

Abstract
Objectives
This study prospectively evaluated postthyroidectomy syndrome (PTS) through objective and subjective voice changes following thyroidectomy of open vs. endoscopic thyroidectomy.
Methods
A prospective clinical trial (SCHBC IRB 09 26) was performed from Jan 2008 to Aug 2010 to compare the open thyroidectomy (OPEN group) and endoscopic thyroidectomy (ENDO group). Of the 110 patients, 75 completed the evaluation before and 1 and 6 months after surgery. Subjective parameters included perceptual analysis (GRBAS [grade, roughness, breathiness, asthenia, and strain] scale), stroboscopic or flexible fiberscopic analysis, voice handicap index, and 5-point visual analog scales for vocal fatigue, singing difficulty, difficulty with high-pitch phonation, and neck discomfort. Objective parameters included acoustic, aerodynamic analysis and the electroglottograph.
Results
For the ENDO group (n=36), the operation time was longer than in the OPEN group (n=39; P<0.01). For the OPEN group, two objective and five subjective parameters were worse 1 month postoperatively; of these, two subjective parameters persisted for 6 months (P<0.05). For the ENDO group, three objective and six subjective parameters were worse 1 month postoperatively, and three of the subjective parameters persisted 6 months postoperatively (P<0.05).
Conclusion
PTS really exists following simple thyroidectomy and are very common for both OPEN and ENDO groups. Most of the parameters improved gradually over time, but some subjective changes persisted 6 months postoperatively.
Keywords: Thyroidectomy, Voice Quality, Postoperative Complications
INTRODUCTION
Many patients have suffered from unexplained discomforts after simple thyroidectomy, without evidence of recurrent laryngeal nerve (RLN) injury [1]. Typical symptoms are easy fatigue during phonation and difficulty with high-pitched and singing voices; other symptoms are paresthesia, vague voice changes, throat discomfort, swallowing difficulties, and the feeling of choking. This collection of symptoms appears to be a real syndrome, which we have named postthyroidectomy syndrome (PTS). Various causes of PTS have been suggested, including laryngotracheal fixation, direct injury of superior laryngeal nerve, and laryngeal lymph edema following thyroidectomy [2,3,4]. Among these causes, laryngotracheal fixation is the most suggested cause of PTS, however, the exact cause of PTS is not clear until now.
Although several papers on the operative outcomes of endoscopic and conventional thyroidectomy have reported, no prospective trials comparing the functional outcomes, including postoperative discomfort and voice changes, between patients undergoing endoscopic and conventional open thyroidectomy have been performed. This study prospectively evaluated PTS through objective and subjective voice parameters following thyroidectomy of conventional open thyroidectomy (OPEN) and endoscopic thyroidectomy (ENDO) groups.
MATERIALS AND METHODS
Patients
The initial study sample consisted of 110 ENDO group and OPEN group patients seen at the Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, between January 2008 and August 2010. This study was prospective observational study in single center and by a single surgeon (SWL).
All patients were explained about the operative techniques involved in OPEN and ENDO, and the patient subsequently chose which approach would be applied and be provided with written informed consent. This study protocol was approved by Institutional Review Board (SCHBC IRB 09 26).
The inclusion criteria of patients were benign thyroid tumor of 4 cm less in diameter or a papillary thyroid carcinoma 1.5 cm or less in diameter. The exclusion criteria were previous neck surgery; severe Graves disease; a malignancy with definite extrathyroidal extension, multiple lateral neck node metastasis, extracapsular spread of metastatic lymph node, or distant metastasis; a lesion located in the thyroid dorsal area (especially adjacent to the tracheoesophageal groove) because this may risk possible injury to the trachea, esophagus and RLN. Ultimately, 75 patients were enrolled in this study: 39 patients in the OPEN group (total thyroidectomy [TT]+central neck dissection [CND]) and 36 patients in the ENDO group (endoscopic TT+ipsilateral CND).
Surgical outcomes
We measured the maximum phonation time, jitter, shimmer, harmonics-to-noise ratio, maximum fundamental frequency (Max F0), mean fundamental frequency (Mean F0), minimum fundamental frequency, contact quotient of the electroglottograph, and stroboscopy or flexible fiberoscopy for objective parameters. For the subjective parameters, we also evaluated the GRBAS (grade, roughness, breathiness, asthenia, and strain) scales and the voice handicap index (VHI) as well as other scaled subjective voice parameters. The patients were asked (by questionnaire using 5-point visual analog scale [VAS]) to evaluate the presence of hyperesthesia and paresthesia in the neck before and 1 and 6 months after surgery. The 5-point VAS was also applied to evaluate the subjective voice function changes (easy vocal fatigue, singing difficulty, and difficulty with high-pitch phonation [0, normal; 5, worst]). Cosmetic results for healed wound appearance and complaints, were evaluated by the patients 6 months after surgery using a verbal response scale with five possible responses: extremely satisfied (0 point), excellent, acceptable, dissatisfied, and extremely dissatisfied (5 points).
To exclude other reasons of voice change, such as vocal cord paralysis, arytenoid dislocation, and preexisting voice disorders, we performed stroboscopic or fiberscopic examinations before and 1 and 6 months after surgery.
We defined the first postoperative month as the early postoperative period to exclude the effects of endotracheal intubation and vocal fold edema. And postoperative six months defined as the late postoperative period. The operation time was defined as the time from to skin incision to completion of total thyroidectomy with CND but time for the bleeding control and skin closure was not included.
Surgical procedures
In the OPEN group, a no-tie harmonic scalpel (CS-14C handpiece, Johnson & Johnson Medical, Cincinnati, OH, USA) thyroidectomy was performed. All the procedures including vascular control of the thyroid gland were completed with only harmonic scalpel without conventional hand-tied ligation [5].
In the ENDO group, total thyroidectomy with ipsilateral CND was performed with a gasless unilateral transaxillary approach (Fig. 1) [6]. A 5-cm skin incision was made parallel to a skin crease in the axillary fossa. The skin was elevated above the pectoralis major muscle under direct vision using Bovie electrocautery (Conmed Co., Utica, NY, USA) through the axillary skin incision.
Fig. 1.

The position of patient during endoscopic total thyroidectomy+ ipsilateral central neck dissection through a unilateral transaxillary approach.
To create a working space, an external retractor (Sejong Medical Co., Paju, Korea) was inserted through the skin incision in the axilla and raised using a lifting device. A second 1-cm skin incision was made along the upper margin of the mammary areola on the tumor side for insertion of a 10-mm trocar. We used the Harmonic Scalpel (Harmonic Ace 36P, Johnson & Johnson Medical) and an endoscopic dissector for vessel sealing and tissue dissection throughout the operation. For ipsilateral CND (the pretracheal and paratracheal lymph node on the tumor side), dissection was performed superficial to the RLN using an endoscopic dissector without the Harmonic Scalpel. The CND was performed separately after the thyroidectomy.
Statistical analysis
SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) were performed using the paired t-test, Student t-test, chi-square test, and Fisher exact test. P-values less than 0.05 were considered statistically significant.
RESULTS
Table 1 summarizes the demographic data for the OPEN and ENDO group. The ENDO group had showed better cosmetic results and a longer operating time than the OPEN group (P<0.01). Thyroidectomy-related discomforts occurred in 64.1% of the OPEN group and 75.0% of the ENDO group patients, although the difference in incidence between groups was not significant (P>0.05). The existence of thyroidectomy-related discomforts such as vocal fatigue, high pitch singing and neck discomfort were not correlated with the operative technique (OPEN vs. ENDO), tumor size (small vs. large), tumor T stage (early vs. advanced), multiplicity of tumors (single vs. multiple), or radioactive iodide therapy (P>0.05). The cutoff value between small and large tumors was 1 cm in size; early and advanced T stage were divided as stage I and II vs. III and IV, respectively.
Table 1.
Patient demographics (n=75)
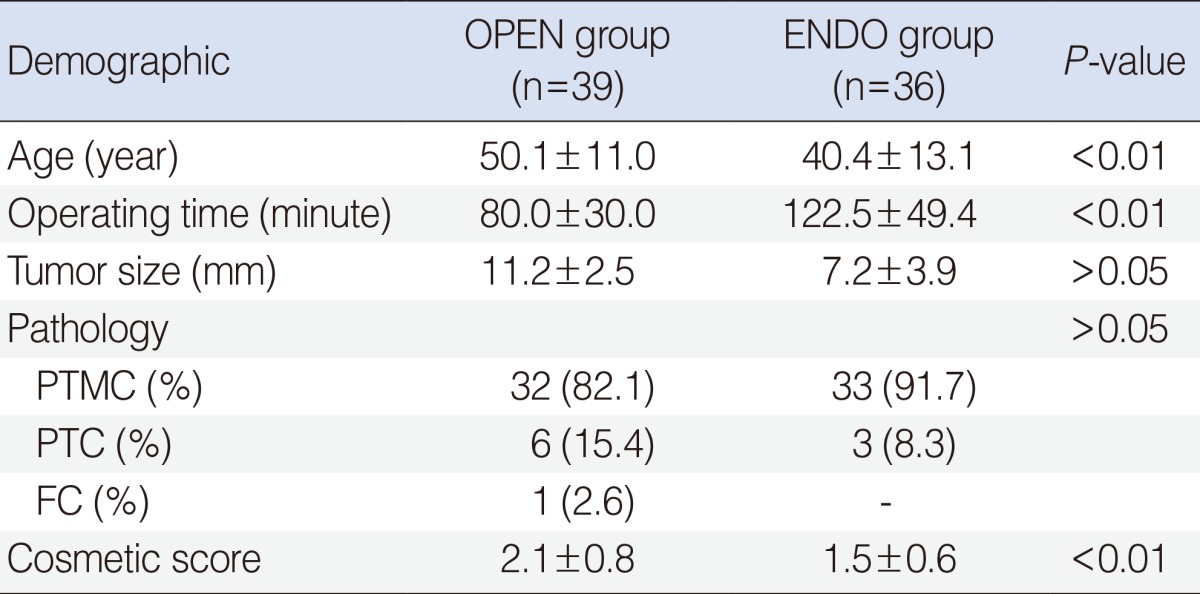
Values are presented as mean±SD or number (%).
OPEN group, conventional open thyroidectomy group; ENDO group, endoscopic thyroidectomy group; PTMC, papillary thyroid microcarcinoma; PTC, papillary thyroid carcinoma; FC, follicular carcinoma; Cosmetic score, 5-point visual analog scale of the cosmetic satisfaction score.
P<0.01, using the paired t-test.
Objective parameters
Figs. 2 and 3 present the objective parameters for the OPEN and ENDO groups, respectively. For the OPEN group, significant decreases were observed in Max F0 and Mean F0 in the early postoperative period (P<0.05). For the ENDO group, significant decreases were observed in Max F0 and Mean F0 in the early postoperative period (P<0.05), while the average percentages of jitter had increased significantly in the early postoperative period (P<0.05). These parameters had improved gradually and did not differ significantly in the late postoperative period for both OPEN and ENDO groups.
Fig. 2.

Changes in the objective parameters during follow-up in the conventional open thyroidectomy group. PreOp, preoperatively; Post 1M, 1 month postoperatively; Post 6M, 6 months postoperatively; MPT, maximum phonation time (second); Max/Mean/Min F0/20, maximum/mean/minimum fundamental frequency/20; HNR/10, harmonics-to-noise ratio (dB)/10; CQ/10, contact quotient (%) of the electroglottograph/10. *P<0.05, using paired t-test, PreOp vs. Post 1M.
Fig. 3.

Changes in the subjective parameters during follow-up in the conventional open thyroidectomy group. PreOp, preoperatively; Post 1M, 1 month postoperatively; Post 6M, 6 months postoperatively; GRBAS, grade, roughness, breathiness, asthenia, and strain; GRBAS, sum of the GRBAS scale; VHI, voice handicap index; Vocal fatigue, visual analog scale of the patients' symptomatic rating of vocal fatigue; Singing, visual analog scale of the patients' symptomatic rating of the singing difficulty; High pitch, visual analog scale of the patients' symptomatic rating of the high-pitched voice difficulty; Neck discomfort, visual analog scale of the patients' symptomatic rating of neck discomfort. *,†P<0.05, using paired t-test. *PreOp vs. Post 1M. †PreOp vs. Post 6M.
Subjective parameters
Figs. 4 and 5 present the subjective parameters for the OPEN and ENDO groups, respectively. For the OPEN group, the sum of the GRBAS scale, VHI, and the average VAS scores for vocal fatigue, singing, difficulty with high pitch, and neck discomfort significantly had got worsen in the early postoperative period (P<0.05), although most of the parameters had improved gradually in the late postoperative period, except for difficulty with high-pitched and singing voices (P>0.05). These parameters had not improved until 6 months postoperatively when compared to the preoperative status (P<0.05).
Fig. 4.

Changes in the objective parameters during follow-up in the endoscopic thyroidectomy group. PreOp, preoperatively; Post 1M, 1 month postoperatively; Post 6M, 6 months postoperatively; MPT, maximum phonation time (second); Max/Mean/Min F0/20, maximum/mean/minimum fundamental frequency/20; HNR/10, harmonics-to-noise ratio (dB)/10; CQ/10, contact quotient (%) of the electroglottograph/10. *P<0.05, using paired t-test. PreOp vs. Post 1M.
Fig. 5.

Changes in the subjective parameters during follow-up in the endoscopic thyroidectomy group. PreOp, preoperatively; Post 1M, 1 month postoperatively; Post 6M, 6 months postoperatively; GRBAS, grade, roughness, breathiness, asthenia, and strain; GRBAS, sum of the GRBAS scale; VHI, voice handicap index; Vocal fatigue, visual analog scale of the patients' symptomatic rating of vocal fatigue; Singing, visual analog scale of the patients' symptomatic rating of the singing difficulty; High pitch, visual analog scale of the patients' symptomatic rating of the high-pitched voice difficulty; Neck discomfort, visual analog scale of the patients' symptomatic rating of neck discomfort. *,†P<0.05, using paired t-test. *PreOp vs. Post 1M. †PreOp vs. Post 6M.
For the ENDO group, the sum of the GRBAS scale, VHI, and average scores for vocal fatigue, singing, high pitch, and neck discomfort significantly had got worsen in the early postoperative period (P<0.05). Most of the parameters had improved gradually by the late postoperative period, except for VHI, high-pitched voice, and singing voice (P>0.05), which had not improved until 6 months postoperatively when compared to the preoperative status (P<0.05).
Complications
Complications related to the thyroidectomy in this study were two cases of temporary vocal fold paralysis, one case of postoperative hematoma in the ENDO group, and one case of vocal cord paralysis in the OPEN group (P>0.05).
DISCUSSION
As surgeons, we have noticed many similar complaints from patients following simple thyroidectomy, even when the RLN had been identified and preserved. Typical voice complaints include easy fatigue during phonation and difficulty with high-pitched and singing voices. Other symptoms include paresthesia, vague voice changes, neck discomfort, sudden sting pain, and a feeling of choking [7]. Some call these changes 'thyroid surgery-related voice changes' [8]. However, no systematic clinical study of this syndrome has been performed. This collection of symptoms appears to be a real syndrome. We call this collection of symptoms PTS. Several hypotheses have been proposed to explain the collection of voice changes following thyroidectomy. Currently, the most likely explanation is laryngotracheal fixation between the trachea and strap muscle, resulting in impaired strap muscle function [4,9]. Other suggested causes are SLN or pharyngeal plexus damage and delayed laryngeal lymph edema from thyroid surgery [1,2,10]. The exact cause of this collection of symptoms, however, remains unclear. Among these causes, laryngotracheal fixation is the most suggested cause of PTS, however, the exact cause of PTS is not clear until now.
ENDO is under development and is being popularized in some Asian countries because this approach confers better cosmetic benefits and an excellent operative view compared to conventional thyroidectomy. However, it is more invasive because it requires a wider skin flap and access from remote sites [11]. Although several papers on the operative outcomes of ENDO and OPEN have reported, no prospective trials comparing the functional outcomes, including postoperative discomfort and voice changes, between ENDO and OPEN.
Theoretically, PTS following ENDO should be more severe and last longer than after OPEN because endoscopic surgery needs wider dissection to access the thyroid gland. However, the natural history of PTS with preserved RLN function has not been studied systematically.
We conducted a prospective observational study for comparing the results between OPEN vs. ENDO patients with a normal preoperative voice, and then evaluated the presence of PTS by evaluating the changes in subjective and objective parameters.
We found that PTS really existed following simple thyroidectomy and were very common in both the OPEN and ENDO groups. However, no significant difference was observed in PTS following thyroidectomy between the ENDO and OPEN groups. Changes in the Max F0 and Mean F0 were seen in the early postoperative period for both groups. Typical voice symptoms after thyroidectomy in the early postoperative period were easy vocal fatigue and difficulty with high-pitched and singing voices. Most of the parameters had improved gradually with time, although some changes persisted 6 months postoperatively, especially those involved in singing and high-pitched voices.
Recent studies have demonstrated that a few objective parameters changed following thyroidectomy, including fundamental frequency, shimmer, and jitter, but these results were inconsistent [4].
We postulated that the drop of maximum and Mean F0 frequency in the early postoperative period could be from laryngotracheal fixation with impaired vertical movement or temporary malfunction of the strap muscle [4]. The strap muscles may be damaged during forceful lateral retraction, cut during thyroid surgery, or affected by wound contracture after surgery. The another cause of fundamental frequency's drop is the damage of the SLN, this nerve is vulnerable to injury during the ligation of superior pole of thyroid gland, especially for lower lying deviated patient [2]. However, to confirm the SLN injury following thyroidectomy, it is mandatory to performe the regular laryngeal electromyography during follow-up period in the future.
And in some patients of ENDO, the omohyoid muscle might be divided for better exposure of the upper pole, or that the sternothyroid and sternohyoid muscles are strongly retracted upward by the endoscopic retractor during the procedure. This would cause ischemic injury to the strap muscle.
Alternatively, the wider dissection over the pectoralis major and over and below the strap muscle used to reach the thyroid gland might result in more severe wider laryngotracheal fixation, which results in a harsh voice with aggravated jitter.
Based on these results, PTS following thyroidectomy commonly occur in simple thyroidectomy patients. And some subjective voice parameters changes, such as high pitched and sing voice difficulties persisted 6 months postoperatively.
In conclusion, PTS really exists following simple thyroidectomy and are very common for both OPEN and ENDO groups. Most of the parameters had improved gradually over time, but some subjective changes persisted 6 months postoperatively.
ACKNOWLEDGMENTS
This work was supported by the Soonchunhyang University Research Fund.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Sinagra DL, Montesinos MR, Tacchi VA, Moreno JC, Falco JE, Mezzadri NA, et al. Voice changes after thyroidectomy without recurrent laryngeal nerve injury. J Am Coll Surg. 2004 Oct;199(4):556–560. doi: 10.1016/j.jamcollsurg.2004.06.020. [DOI] [PubMed] [Google Scholar]
- 2.Aluffi P, Policarpo M, Cherovac C, Olina M, Dosdegani R, Pia F. Post-thyroidectomy superior laryngeal nerve injury. Eur Arch Otorhinolaryngol. 2001 Nov;258(9):451–454. doi: 10.1007/s004050100382. [DOI] [PubMed] [Google Scholar]
- 3.Stojadinovic A, Shaha AR, Orlikoff RF, Nissan A, Kornak MF, Singh B, et al. Prospective functional voice assessment in patients undergoing thyroid surgery. Ann Surg. 2002 Dec;236(6):823–832. doi: 10.1097/00000658-200212000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hong KH, Kim YK. Phonatory characteristics of patients undergoing thyroidectomy without laryngeal nerve injury. Otolaryngol Head Neck Surg. 1997 Oct;117(4):399–404. doi: 10.1016/S0194-5998(97)70133-5. [DOI] [PubMed] [Google Scholar]
- 5.Koh YW, Park JH, Lee SW, Choi EC. The harmonic scalpel technique without supplementary ligation in total thyroidectomy with central neck dissection: a prospective randomized study. Ann Surg. 2008 Jun;247(6):945–949. doi: 10.1097/SLA.0b013e31816bcd61. [DOI] [PubMed] [Google Scholar]
- 6.Koh YW, Park JH, Kim JW, Lee SW, Choi EC. Clipless and sutureless endoscopic thyroidectomy using only the harmonic scalpel. Surg Endosc. 2010 May;24(5):1117–1125. doi: 10.1007/s00464-009-0738-2. [DOI] [PubMed] [Google Scholar]
- 7.Stojadinovic A, Henry LR, Howard RS, Gurevich-Uvena J, Makashay MJ, Coppit GL, et al. Prospective trial of voice outcomes after thyroidectomy: evaluation of patient-reported and clinician-determined voice assessments in identifying postthyroidectomy dysphonia. Surgery. 2008 Jun;143(6):732–742. doi: 10.1016/j.surg.2007.12.004. [DOI] [PubMed] [Google Scholar]
- 8.McIvor NP, Flint DJ, Gillibrand J, Morton RP. Thyroid surgery and voice-related outcomes. Aust N Z J Surg. 2000 Mar;70(3):179–183. doi: 10.1046/j.1440-1622.2000.01781.x. [DOI] [PubMed] [Google Scholar]
- 9.Hong KH, Ye M, Kim YM, Kevorkian KF, Berke GS. The role of strap muscles in phonation--in vivo canine laryngeal model. J Voice. 1997 Mar;11(1):23–32. doi: 10.1016/s0892-1997(97)80020-3. [DOI] [PubMed] [Google Scholar]
- 10.de Pedro Netto I, Fae A, Vartanian JG, Barros AP, Correia LM, Toledo RN, et al. Voice and vocal self-assessment after thyroidectomy. Head Neck. 2006 Dec;28(12):1106–1114. doi: 10.1002/hed.20480. [DOI] [PubMed] [Google Scholar]
- 11.Koh YW, Park JH, Kim JW, Lee SW, Choi EC. Endoscopic hemithyroidectomy with prophylactic ipsilateral central neck dissection via an unilateral axillo-breast approach without gas insufflation for unilateral micropapillary thyroid carcinoma: preliminary report. Surg Endosc. 2010 Jan;24(1):188–197. doi: 10.1007/s00464-009-0646-5. [DOI] [PubMed] [Google Scholar]