

Abstract
Caffeine (1,3,7-trimethylxanthine) is a popular mild central nervous system stimulant found in the leaves, seeds and fruits of various plants and in foodstuffs such as coffee, tea, and chocolate, among others. Caffeine is widely used and is not associated with severe side effects when consumed at relatively low doses. Although rarely observed, overdoses can occur. However, only a few fatal caffeine intoxication cases have been reported in the literature. Herein, we report the pathological examination results and information on caffeine concentrations in the blood, urine and main organs in a fatal caffeine intoxication case. Even though high caffeine concentrations were found in the systemic organs, no caffeine-related pathological changes were detected.
Keywords: caffeine, intoxication, autopsy, pathology, suicide
Caffeine (1,3,7-trimethylxanthine) is a naturally occurring mild central nervous system stimulant found in the leaves, seeds, and fruits of various natural plants. Common foodstuffs that contain caffeine include coffee, tea, and chocolate, among others1, 2. When relatively low doses are consumed, severe side effects are uncommon. However, larger concentrations of caffeine are now being added to energy drinks or are being taken as dietary supplements3. Clinically, caffeine intoxication presents with headache, nausea, vomiting, fever, hyperventilation, dizziness, anxiety, tinnitus, tremor, and agitation4. In overdose cases, hypertension, hypotension, arrhythmia, and seizures have been reported5. Although the acute level of caffeine consumption has yet to be definitively established, it is thought to be approximately 10 g per day in adults, which is comparable to consuming around 100 cups of coffee6. However, it can be difficult to determine the cause of death in patients who do overdose, as they lack specific diagnostic symptoms. Thus, blood caffeine concentrations can be used to help make a definitive diagnosis in such patients.
Only a few fatal caffeine intoxication cases have been reported in the medical literature. A study by Silva et al. found that out of 15 case reports on attempted suicides that used caffeine, only 7 fatalities occurred7. In the current study, we present the pathological examination performed in a fatal caffeine intoxication case, along with information on the caffeine concentrations found in the blood, urine, and main organs.
An 18-year-old woman was found dead in her bed at home. Although she had been suffering from depression, she was not taking any medication for her condition. A large amount of vomit was observed around her mouth, and her room contained 258 empty blister packs of an over-the-counter sleep inhibitor product. Each of the individual tablets in the blister pack contained caffeine (200 mg/tablet) and some vitamins. An autopsy of her systemic organs was performed 17 hours after her death. External examination revealed no injuries to her body. Her height was 162 cm, and her weight was 47 kg. Examination of her organs revealed her heart weighed 210 g and had no observable coronary artery abnormalities, her brain weighed 1,540 g and looked edematous, her left and right lungs weighed 130 g and 160 g, respectively, and there was 135 g of gastrointestinal contents, which contained many drug particles (Fig. 1). Large amounts of a gray-white particulate were observed from the mouth to the upper intestine, and there was diffuse bleeding of the gastric mucosa. At autopsy, systemic organs including the brain were fixed in 10% buffered formalin, embedded in paraffin, sectioned, and stained with hematoxylin and eosin (H & E) for routine histopathologic examinations. While mild erosion of the stomach with hemorrhage (Fig. 2a) and brain edema (Fig. 2b) were seen, there were nonspecific changes in many of the organs, including the heart (Fig. 2c), lungs (Fig. 2d), liver and kidneys.
Fig. 1.

Macroscopic findings of the stomach. Hemorrhagic fluid contained many gray-white drug particles. The gastric mucosa showed diffuse hemorrhage.
Fig. 2.

Histopathology of the stomach, heart, and lung. (a) Gastric erosion with hemorrhage. Inflammatory cell infiltration is not seen because of the early phase of the lesion. (b) Edematous change of the cerebrum. Note the submeningeal and perivascular area. (c) No caffeine-related changes are observed in the heart. (d) No caffeine-related changes are observed in the lungs. H & E staining, ×200.
For the toxicological analyses, 0.2 ml/g extracts were obtained from the heart blood, urine, gastric contents, brain, lung, heart, liver, kidney, skeletal muscle (quadriceps) and skin. Caffeine-d3 was used as the internal standard (IS). Gastric contents were diluted before extraction. Organs were prepared by homogenizing the tissue and then adding the IS. Each preparation was extracted using 2 ml of acetonitrile containing 0.1 ml of aqueous ammonia. Our analysis was based on our previously reported method and used the following equipment: GCMS-QP2010 Ultra Gas Chromatograph Mass Spectrometer (Shimadzu, Kyoto, Japan) with a BPX-5 (2 m × 0.25 mm i.d., membrane thickness 0.5 µm)/BPX-5 (4 m × 0.15 mm i.d., membrane thickness 0.25 µm) column (SGE Analytical Sciences, Ringwood, Victoria, Australia)8.
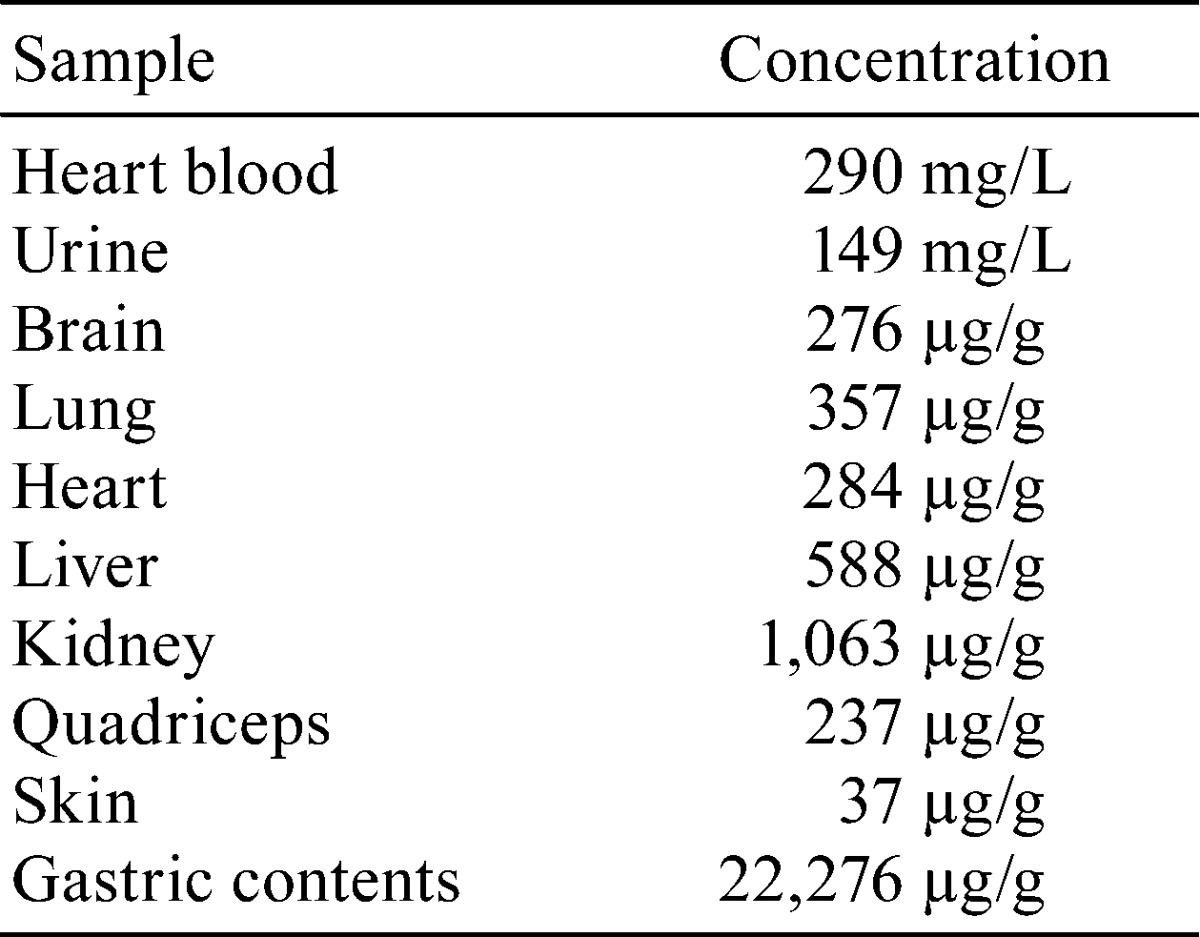
Our analyses indicated that there was no alcohol in the peripheral blood or urine. However, as seen in Table 1, our toxicological tests did show there were large amounts of caffeine in many of the tested samples, including 22,276 µg/g in the gastric contents, 1,063 µg/g in the kidney, 588 µg/g in the liver, 357 µg/g in the lung, 290 mg/L in the peripheral blood, 284 µg/g in the heart, 276 µg/g in the brain, 237 µg/g in the skeletal muscle (quadriceps), 149 mg/L in the urine, and 37 µg/g in the skin. The cause of death was determined to be fatal caffeine intoxication, with the police investigation considering the manner of death to be a suicide.
Table 1. Caffeine Concentration in the Blood and Organs.
An average cup of coffee contains an estimated 100 mg of caffeine. Numerous dietary supplements, over-the-counter drugs and various prescription drug mixtures also contain caffeine, with doses ranging from 30–200 mg2, 5. Mild stimulation is usually associated with a caffeine dose of 50–200 mg5. After oral intake, caffeine is rapidly absorbed, and clinical effects are observed within 15 minutes, with peak plasma levels attained within one hour after ingestion1. Caffeine is metabolized via hepatic N-demethylation, acetylation and oxidation9. Experiments investigating the toxicity of oral caffeine in animals revealed that the LD50 was 200–400 mg/kg in rats and 185 mg/kg in mice. The no observed adverse effect level was determined to be 150–174 mg/kg body weight/day in rats and 167–179 mg/kg body weight/day in mice. Caffeine toxicity was examined in rats over a period of 100 days by administering 110 mg/kg caffeine daily via intragastric cannulas10. The results showed stressor reactions such as adrenal cortex hypertrophy and thymic atrophy, gastric ulcer, and hypertrophy of the salivary glands, liver, heart, kidney, and lung. Thus, in order to achieve fatal blood concentrations of 80–100 mg/L in humans, a person would need to ingest 50–100 tablets of 100 mg pure caffeine9.
Caffeine is a natural alkaloid methylxanthine that is structurally similar to adenosine and can block the adenosine receptor. It increases the intracellular calcium concentration, causes noradrenaline release and sensitizes dopamine receptors, which can trigger arrhythmia. It has been speculated that caffeine’s mechanism of death is usually associated with ventricular arrhythmia. Other studies have suggested that caffeine-associated seizures may be another possible mechanism1, 5, 11. In the present case, 258 empty packs of an over-the-counter sleep inhibitor product, which was assumed to contain about 50 g of caffeine, was found next to the deceased. There still remained many drug particles in the stomach, and the mucosa of the stomach showed mild erosion without inflammatory cell infiltration, which means the blood caffeine concentration rapidly increased and the deceased died before inflammatory cell infiltration. The concentration was 290 mg/L, which is consistent with concentrations found in previously reported suicide cases1, 2, 5, 9, 11. However, there was no congestion or edema of the lungs, which is inconsistent with typical acute vascular collapse. It appears unlikely that the mechanism of death in the present case was just arrhythmia. Some reports have mentioned that caffeine causes severe rhabdomyolysis and acute renal failure, but in the present case, the kidneys showed no pathological change of acute renal failure12. Unfortunately we were not able to determine the exact mechanism of death, but we speculated that the brain showed edematous changes, which suggests that death could have possibly been due to respiratory arrest caused by caffeine-induced brain functional damage.
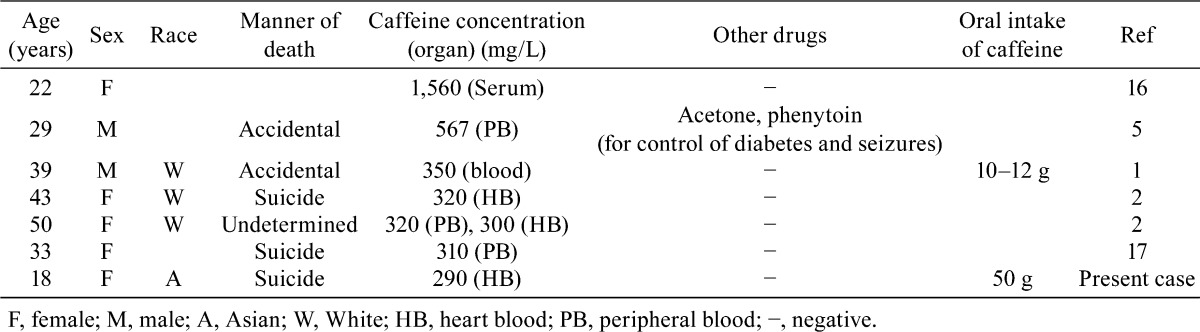
We reviewed previous caffeine intoxication reports in the literature, especially those that resulted in the death of the subject (Table 2). In the majority of cases, caffeine was taken in conjunction with other drugs2, 5, 9, 11, 13. In a large number of these cases, ethanol was found in addition to caffeine2, 9, 13. The concentration of caffeine detected in the non-ethanol cases tended to be higher than that found when caffeine was used in combination with ethanol (Table 2). The caffeine concentration in the present case was much higher than the concentrations that have been commonly reported in other fatal cases.
Table 2. High Caffeine Concentrations in Subjects who Subsequently Died.
Examination of the caffeine concentration in the main organs revealed there was caffeine distribution to the systemic organs. The caffeine concentration was especially high in the kidney. An animal experiment demonstrated that caffeine was distributed to and accumulated in the brain, kidney and liver of male Wistar rats14. In a human case, Bonsignore et al. also reported finding that there was distribution of caffeine in the systemic organs9. The distribution in the present case was consistent with these previous results. It should be noted that not only the arrhythmia mechanism, but also other organ damage could potentially contribute to the death in these types of cases. Recently, there has been an increase in illegal drug use in Japan. Unlike problems with illegal drugs, caffeine is legal and can be very easily obtained. Furthermore, although many people commonly consume this drug in the form of energy drinks or dietary supplements, the risk of using it is not widely known. To date, there have been no previous reports in Japan of fatal caffeine intoxication occurring as a result of only consuming caffeine by itself15. Even so, there should be a heightened awareness of the potential dangers of a caffeine overdose.
We made our best effort to ensure that readers could not identify the patient in this case report.
Declaration of Conflicting Interests: The authors declare that they have no competing interests.
References
- 1.Jabbar SB, and Hanly MG. Fatal caffeine overdose: a case report and review of literature. Am J Forensic Med Pathol. 34: 321–324. 2013. [DOI] [PubMed] [Google Scholar]
- 2.Banerjee P, Ali Z, Levine B, and Fowler DR. Fatal caffeine intoxication: a series of eight cases from 1999 to 2009. J Forensic Sci. 59: 865–868. 2014. [DOI] [PubMed] [Google Scholar]
- 3.Reissig CJ, Strain EC, and Griffiths RR. Caffeinated energy drinks—a growing problem. Drug Alcohol Depend. 99: 1–10. 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rudolph T, and Knudsen K. A case of fatal caffeine poisoning. Acta Anaesthesiol Scand. 54: 521–523. 2010. [DOI] [PubMed] [Google Scholar]
- 5.Kerrigan S, and Lindsey T. Fatal caffeine overdose: two case reports. Forensic Sci Int. 153: 67–69. 2005. [DOI] [PubMed] [Google Scholar]
- 6.Heckman MA, Weil J, and Gonzalez de Mejia E. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci. 75: R77–R87. 2010. [DOI] [PubMed] [Google Scholar]
- 7.Silva AC, de Oliveira Ribeiro NP, de Mello Schier AR, Pereira VM, Vilarim MM, Pessoa TM, Arias-Carrión O, Machado S, and Nardi AE. Caffeine and suicide: a systematic review. CNS Neurol Disord Drug Targets. 13: 937–944. 2014. [DOI] [PubMed] [Google Scholar]
- 8.Waters B, Hara K, Kashiwagi M, Matsusue A, Sugimura T, Hamasato S, and Kubo S. Combination of a short middle-bore capillary column with a thicker stationary phase and a short narrow-bore separation column with a thinner stationary phase for the rapid screening of non-volatile drugs by gas chromatography–mass spectrometry. Forensic Toxicol. 31: 67–69. 2013. [Google Scholar]
- 9.Bonsignore A, Sblano S, Pozzi F, Ventura F, Dell’Erba A, and Palmiere C. A case of suicide by ingestion of caffeine. Forensic Sci Med Pathol. 10: 448–451. 2014. [DOI] [PubMed] [Google Scholar]
- 10.National Toxicology Program (NTP) CAS registry Number: 58-08-2 Toxicity effects. 2014. http://ntp.niehs.nih.gov/testing/status/chemid/hsdb-58-08-2.html.
- 11.Holmgren P, Nordén-Pettersson L, and Ahlner J. Caffeine fatalities—four case reports. Forensic Sci Int. 139: 71–73. 2004. [DOI] [PubMed] [Google Scholar]
- 12.Campana C, Griffin PL, and Simon EL. Caffeine overdose resulting in severe rhabdomyolysis and acute renal failure. Am J Emerg Med. 32: 111.e3–111.e4. 2014. [DOI] [PubMed] [Google Scholar]
- 13.Caughlin LJ, and O’Halloran RL. An accidental death related to cocaine, cocaethylene, and caffeine. J Forensic Sci. 38: 1513–1515. 1993. [PubMed] [Google Scholar]
- 14.Che B, Wang L, Zhang Z, Zhang Y, and Deng Y. Distribution and accumulation of caffeine in rat tissues and its inhibition on semicarbazide-sensitive amine oxidase. Neurotoxicology. 33: 1248–1253. 2012. [DOI] [PubMed] [Google Scholar]
- 15.Takase I, Yamamoto Y, Nakagawa T, and Nishi K. A fatal case of potential chronic overdoses of prescribed and proprietary remedies. Hum Exp Toxicol. 29: 695–699. 2010. [DOI] [PubMed] [Google Scholar]
- 16.Mrvos RM, Reilly PE, Dean BS, and Krenzelok EP. Massive caffeine ingestion resulting in death. Vet Hum Toxicol. 31: 571–572. 1989. [PubMed] [Google Scholar]
- 17.Thelander G, Jönsson AK, Personne M, Forsberg GS, Lundqvist KM, and Ahlner J. Caffeine fatalities—do sales restrictions prevent intentional intoxications? Clin Toxicol (Phila). 48: 354–358. 2010. [DOI] [PubMed] [Google Scholar]