

Abstract
Background
Many SNPs influence prostate cancer risk. To what extent genetic risk can be reduced by environmental factors is unknown.
Methods
We evaluated effect modification by environmental factors of the association between susceptibility SNPs and prostate cancer in 1,230 incident prostate cancer cases and 1,361 controls, all white and similar ages, nested in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Trial. Genetic risk scores were calculated as number of risk alleles for 20 validated SNPs. We estimated the association between higher genetic risk (≥ 12 SNPs) and prostate cancer within environmental factor strata and tested for interaction.
Results
Men with ≥12 risk alleles had 1.98, 2.04, and 1.91 times the odds of total, advanced, and nonadvanced prostate cancer, respectively. These associations were attenuated with the use of selenium supplements, aspirin, ibuprofen, and higher vegetable intake. For selenium, the attenuation was most striking for advanced prostate cancer: compared with <12 alleles and no selenium, the OR for ≥12 alleles was 2.06 [95% confidence interval (CI), 1.67–2.55] in nonusers and 0.99 (0.38–2.58) in users (Pinteraction = 0.031). Aspirin had the most marked attenuation for nonadvanced prostate cancer: compared with <12 alleles and nonusers, the OR for ≥12 alleles was 2.25 (1.69–3.00) in nonusers and 1.70 (1.25–2.32) in users (Pinteraction = 0.009). This pattern was similar for ibuprofen (Pinteraction = 0.023) and vegetables (Pinteraction = 0.010).
Conclusions
This study suggests that selenium supplements may reduce genetic risk of advanced prostate cancer, whereas aspirin, ibuprofen, and vegetables may reduce genetic risk of nonadvanced prostate cancer.
Introduction
The predisposition to prostate cancer is multifactorial with important contributions from genetic and environmental factors. Recent studies have identified numerous low penetrance SNPs accounting for a proportion of prostate cancer susceptibility (1–3). Zheng and colleagues reported that prostate cancer risk increased with cumulative number of risk genotypes for five SNPs, and that when family history was additionally considered, men who had five or six risk factors—risk genotypes and/or family history–had a 9-fold increased prostate cancer risk compared with men with no risk genotypes and a negative family history (4). In addition, a Swedish study that combined prostate cancer risk alleles into a genetic risk score found that it predicted prostate cancer on biopsy among men with low PSA levels (1–3 ng/mL; ref. 5).
Numerous environmental factors have also been investigated in association with prostate cancer risk, including diet, exercise, and medications (6–8). The relative contribution of genes and environment to prostate carcinogenesis remains uncertain. A Scandinavian twin study suggested an overall heritability index of 42%, (9) indicating a major contribution also from environmental factors. Migration studies have shown that immigrants from low- to high-risk countries experience higher prostate cancer rates, further supporting that environmental factors are important (10).
Although genetic screening tests for diseases, including prostate cancer, are now commercially available to consumers, (11) these tests are controversial because they have not been shown to improve clinical outcomes, as demonstrated by the conflict between the FDA and the personal genomic testing company 23andme (12). Furthermore, no guidance is available on how the information from these tests can be used by patients and clinicians in healthcare decision-making (13). For example, if a man is found to be at higher genetic risk for prostate cancer, is there anything he can do to reduce his risk? At present, the answer to this question is unknown. Thus, the purpose of our study was to evaluate whether environmental factors, such as diet and lifestyle, modify the association between 20 validated prostate cancer susceptibility SNPs, previously identified including in genome-wide association studies (GWAS), and the risk of prostate cancer overall, and by stage and grade.
Materials and Methods
We performed an analysis of existing data from a GWAS performed in a case-control study nested in the screening arm of the Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial. These data are available in the Cancer Genetic Markers of Susceptibility database (http://cgems.cancer.gov; ref 1), and we accessed them under a confidentiality agreement. The PLCO included men ages 55 to 74 years at baseline recruited at 10 U.S. centers (14). Men in the prostate cancer-screening arm underwent yearly prostate-specific antigen (PSA) tests for 6 years and digital-rectal examinations (DRE) for 4 years. The trial investigators referred men with a PSA >4 ng/mL or suspicious DRE to their medical providers for further evaluation. All participants provided informed consent, and the Institutional Review Boards at all participating institutions approved the trial.
We included in this analysis 1,230 incident prostate cancer cases and 1,361 controls who were non-Hispanic white and were frequency-matched on age in 5-year intervals. Prostate cancer status was ascertained using the National Death Index and annual health history questionnaires, with confirmation and additional details on stage and grade obtained from review of the medical records. Nonadvanced-stage cases were defined as clinical stage I and II tumors. Advanced cases were defined as clinical stage III and IV (regional or distant). Gleason score was divided into low (Gleason ≤6), intermediate (Gleason 7), and high (Gleason ≥8) grade.
The participants completed a baseline questionnaire including demographics, education, past medical history, medications, smoking history, height, weight, and physical activity. Participants also completed a 137-item food frequency questionnaire to assess dietary patterns during the year before enrollment (15). This questionnaire included 14 questions about vitamin and mineral supplement use (16). Total intake of vitamins and minerals was calculated by adding intakes from diet and supplements. From these questionnaires, we selected environmental factors that are modifiable with the greatest consensus for further evaluation because they are purported risk or protective factors for prostate cancer or other major cancers (6, 7, 17). The factors we selected were: body mass index (BMI; at age 20, age 50, baseline); vigorous physical activity; smoking; alcohol drinking; aspirin use, ibuprofen use; intake of fruit, vegetables, broccoli, red meat (total, ruminants only), energy, fat, vitamin D, zinc, folate, and lycopene; use of a multivitamin (current, within the last 2 years), selenium supplement, vitamin E supplement; and high intake of calcium (primarily from supplement use).
The participants also provided a blood sample at baseline and/or subsequent screening years. DNA extracted from buffy coat was used for the prior GWAS study in the PLCO (1). We identified 20 SNPs previously associated with prostate cancer susceptibility and validated from the literature (Supplementary Table S1; refs. 1, 4, 18–24) and that had already been genotyped in the PLCO GWAS. Using the existing data, we calculated a genetic risk score for each man based on the number of risk alleles for the 20 SNPs. We defined a higher genetic risk score as carrying ≥12 risk alleles, the median number (and mode) in controls. No obvious threshold in the OR was present across number of risk alleles (see Results), thus we dichotomized at the median number of risk alleles to have roughly equal information in the two groups (under the null hypothesis). We used logistic regression to evaluate the association between higher genetic risk score and the risk of total prostate cancer as well as disease that was nonadvanced or advanced stage; low (Gleason ≤6), intermediate (Gleason 7), or high (Gleason ≥8) grade; and aggressive [either advanced stage (III–IV) or high grade (Gleason ≥8)] after adjusting for age (continuous) and attained education (college graduate or postgraduate vs. less than college graduate), a correlate of lifestyle and dietary factors. To identify effect modification, we stratified these associations by the environmental factors. To test for multiplicative interaction, we entered into the model (adjusting for age and education) terms for higher genetic risk score, the environmental factor, and their cross-product, the coefficient for which we evaluated using the Wald test. For nominally statistically significant interactions (P < 0.05), we further explored the nature of the multiplicative interaction by modeling joint associations. For the most robust interaction, we also evaluated the joint association across number of risk alleles using the mode (12 risk alleles) in the unexposed as the reference group. All tests were two sided and analyses were conducted using SAS v.9.3.
Results
Table 1 shows baseline characteristics of the study population. Prostate cancer cases and controls were similar on most characteristics, except that cases were less likely to have ever smoked and to currently use vitamin E supplements than controls, as in previous PLCO studies (15). Advanced-stage cases were older than controls and had less total folate intake. Nonadvanced-stage cases had a lower BMI at age 50 years compared with controls.
Table 1.
Baseline characteristics of prostate cancer cases and controls, PLCO
| Prostate cancer cases
|
||||
|---|---|---|---|---|
| Characteristics | Total | Advanced stage | Nonadvanced stage | Controls |
| Age (y), mean | 66.7 | 67.0a | 66.4 | 66.4 |
| College graduate or postgraduate, % | 41.5 | 39.5 | 44.0 | 40.2 |
| BMI (kg/m2), mean | ||||
| At age 20 y | 22.9 | 23.0 | 22.8 | 23.0 |
| At age 50 y | 26.3 | 26.4 | 26.1a | 26.6 |
| At baseline | 27.3 | 27.4 | 27.3 | 27.6 |
| Vigorous physical activity, % | ||||
| <1 h/wk | 12.2 | 13.1 | 11.0 | 14.1 |
| 1–3 h/wk | 43.9 | 43.6 | 44.3 | 45.3 |
| ≥4 h/wk | 43.9 | 43.3 | 44.7 | 40.6 |
| Smoking history, % | ||||
| Never smoker | 32.2b | 33.2 | 31.0 | 28.6 |
| Former (quit ≥10 y ago) | 42.0b | 40.3 | 44.2 | 42.0 |
| Former (quit <10 y ago) & cigar/pipe only | 17.8b | 18.6 | 16.7 | 18.3 |
| Current smoker | 8.0b | 7.9 | 8.1 | 11.1 |
| Alcohol use, % | ||||
| ≤1 drink/mo | 30.9 | 31.8 | 29.8 | 30.2 |
| >1 drink/mo to ≤1 drink/d | 36.9 | 38.6 | 34.9 | 38.6 |
| >1 drink/day | 32.2 | 29.6 | 35.3 | 31.2 |
| Aspirin use regularly, % | 42.6 | 41.8 | 43.5 | 45.9 |
| Ibuprofen use regularly, % | 14.1 | 13.6 | 14.8 | 15.7 |
| Fruit intake (pyramid servings/d), mean | 3.4 | 3.3 | 3.5 | 3.4 |
| Vegetable intake (pyramid servings/d), mean | 5.4 | 5.4 | 5.4 | 5.5 |
| Broccoli intake (g/d), mean | 13.9 | 13.8 | 14.1 | 14.0 |
| Red meat intake (g/d), mean | 96.9 | 97.5 | 96.0 | 100.2 |
| Red meat from ruminants intake (g/d), mean | 65.2 | 66.0 | 64.3 | 67.8 |
| Energy intake (kcal/d), mean | 2,337.4 | 2,293.4 | 2,390.5 | 2,348.2 |
| Fat intake (g/d), mean | 79.9 | 79.8 | 80.0 | 80.0 |
| Vitamin D intake (IU/d), mean | 10.7 | 10.3 | 11.2 | 10.9 |
| Folate intake (mcg/d), mean | 603.9 | 586.6a | 624.8 | 617.3 |
| Zinc intake (mg/d), mean | 20.5 | 20.1 | 21.0 | 20.7 |
| Lycopene intake from diet (μg/d), mean | 11,264.7 | 11,090.2 | 11,475.6 | 11,470.2 |
| Current multivitamin use, % | 34.5 | 33.3 | 36.0 | 33.7 |
| Recent multivitamin use (within past 2 y), % | 42.5 | 39.8 | 45.7 | 43.0 |
| Current selenium supplement use, % | 3.3 | 3.1 | 3.5 | 3.7 |
| Current vitamin E supplement use, % | 28.4a | 28.0 | 28.9 | 33.3 |
| Calcium intake ≥1,500 mg/d, % | 23.5 | 21.4 | 26.0 | 23.6 |
NOTE: Bold font indicates statistically significant values.
P < 0.05 versus controls.
The distribution of smoking history differs between total cases and controls, P < 0.05.
Men with ≥ 12 risk alleles had a greater risk of prostate cancer, including nonadvanced and advanced stage; low, intermediate, and high grade; and aggressive (stage III–IV or Gleason ≥8) disease (Table 2). Before stratification, risk of nonadvanced stage prostate cancer increased across number of risk alleles [OR (95% confidence interval (CI), ≤9 alleles: 0.49 (0.34–0.71); 10–11 alleles: 0.70 (0.51–0.97); 12 alleles: reference; 13 alleles: 1.07 (0.74–1.55), ≥14 alleles: 1.47 (1.04–2.09); Ptrend < 0.0001]. The risk of advanced-stage disease also increased across number of risk alleles; due to the smaller number of advanced-stage cases, we combined over categories [≤11 alleles: 0.63 (0.48–0.84); 12 alleles: reference; ≥13 alleles: 1.45 (1.08–1.94); Ptrend < 0.0001).
Table 2.
Association between higher genetic risk (≥12 risk alleles) and prostate cancer adjusted for age and education, stratified by environmental factors, PLCO
| OR (95% CI) of higher genetic risk (≥12 risk alleles)
|
|||||||
|---|---|---|---|---|---|---|---|
| Total | Nonadvanced stage | Advanced stage | Aggressive (advanced stage or Gleason sum ≥8) | Low grade (Gleason sum ≤6) | Intermediate grade (Gleason sum 7) | High grade (Gleason sum ≥8) | |
| Overall | 1.98 (1.67–2.34) | 1.91 (1.54–2.36) | 2.04 (1.67–2.49) | 1.73 (1.33–2.25) | 1.93 (1.56–2.37) | 2.33 (1.86–2.93) | 1.45 (0.97–2.15) |
| BMI at age 20 | |||||||
| Normal | 2.11 (1.73–2.57) | 2.09 (1.62–2.68) | 2.13 (1.69–2.70) | 1.93 (1.42–2.63) | 2.10 (1.64–2.68) | 2.39 (1.83–3.12) | 1.59 (1.00–2.53) |
| Overweight | 1.78 (1.23–2.58) | 1.59 (0.98–2.57) | 1.93 (1.24–3.00) | 1.58 (0.89–2.79) | 1.62 (1.02–2.58) | 2.30 (1.37–3.86) | 1.41 (0.57–3.50) |
| Obese | 0.69 (0.19–2.57) | 0.59 (0.10–3.56) | 0.90 (0.18–4.55) | 0.52 (0.06–4.35) | 0.45 (0.08–2.48) | 1.29 (0.21–7.80) | 0.19 (0.00–9.88) |
| Aspirin | |||||||
| Nonuser | 2.25 (1.80–2.83) | 2.25 (1.68–3.00) | 2.26 (1.73–2.95) | 1.89 (1.34–2.67) | 2.47 (1.86–3.28) | 2.49 (1.85–3.36) | 1.44 (0.84–2.49) |
| User | 1.67 (1.30–2.15) | 1.54 (1.12–2.13) | 1.79 (1.32–2.42) | 1.54 (1.03–2.30) | 1.41 (1.03–1.92) | 2.14 (1.51–3.04) | 1.47 (0.82–2.64) |
| Ibuprofen | |||||||
| Nonuser | 2.02 (1.68–2.42) | 1.99 (1.58–2.51) | 2.04 (1.64–2.53) | 1.86 (1.40–2.46) | 2.04 (1.63–2.56) | 2.25 (1.76–2.87) | 1.57 (1.03–2.39) |
| User | 1.75 (1.13–2.71) | 1.43 (0.83–2.49) | 2.05 (1.21–3.49) | 1.14 (0.57–2.26) | 1.34 (0.78–2.30) | 2.88 (1.56–5.33) | 0.75 (0.20–2.80) |
| Fruit intake | |||||||
| Tertile 1 | 2.04 (1.50–2.78) | 2.17 (1.45–3.26) | 1.94 (1.35–2.80) | 1.52 (0.96–2.42) | 2.16 (1.46–3.20) | 2.39 (1.58–3.63) | 1.20 (0.56–2.57) |
| Tertile 2 | 2.07 (1.54–2.80) | 1.86 (1.28–2.72) | 2.27 (1.59–3.23) | 2.17 (1.35–3.50) | 1.89 (1.31–2.72) | 2.53 (1.69–3.80) | 1.82 (0.92–3.60) |
| Tertile 3 | 1.76 (1.30–2.38) | 1.73 (1.19–2.50) | 1.78 (1.24–2.56) | 1.54 (0.97–2.45) | 1.80 (1.25–2.59) | 2.06 (1.35–3.13) | 1.19 (0.58–2.43) |
| Vegetable intake | |||||||
| Tertile 1 | 1.97 (1.46–2.66) | 2.23 (1.53–3.25) | 1.76 (1.23–2.51) | 1.34 (0.86–2.09) | 2.18 (1.52–3.13) | 2.39 (1.58–3.63) | 0.78 (0.38–1.59) |
| Tertile 2 | 1.92 (1.43–2.60) | 1.67 (1.14–2.44) | 2.16 (1.51–3.09) | 1.82 (1.15–2.87) | 1.76 (1.22–2.55) | 2.47 (1.63–3.73) | 1.64 (0.83–3.24) |
| Tertile 3 | 1.94 (1.43–2.64) | 1.81 (1.23–2.67) | 2.09 (1.44–3.02) | 2.30 (1.37–3.84) | 1.84 (1.25–2.70) | 2.07 (1.38–3.11) | 2.51 (1.11–5.67) |
| Vitamin D intake | |||||||
| Tertile 1 | 1.72 (1.26–2.34) | 1.62 (1.08–2.41) | 1.78 (1.24–2.55) | 1.46 (0.90–2.37) | 1.60 (1.08–2.36) | 2.20 (1.46–3.31) | 0.98 (0.45–2.15) |
| Tertile 2 | 1.91 (1.42–2.56) | 1.80 (1.25–2.60) | 2.02 (1.43–2.87) | 1.66 (1.08–2.57) | 1.92 (1.34–2.75) | 2.02 (1.36–3.00) | 1.99 (1.05–3.78) |
| Tertile 3 | 2.26 (1.67–3.07) | 2.34 (1.60–3.42) | 2.20 (1.52–3.20) | 2.11 (1.29–3.43) | 2.27 (1.58–3.26) | 2.81 (1.81–4.36) | 1.18 (0.55–2.56) |
| Folate intake | |||||||
| Tertile 1 | 1.99 (1.47–2.70) | 1.95 (1.31–2.90) | 2.02 (1.41–2.88) | 1.72 (1.08–2.75) | 1.89 (1.29–2.77) | 2.30 (1.54–3.43) | 1.36 (0.62–3.00) |
| Tertile 2 | 1.61 (1.19–2.16) | 1.54 (1.06–2.23) | 1.69 (1.18–2.40) | 1.36 (0.88–2.12) | 1.56 (1.08–2.24) | 1.91 (1.26–2.87) | 1.42 (0.74–2.70) |
| Tertile 3 | 2.38 (1.75–3.23) | 2.39 (1.63–3.48) | 2.40 (1.65–3.50) | 2.37 (1.44–3.91) | 2.53 (1.74–3.67) | 2.88 (1.87–4.44) | 1.47 (0.70–3.06) |
| Lycopene intake | |||||||
| Tertile 1 | 2.14 (1.58–2.92) | 2.36 (1.57–3.53) | 1.99 (1.40–2.84) | 1.60 (1.01–2.55) | 2.39 (1.62–3.52) | 2.41 (1.61–3.62) | 0.99 (0.47–2.05) |
| Tertile 2 | 1.95 (1.45–2.63) | 1.94 (1.34–2.80) | 1.97 (1.37–2.81) | 1.53 (0.97–2.40) | 1.86 (1.30–2.66) | 2.38 (1.57–3.61) | 1.78 (0.85–3.70) |
| Tertile 3 | 1.74 (1.29–2.36) | 1.50 (1.03–2.19) | 2.00 (1.38–2.88) | 2.04 (1.25–3.34) | 1.60 (1.11–2.32) | 2.11 (1.39–3.20) | 1.60 (0.79–3.26) |
| Selenium supplement | |||||||
| Nonuser | 2.01 (1.68–2.40) | 1.94 (1.55–2.43) | 2.06 (1.67–2.55) | 1.79 (1.37–2.36) | 1.97 (1.59–2.45) | 2.35 (1.85–3.00) | 1.54 (1.01–2.36) |
| User | 0.86 (0.33–2.25) | 0.94 (0.29–3.08) | 0.84 (0.24–2.88) | 0.54 (0.08–3.53) | 0.84 (0.25–2.82) | 1.17 (0.30–4.64) | 0.36 (0.03–4.05) |
NOTE: Results are shown when Pinteraction ≤ 0.15 (Supplementary Table S2). Results with Pinteraction < 0.05 are shown in bold font.
Effect modification (Pinteraction < 0.05) of the association between higher genetic risk score (≥12 risk alleles) and prostate cancer risk was observed for aspirin use, ibuprofen use, vegetable intake, and selenium supplement use (Table 2 and Supplementary Table S2). Selenium supplement use was the only environmental factor that we evaluated that statistically significantly modified the higher genetic risk of advanced-stage disease: among nonusers of selenium supplements, higher genetic risk score was more strongly associated with risk of total (Pinteraction = 0.033) and advanced-stage (Pinteraction = 0.031) prostate cancer, whereas in users of selenium supplements, these associations were all null. Aspirin and ibuprofen use, and vegetable intake modified the risk of nonadvanced-stage and low-grade disease only. Among men who did not use aspirin, we observed a stronger association between higher genetic risk and total (Pinteraction = 0.028), nonadvanced-stage (Pinteraction = 0.009), and low-grade (Pinteraction = 0.0008) prostate cancer, whereas these associations were attenuated among men who used aspirin (Table 2 and Supplementary Table S2). Among men who did not use ibuprofen, we observed a stronger association between higher genetic risk and nonadvanced-stage (Pinteraction = 0.023), and low-grade (Pinteraction = 0.008) disease; whereas these associations were attenuated in ibuprofen users (Table 2 and Supplementary Table S2). Among men with low vegetable intake (lowest tertile), higher genetic risk was more strongly associated with risk of nonadvanced-stage (Pinteraction = 0.010) and low-grade (Pinteraction = 0.014) disease, whereas in men who consumed more vegetables (middle and highest tertiles), these associations were attenuated. Possible effect modification was observed by intake of fruit, vegetables, folate, and lycopene (Table 2 and Supplementary Table S2), but the interactions were less robust (0.05 < Pinteraction ≤0.15) and patterns were not as clear or were inconsistent across strata of the effect modifier or prostate cancer features. Possible effect modification was present by BMI at the age of 20 years (Table 2 and Supplementary Table S2). However, the interactions were not statistically significant and the association for higher genetic risk score was reduced in men who were overweight and obese at the age of 20 years (nonadvanced-stage prostate cancer: overweight/obese–OR = 1.50, 95% CI, 0.94–2.37, normal –OR= 2.09, 95% CI, 1.62–2.68; Pinteraction = 0.28; advanced-stage prostate cancer: overweight/obese – OR = 1.82, 95% CI, 1.19–2.78, normal – OR = 2.13, 95% CI, 1.69–2.70; Pinteraction = 0.61), which would not be an appropriate preventive strategy.
We next evaluated the joint associations for higher genetic risk score and use of a selenium supplement, aspirin, ibuprofen, and vegetable intake with advanced or nonadvanced-stage prostate cancer (Table 3). Men with ≥12 risk alleles and who used a selenium supplement had a similar risk to men with <12 risk alleles and who did not use a selenium supplement. In contrast, among men with <12 risk alleles, those who used a selenium supplement appeared to have an increased risk of advanced-stage disease, although this association was not statistically significant (Table 3). Among men with <12 risk alleles, using aspirin or ibuprofen or eating more vegetables did not appear to attenuate the genetic risk of nonadvanced-stage disease. However, among men with ≥ 12 risk alleles, the genetic risk of nonadvanced disease was attenuated with aspirin or ibuprofen use and eating more vegetables. Despite this attenuation, the risk of nonadvanced-stage disease was still approximately 70% higher than in men with < 12 risk alleles who did not use aspirin or ibuprofen and ate fewer vegetables.
Table 3.
Joint association of higher genetic risk score (≥12 risk alleles) and environmental factors with advanced- and nonadvanced-stage prostate cancer adjusted for age and education, PLCO
| OR (95% CI)
|
||
|---|---|---|
| <12 risk alleles | ≥12 risk alleles | |
| Advanced-stage prostate cancer | ||
| Overall | 1.00 (ref.) | 2.04 (1.67–2.49) |
| Selenium supplement | ||
| Nonuser | 1.00 (ref.) | 2.06 (1.67–2.55) |
| User | 1.43 (0.70–2.96) | 0.99 (0.38–2.58) |
| Pinteraction = 0.031 | ||
| Nonadvanced-stage prostate cancer | ||
| Overall | 1.00 (ref.) | 1.91 (1.54–2.36) |
| Aspirin | ||
| Nonuser | 1.00 (ref.) | 2.25 (1.69–3.00) |
| User | 1.10 (0.80–1.51) | 1.70 (1.25–2.32) |
| Pinteraction = 0.009 | ||
| Ibuprofen | ||
| Nonuser | 1.00 (ref.) | 1.99 (1.58–2.52) |
| User | 1.10 (0.71–1.68) | 1.62 (1.07–2.45) |
| Pinteraction = 0.023 | ||
| Vegetable intake | ||
| Tertile 1 | 1.00 (ref.) | 2.24 (1.54–3.25) |
| Tertile 2 | 1.05 (0.71–1.56) | 1.76 (1.20–2.58) |
| Tertile 3 | 0.95 (0.64–1.42) | 1.71 (1.16–2.52) |
| Pinteraction = 0.010 | ||
NOTE: Results are shown when Pinteraction < 0.05 (Supplementary Table S2).
Finally, we evaluated the pattern of effect modification for aspirin and selenium across the range of genetic risk scores using 12 risk alleles in the unexposed as the reference. Figure 1 shows joint associations for categories of number of risk alleles and aspirin use: the increased risk of nonadvanced-stage prostate cancer associated with carrying 13 risk alleles or ≥14 risk alleles was attenuated in aspirin users; however, the association between carrying ≤ 9 risk alleles and nonadvanced disease was less inverse among aspirin users. The increased risk of advanced-stage disease associated with carrying ≥ 13 risk alleles appeared to be attenuated in selenium supplement users (OR = 0.69, 95% CI, 0.09–5.51; nonusers: OR = 1.45, 95% CI, 1.06–1.98); however, the inverse association between carrying ≤11 risk alleles and advanced-stage disease was null in selenium supplement users (OR = 0.92, 95% CI, 0.14–6.08; nonusers OR = 0.63, 95% CI, 0.46–0.84).
Figure 1.
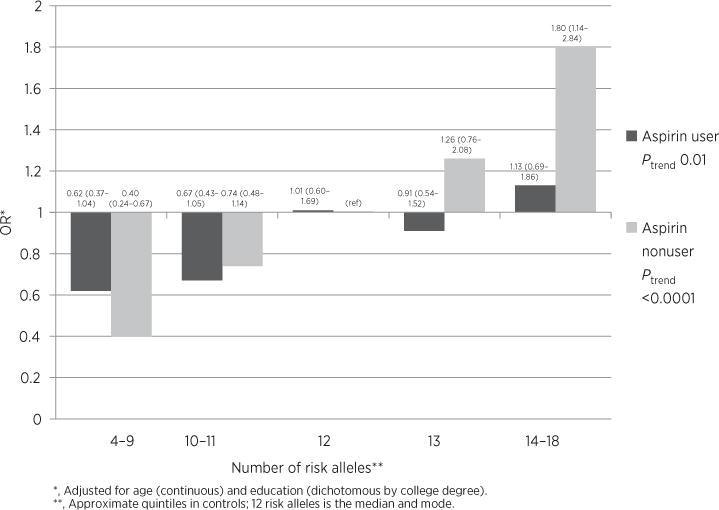
OR of nonadvanced prostate cancer for joint categories of number of risk alleles and aspirin use, PLCO. ORs are adjusted for age (continuous) and education (dichotomous by college degree). The categories for number of risk alleles are approximate quintiles in controls. The median and mode are both 12 risk alleles in the controls.
Discussion
In this prospective study evaluating 20 SNPs that were previously associated with prostate cancer susceptibility, we observed that selenium supplement use may reduce the genetic risk of advanced-stage prostate cancer and that aspirin and ibuprofen use and vegetable intake may reduce the genetic risk of nonadvanced-stage and low-grade prostate cancer. Although based on data from one cohort only, our results may help inform the testing of strategies for prevention among those at higher genetic risk.
To date, only a few preventive interventions have been evaluated in a randomized, prospective fashion. 5-α reductase inhibitors (5ARI’s) were shown to decrease the incidence of biopsy-detectable prostate cancer (25, 26). However, they lead to sexual side effects and their use for prostate cancer prevention was rejected by the FDA due to an absolute increase in the incidence of high-grade prostate cancer (27). Epidemiologic studies have also suggested a protective relationship between many other modifiable factors with prostate cancer risk, but they have not been validated or cannot be practically tested in randomized trials (6). Moreover, relatively little research has been conducted on gene–environment interactions and prostate cancer risk. Thus, the goal of our study was to specifically evaluate whether environmental factors that men have some control over may reduce or eliminate the genetic risk of prostate cancer, especially aggressive disease.
Among men with a high genetic risk profile, we found that selenium supplement use may attenuate the risk of advanced-stage disease, whereas aspirin, ibuprofen, and higher vegetable intake may attenuate the risk of nonadvanced-stage disease. Some studies support that higher selenium intake, especially from a supplement, may reduce prostate cancer risk, (28) including the Nutritional Prevention of Cancer (NPC) Study. In that study, the reduction in risk association with selenium supplementation was limited to men with low circulating selenium levels at baseline (29). In a nested case–control study in the PLCO, the same cohort in which the current study was done, no statistically significant association between serum selenium levels and the incidence of total or advanced prostate cancer was found, although higher serum levels were inversely associated with prostate cancer in smokers and men with highest total intake of Vitamin E (16). Ultimately, a randomized placebo controlled trial called the Selenium and Vitamin E Cancer Prevention Trial (SELECT) reported no significant reduction in prostate cancer risk using selenium alone or in combination with vitamin E, and even potential harm (30). It remains to be studied whether selenium supplementation is inversely associated with prostate cancer among men at higher genetic risk within the NPC and SELECT trials.
Many observational studies support that aspirin and ibuprofen use are associated with a modest reduction in prostate cancer risk (7). In the PLCO, daily aspirin use was modestly inversely associated with prostate cancer risk, but ibuprofen use was not (8). It is unclear whether the inverse association between aspirin and prostate cancer risk reflects a true reduction in risk or a complex detection bias related to the effects of aspirin on serum PSA levels (31). Either way, a reduction in biopsy-detectable nonaggressive prostate cancer could have important public health consequences, including a reduction in the overdetection of prostate cancer that may never cause morbidity or premature mortality. Nevertheless, the potential benefit of aspirin in men with the higher genetic risk profile must be weighed against the risks of aspirin use. The United States Preventive Services Task Force (USPSTF) recommends against the routine use of aspirin or nonsteroidal anti-inflammatory drugs to prevent colorectal cancer, indicating that potential harms such as bleeding outweigh the preventative benefits in average-risk men (32). On the other hand, the USPSTF recommends aspirin in men ages 45 to 79 years for the prevention of heart attack, if the potential benefit outweighs the potential harm of gastrointestinal bleeding (33). In light of the potential harms of aspirin and other NSAIDs, they would likely not be a viable preventive strategy for prostate cancer in average-risk men. However, our results suggest that the risk to benefit ratio may shift for men with a higher genetic risk profile.
Finally, we found that higher vegetable intake may also modify the higher genetic risk of nonaggressive prostate cancer. Aside from tomatoes and possibly broccoli, there is limited evidence that vegetable intake protects against prostate cancer risk (6, 34, 35). In the PLCO, intake of broccoli and other cruciferous vegetables was associated with a lower risk of aggressive prostate cancer (36). The benefits of vegetable consumption are numerous for good health in general, so while it is possible that some men could benefit from vegetable intake more than others with respect to prostate cancer, promoting vegetable consumption by all men irrespective of genetic risk is sound public health advice.
A strength of this study is the robust dataset, including environmental factors and genotypes, allowing a comprehensive examination of their interactions. The findings from our study have importance as we move toward an era of personalized medicine, and for the design of future intervention studies. Another strength of the study is that food frequency questionnaires were administered at baseline, eliminating the possibility of biased recall following prostate cancer diagnosis. All participants were subjected to a uniform screening protocol within the PLCO trial and were thus afforded a similar opportunity for prostate cancer detection. Because prostate cancer was one of the target cancers in the PLCO, follow-up for the diagnosis of prostate cancer was complete and detailed data were collected on tumor features, enabling a separate evaluation of aggressive and nonag-gressive disease.
Several limitations of our study deserve mention including chance findings from the evaluation of interaction of the genetic risk score with numerous lifestyle variables. For advanced-stage and nonadvanced-stage disease, in total we evaluated 48 interactions; neither the aspirin (P = 0.009) nor the selenium (P = 0.031) interactions with the genetic risk score would have been considered to be statistically significant at the 0.05/48 = 0.001 level. In addition, many of the SNPs have no known function, and therefore the mechanism for effect modification by environmental factors is unclear. Some of the SNPs are associated with the serum PSA concentration (including rs10993994 on chromosome 10, as well as rs2659056 and rs2735839 on chromosome 19), raising the possibility of a detection bias (37, 38). As such, it is not possible to distinguish whether our observed findings reflect a true reduction in the risk of developing prostate cancer or simply a reduction in the detectability of prostate cancer associated with the genetic risk score. Nevertheless, even a reduction in the detectability of nonaggressive cancers could represent an important public health benefit, given current concerns with overdiagnosis and overtreatment.
Another important limitation is that our study only included non–Hispanic white male participants from the PLCO screening trial, and therefore it is unclear whether the findings are generalizable to other racial/ethnic groups or cases that present in other ways. Moreover, many new genetic variants have been identified since the original genotyping was performed in PLCO (the data used in the current analysis; ref. 2). Also, our study focused on a limited number of preselected possible effect modifiers assessed by questionnaire. As such, future studies are necessary to further examine many other potential gene–environment interactions outside the scope of the current study. Finally, the results of this study are observational in nature, and therefore it is not possible to determine whether modification of these environmental exposures would ultimately decrease the risk of prostate cancer development or detection.
In conclusion, because personalized genomic testing is now available, there is an urgent need for further study on gene–environment interactions and the identification and testing of preventive strategies for men at higher genetic risk for prostate cancer. Our results from this prospective study nested in the PLCO suggest that selenium supplement use may reduce the genetic risk of advanced-stage prostate cancer and that aspirin, ibuprofen, and vegetable intake may attenuate the genetic risk of nonadvanced-stage and low-grade prostate cancer.
Supplementary Material
Impact.
The effect of genetic factors on prostate cancer risk may vary by lifestyle interventions.
Acknowledgments
Grant Support
This work was supported by P50 CA58236 (to W.G. Nelson) from the National Cancer Institute, NIH, Department of Health and Human Services, and by K07 CA178258 from the National Cancer Institute, NIH, Department of Health and Human Services (to S. Loeb). This work was also supported by the Louis Feil Charitable Lead Trust to S. Loeb.
Footnotes
Note: Supplementary data for this article are available at Cancer Epidemiology, Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
Disclosure of Potential Conflicts of Interest
S. Loeb has received speakers’ bureau honoraria from Sanofi IGUCC meeting and Bayer lecture at Colombian Urologic. No potential conflicts of interest were disclosed by the other authors.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Authors’ Contributions
Conception and design: S. Loeb, W.-Y. Huang, E.A. Platz, H.B. Carter
Development of methodology: S. Loeb
Acquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): W.-Y. Huang, R.B. Hayes
Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): S. Loeb, S.B. Peskoe, W.-Y. Huang, W.B. Isaacs, E.A. Platz, H.B. Carter
Writing, review, and/or revision of the manuscript: S. Loeb, S.B. Peskoe, C.E. Joshu, W.-Y. Huang, R.B. Hayes, E.A. Platz, H.B. Carter
Study supervision: S. Loeb, E.A. Platz
References
- 1.Thomas G, Jacobs KB, Yeager M, Kraft P, Wacholder S, Orr N, et al. Multiple loci identified in a genome-wide association study of prostate cancer. Nat Genet. 2008;40:310–5. doi: 10.1038/ng.91. [DOI] [PubMed] [Google Scholar]
- 2.Eeles RA, Olama AA, Benlloch S, Saunders EJ, Leongamornlert DA, Tym-rakiewicz M, et al. Identification of 23 new prostate cancer susceptibility loci using the iCOGS custom genotyping array. Nat Genet. 2013;45:385–91. 91e1–2. doi: 10.1038/ng.2560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kader AK, Sun J, Reck BH, Newcombe PJ, Kim ST, Hsu FC, et al. Potential impact of adding genetic markers to clinical parameters in predicting prostate biopsy outcomes in men following an initial negative biopsy: findings from the REDUCE trial. Eur Urol. 2012;62:953–61. doi: 10.1016/j.eururo.2012.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zheng SL, Sun J, Wiklund F, Smith S, Stattin P, Li G, et al. Cumulative association of five genetic variants with prostate cancer. N Engl J Med. 2008;358:910–9. doi: 10.1056/NEJMoa075819. [DOI] [PubMed] [Google Scholar]
- 5.Nordstrom T, Aly M, Eklund M, Egevad L, Gronberg H. A genetic score can identify men at high risk for prostate cancer among men with prostate-specific antigen of 1–3 ng/ml. Eur Urol. 2014;65:1184–90. doi: 10.1016/j.eururo.2013.07.005. [DOI] [PubMed] [Google Scholar]
- 6.World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. Washington, DC: 2007. [Google Scholar]
- 7.Mahmud SM, Franco EL, Aprikian AG. Use of nonsteroidal anti-inflammatory drugs and prostate cancer risk: a meta-analysis. Int J Cancer. 2010;127:1680–91. doi: 10.1002/ijc.25186. [DOI] [PubMed] [Google Scholar]
- 8.Shebl FM, Sakoda LC, Black A, Koshiol J, Andriole GL, Grubb R, et al. Aspirin but not ibuprofen use is associated with reduced risk of prostate cancer: a PLCO study. Br J Cancer. 2012;107:207–14. doi: 10.1038/bjc.2012.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, et al. Environmental and heritable factors in the causation of cancer– analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343:78–85. doi: 10.1056/NEJM200007133430201. [DOI] [PubMed] [Google Scholar]
- 10.Cook LS, Goldoft M, Schwartz SM, Weiss NS. Incidence of adenocarcinoma of the prostate in Asian immigrants to the United States and their descendants. J Urol. 1999;161:152–5. [PubMed] [Google Scholar]
- 11.[Accessed July 2, 2013]. Available from: https://www.23andme.com/health/Prostate-Cancer/.
- 12.Accessed January 8, 2014]. Available from: http://www.fda.gov/iceci/enforcementactions/warningletters/2013/ucm376296.htm.
- 13.McGuire AL, Burke W. An unwelcome side effect of direct-to-consumer personal genome testing: raiding the medical commons. JAMA. 2008;300:2669–71. doi: 10.1001/jama.2008.803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andriole GL, Crawford ED, Grubb RL, III, Buys SS, Chia D, Church TR, et al. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: mortality results after 13 years of follow-up. J Natl Cancer Inst. 2012;104:125–32. doi: 10.1093/jnci/djr500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shikany JM, Flood AP, Kitahara CM, Hsing AW, Meyer TE, Willcox BJ, et al. Dietary carbohydrate, glycemic index, glycemic load, and risk of prostate cancer in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO) cohort. Cancer Causes Control. 2011;22:995–1002. doi: 10.1007/s10552-011-9772-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peters U, Foster CB, Chatterjee N, Schatzkin A, Reding D, Andriole GL, et al. Serum selenium and risk of prostate cancer-a nestedcase-control study. Am J Clin Nutr. 2007;85:209–17. doi: 10.1093/ajcn/85.1.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.The Health Consequences of Smoking- 50 Years of Progress. A Report of the Surgeon General. Accessed September 23, 2014]. Available from: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf. [PubMed]
- 18.Eeles RA, Kote-Jarai Z, Giles GG, Olama AA, Guy M, Jugurnauth SK, et al. Multiple newly identified loci associated with prostate cancer susceptibility. Nat Genet. 2008;40:316–21. doi: 10.1038/ng.90. [DOI] [PubMed] [Google Scholar]
- 19.Gudmundsson J, Sulem P, Rafnar T, Bergthorsson JT, Manolescu A, Gudbjartsson D, et al. Common sequence variants on 2p15 and Xp11.22 confer susceptibility to prostate cancer. Nat Genet. 2008;40:281–3. doi: 10.1038/ng.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Duggan D, Zheng SL, Knowlton M, Benitez D, Dimitrov L, Wiklund F, et al. Two genome-wide association studies of aggressive prostate cancer implicate putative prostate tumor suppressor gene DAB2IP. J Natl Cancer Inst. 2007;99:1836–44. doi: 10.1093/jnci/djm250. [DOI] [PubMed] [Google Scholar]
- 21.Sun J, Zheng SL, Wiklund F, Isaacs SD, Li G, Wiley KE, et al. Sequence variants at 22q13 are associated with prostate cancer risk. Cancer Res. 2009;69:10–5. doi: 10.1158/0008-5472.CAN-08-3464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sun J, Zheng SL, Wiklund F, Isaacs SD, Purcell LD, Gao Z, et al. Evidence for two independent prostate cancer risk-associated loci in the HNF1B gene at 17q12. Nat Genet. 2008;40:1153–5. doi: 10.1038/ng.214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Amundadottir LT, Sulem P, Gudmundsson J, Helgason A, Baker A, Agnars-son BA, et al. A common variant associated with prostate cancer in European and African populations. Nat Genet. 2006;38:652–8. doi: 10.1038/ng1808. [DOI] [PubMed] [Google Scholar]
- 24.Gudmundsson J, Sulem P, Manolescu A, Amundadottir LT, Gudbjartsson D, Helgason A, et al. Genome-wide association study identifies a second prostate cancer susceptibility variant at 8q24. Nat Genet. 2007;39:631–7. doi: 10.1038/ng1999. [DOI] [PubMed] [Google Scholar]
- 25.Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349:215–24. doi: 10.1056/NEJMoa030660. [DOI] [PubMed] [Google Scholar]
- 26.Andriole GL, Bostwick DG, Brawley OW, Gomella LG, Marberger M, Montorsi F, et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010;362:1192–202. doi: 10.1056/NEJMoa0908127. [DOI] [PubMed] [Google Scholar]
- 27.Theoret MR, Ning YM, Zhang JJ, Justice R, Keegan P, Pazdur R. The risks and benefits of 5alpha-reductase inhibitors for prostate-cancer prevention. N Engl J Med. 2011;365:97–9. doi: 10.1056/NEJMp1106783. [DOI] [PubMed] [Google Scholar]
- 28.Clark LC, Combs GF, Jr, Turnbull BW, Slate EH, Chalker DK, Chow J, et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional Prevention of Cancer Study Group. JAMA. 1996;276:1957–63. [PubMed] [Google Scholar]
- 29.Duffield-Lillico AJ, Dalkin BL, Reid ME, Turnbull BW, Slate EH, Jacobs ET, et al. Selenium supplementation, baseline plasma selenium status and incidence of prostate cancer: an analysis of the complete treatment period of the Nutritional Prevention of Cancer Trial. BJU Int. 2003;91:608–12. doi: 10.1046/j.1464-410x.2003.04167.x. [DOI] [PubMed] [Google Scholar]
- 30.Klein EA, Thompson IM, Jr, Tangen CM, Crowley JJ, Lucia MS, Goodman PJ, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT) JAMA. 2011;306:1549–56. doi: 10.1001/jama.2011.1437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singer EA, Palapattu GS, van Wijngaarden E. Prostate-specific antigen levels in relation to consumption of nonsteroidal anti-inflammatory drugs and acetaminophen: results from the 2001–2002 National Health and Nutrition Examination Survey. Cancer. 2008;113:2053–7. doi: 10.1002/cncr.23806. [DOI] [PubMed] [Google Scholar]
- 32.Routine aspirin or nonsteroidal anti-inflammatory drugs for the primary prevention of colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2007;146:361–4. [PubMed] [Google Scholar]
- 33.U.S. Preventive Services Task Force (USPSTF) Recommendations on Aspirin for the Prevention of Cardiovascular Disease. [Accessed September 30, 2013]. Available from: http://www.uspreventiveservicestaskforce.org/uspstf/uspsasmi.htm.
- 34.Kristal AR, Lampe JW. Brassica vegetables and prostate cancer risk: a review of the epidemiological evidence. Nutr Cancer. 2002;42:1–9. doi: 10.1207/S15327914NC421_1. [DOI] [PubMed] [Google Scholar]
- 35.Giovannucci E, Rimm EB, Liu Y, Stampfer MJ, Willett WC. A prospective study of cruciferous vegetables and prostate cancer. Cancer Epidemiol Biomarkers Prev. 2003;12:1403–9. [PubMed] [Google Scholar]
- 36.Kirsh VA, Peters U, Mayne ST, Subar AF, Chatterjee N, Johnson CC, et al. Prospective study of fruit and vegetable intake and risk of prostate cancer. J Natl Cancer Inst. 2007;99:1200–9. doi: 10.1093/jnci/djm065. [DOI] [PubMed] [Google Scholar]
- 37.Loeb S, Carter HB, Walsh PC, Isaacs WB, Kettermann A, Tanaka T, et al. Single nucleotide polymorphisms and the likelihood of prostate cancer at a given prostate specific antigen level. J Urol. 2009;182:101–4. doi: 10.1016/j.juro.2009.02.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ahn J, Berndt SI, Wacholder S, Kraft P, Kibel AS, Yeager M, et al. Variation in KLK genes, prostate-specific antigen and risk of prostate cancer. Nat Genet. 2008;40:1032–4. doi: 10.1038/ng0908-1032. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.