

Highlights
-
•
Pancreatic hydatid cyst is rarely reported.
-
•
Due to its rarity and similarity with more common pancreatic cystic conditions, diagnosis of pancreatic may be a challenging.
-
•
Past history of travelling to endemic ares should raise suspiscion to the possibility of hydatid disease.
Keywords: Pancreas, Hydatid cyst
Abstract
INTRODUCTION
Hydatid disease is a parasitic infestation caused by the cystic stage of Echinococcus granulosus. Hydatid cysts are commonly located in the liver and lung. Pancreatic affection by hydatid cysts is very rare even in endemic areas.
PRESENTATION OF CASE
Our case is a 34-year-old male patient referred to our centre with a pancreatic body cyst diagnosed by abdominal CT scan. The patient gave 3 months history of epigastric pain. He also gave history of travelling to Saudi Arabia and China. His enzyme-linked immunoadsorbent assay (ELIZA) test for echinococcal antigens was positive. Surgical exploration revealed a 7 cm cyst in the body of the pancreas separable from the surroundings. Endocystectomy and deroofing of the cyst was done.
DISCUSSION
Due to its rarity and similarity with more common pancreatic cystic conditions, diagnosis of pancreatic hydatid cyst may be challenging. Abdmonial sonography and CT scan together with enzyme-linked immunoadsorbent assay (ELIZA) test for echinococcal antigens are helpful diagnostic tools. Therapeutic options include endocystectomy and deroofing, albendazol therapy with percutaneous drainage or laparoscopic excision of the cyst.
CONCLUSION
Even in non-endemic areas, past history of travelling abroad in patients with pancreatic cystic lesions should raise the suspicion of hydatid disease as a possible diagnosis.
1. Introduction
Hydatid disease is a parasitic infestation caused by the cystic stage of Echinococcus granulosus. As the definitive hosts are dogs and other carnivores while the intermediate hosts are sheep and cattle, the disease is frequently reported in cattle raising countries as the Middle East, India, Australia and Turkey.1
Hydatid cysts are commonly located in the liver and lung and less commonly in the kidney, bone and brain.2 Pancreatic affection by hydatid cysts is very rare even in endemic areas.3
For pancreas, the head is more frequently involved (57%) followed by the body (24%) and the tail (19%).4
2. Case report
A 34-year-old male patient was referred to our outpatient clinic at Gastroenterology Surgical Centre, Mansoura University with accidentally discovered pancreatic body cyst as the patient was investigated for epigastric pain 3 months before. He gave no history of vomiting, jaundice, fever or weight loss. On examination, the patient was conscious, well oriented. Abdominal examination revealed no tenderness, swellings or organomegally. Apart from controlled hypertension, the past medical and surgical histories were irrelevant; however, the patient gave history for travelling to Saudi Arabia and China.
Abdominal triphasic CT scan revealed a well-defined thick-walled marginally enhancing cystic lesion in the body of the pancreas measuring 7 cm × 4.5 cm with no detected solid nodules or calcifications, mostly hydatid cyst. The surrounding fat planes were normal and no detectable structural abnormalities in the main pancreatic duct (Fig. 1).
Fig. 1.

Abdominal CT scan showing a well-defined thick-walled cystic lesion in the body of the pancreas.
Flexible oesophago-gastro-duodenoscopy showed antral gastritis and mild duodenitis.
Pre-operative laboratory investigations including complete blood picture, liver function tests and serum amylase were within normal ranges. Enzyme-linked immunoadsorbent assay (ELIZA) test for echinococcal antigens was positive.
Laparotomy was done through a left subcostal incision with upper midline extension. Exploration revealed a 7 cm cyst in the body of the pancreas separable from the surrounding structures (Fig. 2). Isolation of the cyst with towels impregnated with hypertonic saline (20%) was done. After aspiration of the fluid content and injection with hypertonic saline (20%), endocystectomy and deroofing (Fig. 3). A drain was left in the resultant cavity.
Fig. 2.
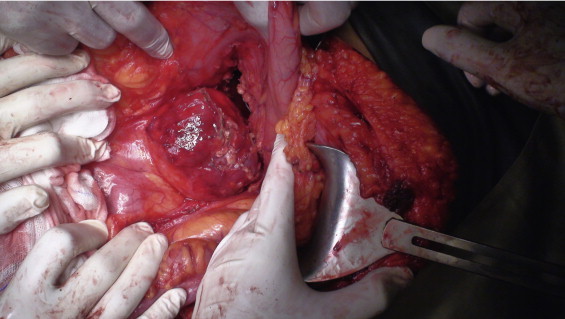
Operative photo showing the pancreatic body cyst after opening of the lesser sac.
Fig. 3.
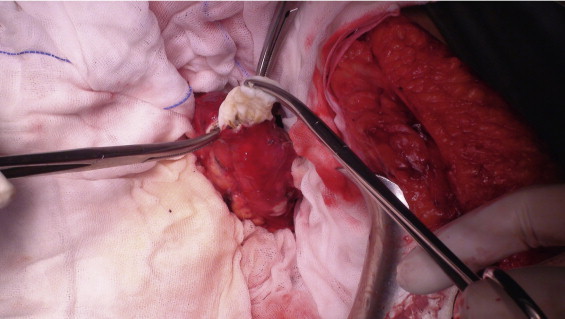
Operative photo after opening of the cyst and extraction of the hydatid membranes.
The patient passed an eventless postoperative course and was discharged on the third postoperative day on oral albendazole therapy.
3. Discussion
Due to its rarity and similarity with more common pancreatic cystic conditions, diagnosis of pancreatic hydatid cyst may be challenging.5
As in most cases, hydatid cysts are usually asymptomatic; however, the patients may complain of abdominal pain, vomting or complications as obstructive jaundice or acute pancreatitis. Past history of travelling or immigration should make physicians aware of the possibility of hydatid disease even in non-endemic areas.6
Enzyme-linked immunoadsorbent assay (ELIZA) test for echinococcal antigens is a helpful tool with an overall specificity of about 85%.4
Abdominal sonography is considered the most sensitive tool detecting the floating membranes, hydatid sand and floating daughter cysts. Water lily sign, water attenuation and calcifications detected by CT scanning are also highly suggestive of hydatid cyst.7
Although the above-mentioned investigations help in the diagnosis of hydatid cyst and its differentiation from other cystic lesions of the pancreas, surgery remains the only definitive diagnostic and therapeutic tool.4,7
Several surgical techniques have been described for the management of pancreatic hydatid cysts according to its location in the pancreas. In our case, as the cyst was located in the pancreatic body we did endocystectomy, deroofing and drainage of the resultant cavity.8
Other treatment options include albendazole therapy with percutaneous drainage3 and laparoscopic excision of the cyst.9
We conclude that even in non-endemic areas, past history of travelling abroad in patients with pancreatic cystic lesions should raise the suspicion of hydatid disease as a possible diagnosis. As to our knowledge this is the first case of pancreatic hydatid cyst to be published from Egypt.
Conflict of interest
The authors declare that is no conflict of interest.
Funding
There is no external funding resources for the study.
Ethical approval
An approval from the hospital board comittee is taken for the procedure and case report publication.
Author contributions
Mohamed El Sorogy helped in the acquisition of data, or analysis and interpretation of data. Mohamed El Sorogy and Mohamed El-Hemaly contributed in drafting the article or revising it critically for important intellectual content. Ahmed Aboelenen helped in the final approval of the version to be submitted.
References
- 1.Sayek I., Onat D. Diagnosis and treatment of uncomplicated hydatid cyst of the liver. World J Surg. 2001;25:21–27. doi: 10.1007/s002680020004. [DOI] [PubMed] [Google Scholar]
- 2.Bedioui H., Chebbi F., Ayadi S., Daghfous A., Bakhtri M., Jouini M. Primary hydatid cyst of the pancreas: diagnosis and surgical procedures. Report of three cases. Gastroenterol Clin Biol. 2008;32:102–106. doi: 10.1016/j.gcb.2007.12.014. [DOI] [PubMed] [Google Scholar]
- 3.Jai S.R., El Hattabi K., Bensardi F., Chehab F., Khaiz D., Bouzidi A. Primary hydatid cyst of the pancreas causing obstructive jaundice. Saudi J Gastroenterol. 2007;13:191–193. doi: 10.4103/1319-3767.36752. [DOI] [PubMed] [Google Scholar]
- 4.Ousadden A., Elbouhaddouti H., Ibnmajdoub K.H., Mazaz K., Aittalebet K. Primary hydatid cyst of the pancreas with a hepatic pedicule compression. Cases J. 2009;2:201. doi: 10.1186/1757-1626-2-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dahniya M.H., Hanna R.M., Ashebu S., Muhtaseb S.A., El-Beltagi A., Badr S. The imaging appearances of hydatid disease at some unusual sites. Br J Radiol. 2001;74:283–289. doi: 10.1259/bjr.74.879.740283. [DOI] [PubMed] [Google Scholar]
- 6.Ozmen M.M., Moran M., Karakahya M., Coskun F. Recurrent acute pancreatitis due to a hydatid cyst of the pancreatic head: a case report and review of the literature. JOP J Pancreas. 2005;6:354–358. [online] [PubMed] [Google Scholar]
- 7.Masoodi I., Nabi G., Kumar R., Lone M.A., Khan B.A., Naseer Al Sayari K. Hydatid cyst of the pancreas: a case report and brief review. Turk J Gastroenterol. 2011;22(4):430–432. doi: 10.4318/tjg.2011.0259. [DOI] [PubMed] [Google Scholar]
- 8.Suryawanshi P., Khan A.Q., Jatal S. Primary hydatid cyst of pancreas with acute pancreatitis. Int J Surg Case Rep. 2011;2:122–124. doi: 10.1016/j.ijscr.2011.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Faraj W., Selmo F., Khalifeh M., Jamali F. Laparoscopic resection of pancreatic hydatid disease. Surgery. 2006;139:438–441. doi: 10.1016/j.surg.2005.10.004. [DOI] [PubMed] [Google Scholar]