy is exceedingly rare with fifteen cases that have been published in the literature. Even less common is the presence of a fetal heartbeat in such a pregnancy of which only one other case has been reported. This case bears the distinction of being the first reported of a spontaneous live recurrent ectopic pregnancy after ipsilateral salpingectomy that subsequently led to tubal rupture.
2. Presentation of case
A 27 year old G5P1031 presented to the emergency room with severe abdominal pain that started approximately six weeks after her last menstrual period. Past history consisted of a laparoscopic right salpingectomy that occurred seven years prior for a tubal ectopic pregnancy. This was followed by a normal spontaneous vaginal delivery, a spontaneous abortion and a left tubal ectopic pregnancy that was treated with methotrexate. On physical examination, the patient was normotensive but tachycardic. Abdominal examination was significant for diffuse tenderness and guarding. Pelvic examination indicated a normal-sized, anteverted uterus. No adnexal masses were palpated. Serum quantitative beta HCG was 9111 mIU/mL. Hemoglobin and hematocrit were 13.1 g/dL and 38.9%, respectively. Transvaginal ultrasonography confirmed the absence of an intrauterine pregnancy (Fig. 1a) and the presence of a right tubal ectopic pregnancy with a crown rump length of 0.3 centimeters, corresponding to a gestational age of 5 weeks and 6 days (Fig. 1b), and a fetal heart rate that was calculated to be 108 beats per minute (Fig. 1c). A left corpus luteal cyst and free pelvic fluid were also noted (Fig. 1d).
Fig. 1.
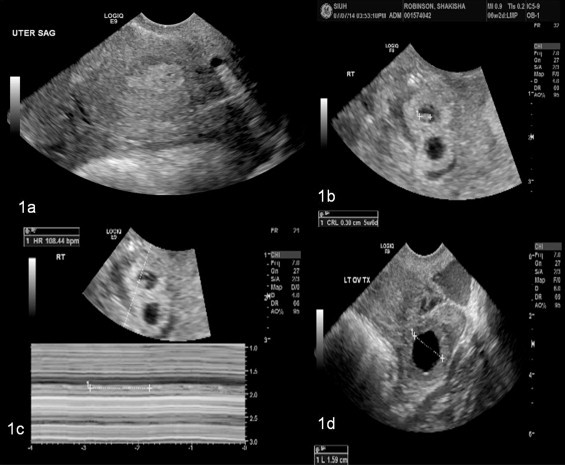
(a) Sagittal view of uterus. No intrauterine pregnancy visualized. (b) Right tubal ectopic pregnancy with crown rump length of 0.3 centimeters, corresponding a gestational age of 5 weeks and 6 days. (c) Measurement of fetal heartbeat in right tubal ectopic is 108 beats per minute. (d) Left corpus luteal cyst was noted.
Laparoscopic evaluation revealed 1.5 l of hemoperitoneum and evidence of a prior right salpingectomy and an ectopic pregnancy in the right proximal tubal remnant (Fig. 2a). The right ovary and left fallopian tube appeared normal. The left ovary appeared to have a corpus luteal cyst. Hemoperitoneum was evacuated. The right tubal remnant was resected (Fig. 2b). Postoperative course was uneventful and the patient was discharged on postoperative day 1. Pathology of the tubal remnant showed immature chorionic villi and fetal parts.
Fig. 2.
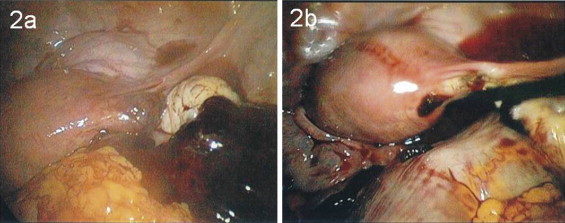
(a) Laparoscopy confirmed an ectopic pregnancy within the remnant of the right fallopian tube. Hemoperitoneum is also present. (b) Right aspect of uterus after removal of fallopian tube remnant.
3. Discussion
Although pregnancies in the fallopian tube account for 95% of all ectopic pregnancies, an ectopic pregnancy in the fallopian tube remnant after ipsilateral salpingectomy is exceptionally rare and may portend serious complications [4]. Isthmic pregnancies are considered to be gynecologic emergencies and are associated with mortality rates of 2.0–2.5%, substantially higher than the rate of 0.14% associated with other ectopic pregnancies [5]. This high mortality rate may be attributed to the inability of this portion of the fallopian tube to distend and the increased vascularity in this area given the presence of anastomoses between the uterine and ovarian arteries [6]. Table 1 shows a list of reported cases of recurrent tubal ectopic pregnancies after ipsilateral salpingectomy based on a PUBMED search using the search words, “ectopic pregnancy after salpingectomy.” The cases in bold indicate those associated with a fetal heartbeat.
Table 1.
Summary of findings associated with previously reported cases of spontaneous recurrent tubal ectopic after ipsilateral salpingectomy.
| Source | Age | Parity | Ectopic history | Procedures performed |
|---|---|---|---|---|
| Lema [11] | 31 | 0 | Three consecutive ipsilateral tubal pregnancies |
Milking ectopic pregnancy, (first, second); partial salpingectomy (third) |
| Mathew et al. [12] | 25 | 2 | Three consecutive ipsilateral tubal pregnancies in the left tube | Partial salpingectomy (first), resection of tubal stump (second, third) |
| Rizos et al. [13] | 33 | 0 | Recurrent ectopic pregnancy in the ipsilateral fallopian tube after endoloop salpingectomy | Endoloop, total salpingectomy |
| Zuzarte et al. [14] | 32 | 0 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Tan et al. [15] | 27 | 1 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Milingros et al. [16] | 38 | 4 | Three consecutive ipsilateral tubal pregnancies |
Partial salpingectomy (first and second), resection of cornua (third) |
| Chou and Huang [17] | 23 | 1 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Liu et al. [7] | 28 | 0 | Recurrent ipsilateral ectopic pregnancy following a partial salpingectomy for ectopic gestation | Partial salpingectomy |
| Chou et al. [9] | 38 | NA | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Chou et al. [9] | 38 | NA | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Longoria et al.[18] | 44 | 5 | Recurrent twin ectopic pregnancy following ipsilateral partial salpingectomy, fetal heart beat present | Partial salpingectomy |
| Samiei-Sarir and Diehm [8] | 42 | 7 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Samiei-Sarir and Diehm [8] | 35 | 2 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Drakopoulos et al. [19] | 33 | 3 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy | Partial salpingectomy |
| Present case | 27 | 1 | Recurrent ectopic pregnancy following ipsilateral partial salpingectomy, fetal heart beat presentàtubal rupture | Partial salpingectomy |
The mechanism by which a recurrent ectopic pregnancy after ipsilateral salpingectomy occurs is unclear. Three theories have been developed. The first proposes that contralateral fertilization occurred and the fertilized egg migrated across the endometrial cavity to the fallopian tube remnant [7]. The second suggests that in spite of a salpingectomy being performed, recanalization may occur due to inadequate diathermy allowing for passage of the ovum on the damaged side into the tubal remnant [8]. The third implies that spermatozoa pass through the patent fallopian tube and travel to fertilize the ovum on the damaged side [9]. Nonetheless, the existence of such cases advocates for a more aggressive surgical approach in the management of ectopic pregnancy when the contralateral fallopian tube appears healthy. Furthermore, studies have reported that salpingectomy is associated with a lower rate of persistent trophoblast than salpingostomy [10]. These cases also emphasize the importance of early diagnosis and management of ectopic pregnancies.
4. Conclusion
This is the first reported case in the literature describing a recurrent ectopic pregnancy with a fetal heartbeat after ipsilateral salpingectomy that led to tubal rupture. Although exceptionally rare, recurrent ectopic pregnancy may occur after ipsilateral salpingectomy. Physicians should be aware that ectopic pregnancies may not only occur repeatedly but may also present a typically. We recommend when performing a salpingectomy that efforts can be undertaken to minimize the length of the tubal remnant and to assure adequate coagulation of tissue so as to reduce the risk of recurrence.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Sources of funding
None.
Ethical approval
Not applicable.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author contribution
Both authors wrote the manuscript and performed the surgery described.
Guarantor
The guarantor is Cynthia Abraham.
References
- 1.Farquhar C.M. Ectopic pregnancy. Lancet. 2005;366(August 13–19(9485)):583–591. doi: 10.1016/S0140-6736(05)67103-6. [DOI] [PubMed] [Google Scholar]
- 2.Bouyer J., Coste J., Fernandez H., Pouly J.L., Job-Spira N. Sites of ectopic pregnancy: a 10-year population-based study of 1800 cases. Hum. Reprod. 2002;17:3224–3230. doi: 10.1093/humrep/17.12.3224. [DOI] [PubMed] [Google Scholar]
- 3.Bouyer J., Coste J., Shojaei T., Pouly J.L., Fernandez H., Gerbaud L., Job-Spira N. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population based study in France. Am. J. Epidemiol. 2003;157:185–194. doi: 10.1093/aje/kwf190. [DOI] [PubMed] [Google Scholar]
- 4.Dialani V., Levine D. Ectopic pregnancy: a review. Ultrasound Q. 2004;20:105–117. doi: 10.1097/00013644-200409000-00005. [DOI] [PubMed] [Google Scholar]
- 5.Lau S., Tulandi T. Conservative medical and surgical management of interstitial ectopic pregnancy. Fertil. Steril. 1999;72(2):207–215. doi: 10.1016/s0015-0282(99)00242-3. [DOI] [PubMed] [Google Scholar]
- 6.Takeda A., Manabe S., Mitsui T., Nakamura H. Spontaneous ectopic pregnancy occurring in the isthmic portion of the remnant tube after ipsilateral adnexectomy: report of two cases. J. Obstet. Gynaecol. Res. 2006;32(2):190–194. doi: 10.1111/j.1447-0756.2006.00385.x. [DOI] [PubMed] [Google Scholar]
- 7.Liu Y.L., Hwang K.S., Chu P.W., Ding D.C. Recurrent ectopic pregnancy in the ipsilateral oviduct after prior laparoscopic partial salpingectomy. Taiwan. J. Obstet. Gynecol. 2009;48(December (4)):417–419. doi: 10.1016/S1028-4559(09)60335-1. [DOI] [PubMed] [Google Scholar]
- 8.Samiei-Sarir B., Diehm C. Recurrent ectopic pregnancy in the tubal remnant after salpingectomy. Case Rep. Obstet. Gynecol. 2013;2013:753269. doi: 10.1155/2013/753269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chou S.Y., Hsu M.I., Chow P.K., Chiang H.K., Su H.W., Hsu C.S. Recurrent ipsilateral ectopic pregnancy after partial salpingectomy. Taiwan. J. Obstet. Gynecol. 2009;48(December (4)):420–422. doi: 10.1016/S1028-4559(09)60336-3. [DOI] [PubMed] [Google Scholar]
- 10.Yao M., Tulandi T. Current status of surgical and nonsurgical management of ectopic pregnancy. Fertil. Steril. 1997;67:421–433. doi: 10.1016/s0015-0282(97)80064-7. [DOI] [PubMed] [Google Scholar]
- 11.Lema V.M. Three consecutive ipsilateral tubal pregnancies in a nulliparous African woman: the role of conservative treatment. Central Afr. J. Med. 1995;41:62–66. [PubMed] [Google Scholar]
- 12.Mathew M., Kumari R., Gowri V. Three consecutive ipsilateral tubal pregnancies. Int. Gynaecol. Obstet. 2002;78:163–164. doi: 10.1016/s0020-7292(02)00134-0. [DOI] [PubMed] [Google Scholar]
- 13.Rizos A., Eyong E., Yassin A. Recurrent ectopic pregnancy at the ipsilateral fallopian tube following laparoscopic partial salpingectomy with endo-loop ligation. J. Obstet. Gynaecol. 2003;23:678–679. doi: 10.1080/01443610310001609524. [DOI] [PubMed] [Google Scholar]
- 14.Zuzarte R., Khong C.C. Recurrent ectopic pregnancy following ipsilateral partial salpingectomy. Singapore Med. J. 2005;46:476–488. [PubMed] [Google Scholar]
- 15.Tan T.L., Elashry A., Tischner I., Jolaoso A. Lightning does strike twice: recurrent ipsilateral tubal pregnancy following partial salpingectomy for ectopic pregnancy. J. Obstet. Gynaecol. 2007;27:534–535. doi: 10.1080/01443610701467606. [DOI] [PubMed] [Google Scholar]
- 16.Milingos D.S., Black M., Bain C. Three surgically managed ipsilateral spontaneous ectopic pregnancies. Obstet. Gynecol. 2008;112(August 2 (Pt 2)):458–459. doi: 10.1097/AOG.0b013e31816baec0. [DOI] [PubMed] [Google Scholar]
- 17.Chou L.L., Huang M.C. Recurrent ectopic pregnancy after ipsilateral segmental salpingectomy. Taiwan. J. Obstet. Gynecol. 2008;47(June (2)):203–205. doi: 10.1016/S1028-4559(08)60081-9. [DOI] [PubMed] [Google Scholar]
- 18.Longoria T.C., Stephenson M.L., Speir V.J. Live unilateral twin ectopic pregnancy in a fallopian tube remnant after previous ipsilateral salpingectomy. J. Clin. Ultrasound. 2014;42(March–April (3)):169–171. doi: 10.1002/jcu.22074. [DOI] [PubMed] [Google Scholar]
- 19.Drakopoulos P., Julen O., Petignat P., Dällenbach P. Spontaneous ectopic tubal pregnancy after laparoscopic tubal sterilisation by segmental isthmic partial salpingectomy. BMJ Case Rep. 2014;2014(March (22)) doi: 10.1136/bcr-2013-203131. [DOI] [PMC free article] [PubMed] [Google Scholar]