

Abstract
Background:
Modern microsurgical techniques enable en bloc resection of complex skull base tumors. Anterior cranial base surgery, particularly, has been associated with a high rate of postoperative cerebrospinal fluid (CSF) leak, meningitis, intracranial abscess, and pneumocephalus. We introduce simple modifications to already existing surgical strategies designed to minimize the incidence of postoperative CSF leak and associated morbidity and mortality.
Methods:
Medical records from 1995 to 2013 were reviewed in accordance with the Institutional Review Board. We identified 21 patients who underwent operations for repair of large anterior skull base defects following removal of sinonasal or intracranial pathology using standard craniofacial procedures. Patient charts were screened for CSF leak, meningitis, or intracranial abscess formation.
Results:
A total of 15 male and 6 female patients with an age range of 26–89 years were included. All patients were managed with the same operative technique for reconstruction of the frontal dura and skull base defect. Spinal drainage was used intraoperatively in all cases but the lumbar drain was removed at the end of each case in all patients. Only one patient required re-operation for repair of persistent CSF leak. None of the patients developed meningitis or intracranial abscess. There were no perioperative mortalities. Median follow-up was 10 months.
Conclusion:
The layered reconstruction of large anterior cranial fossa defects resulted in postoperative CSF leak in only 5% of the patients and represents a simple and effective closure option for skull base surgeons.
Keywords: Cerebrospinal fluid leak, reconstruction, skull base defect
INTRODUCTION
Advances in diagnostic tools and microsurgical techniques have enabled multidisciplinary teams of otolaryngologists and neurosurgeons to treat complex skull base lesions [Figure 1]. Repair of large anterior cranial fossa defects following tumor resection or craniofacial trauma is challenging because of the extensive bony defects and dural openings that require reconstruction.[2] Historically, craniotomies for anterior cranial fossa pathology have resulted in a greater incidence of postoperative cerebrospinal fluid (CSF) leak than craniotomies for similar pathology in middle or posterior cranial fossa.[13] The success of anterior skull base surgery is dependent on a watertight dural closure to prevent postoperative CSF leak that could complicate up to 41% of cases.[7] It is also vital that the closure provide a barrier between the sinonasal tracts and the sterile intracranial environment to avoid delayed meningitis, and possibly death, that are reported in 10–25% of patients in literature.[25] We introduce novel, yet simple, modifications to some already existing techniques for reconstruction of large anterior cranial base dural defects that are durable, effective, and could reduce postoperative CSF leak and its associated morbidity.
Figure 1.
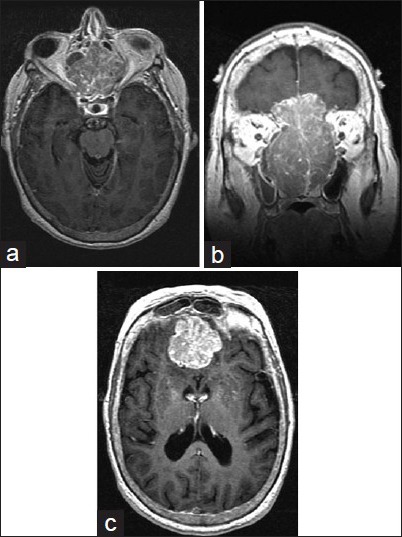
Preoperative T1 MRI + C of a patient with esthesioneuroblastoma who presented with rhinorrhea demonstrating obliteration of the (a) sinonasal cavity, (b) destruction of the anterior cranial fossa, and (c) intracranial extension
Technique
A standard bicoronal incision is made with great attention to preserving the pericranial layer. The scalp flap is then reflected and dissected in the subgaleal plane to the level of the supraorbital rims. The pericranium is incised at the level of the incision and bluntly dissected forward while avoiding electrocautery to preserve the blood supply from the supratrochlear and supraorbital arteries. The harvested pericranium is then wrapped in a moist sponge to prevent desiccation and over-manipulation during this several hours long procedure. After tumor resection and basal-frontal osteotomies by both the neurosurgical and otolaryngology teams, a primary closure of the resected dura is performed by taking a generous piece of tensor facia lata, covering the dural defect, and leaving a 3-cm extension of graft material to overlap the posterior aspect of the frontal fossa. The tensor fascia is sutured to the dural defect in an “in-out-in” fashion beginning at the inferior midline and continuing bilaterally around the defect. The novelty of this approach centers on leaving a small cuff of dura anterior to the optic chiasm during tumor resection. Preserving this small cuff of dura allows the surgeon to suture the graft securely to a stationary piece of tissue on the floor of the anterior fossa, thereby ensuring a successful closure [Figures 2 and 3]. This may lead to incomplete resection of infiltrated dura, but watertight dural closure is most important in extensive resection cases. Before placing the final sutures at the superior midline margin of the graft, saline is irrigated into the reconstructed dura while the dural margin is pinched and sealed off around the irrigator so as to ensure a watertight closure. The repaired dural margins are meticulously inspected circumferentially and if specific areas are noted to be leaking, additional interrupted sutures are placed where necessary.
Figure 2.
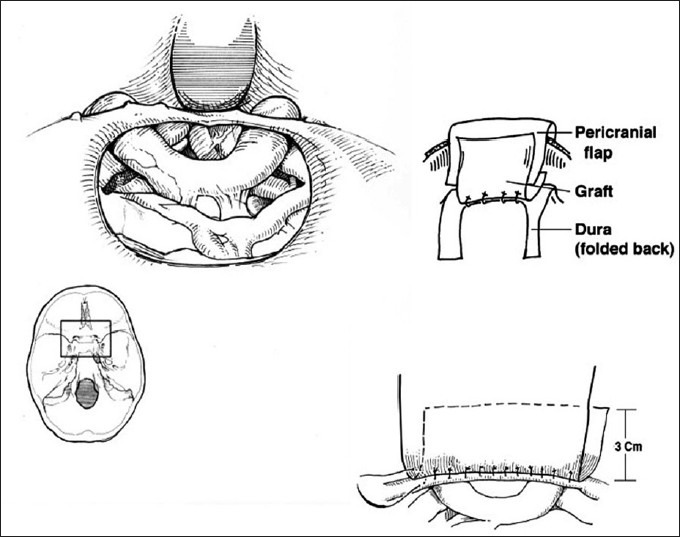
Schematic diagram demonstrating a large dural defect in the anterior cranial base (bottom and top left), the layering of the dural graft over the pericranial flap (top right), and the in-out-in fashion by which the dural graft is sutured (bottom right)
Figure 3.
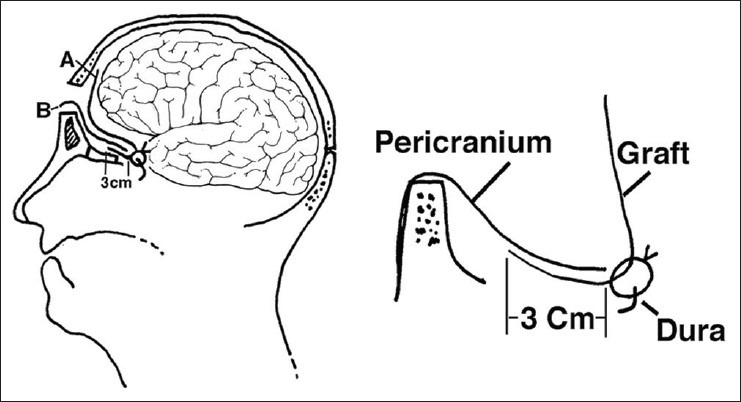
Schematic diagram demonstrates how postoperative expansion of the frontal lobe over the layered closure provides additional fortification (left) as well as a detailed view of the layers of graft material involved in this closure technique (right)
After satisfactory watertight closure is achieved, a piece of cadaveric bone or titanium mesh is fastened with screws to the medial orbital bone, thereby providing a scaffold for separation of the intracranial and nasal compartments [Figure 4]. At this juncture, the harvested vascularized pericranium is gently rotated and then tacked to the most posterior aspect of the frontal graft dura and layered over the 3-cm extension of the frontal dura between the two leaves of tensor fascia lata graft. This “sandwich” technique provides three layers of protection and strengthens the water-tight closure. Postoperative expansion of the frontal lobe over the layered reconstruction of dura and bony anterior cranial fossa floor provides additional support by reinforcing the watertight seal [Figure 3 left panel, Figure 5]. While spinal drainage was used in all cases, the lumbar drain was removed before the patient left the operating room in each case.
Figure 4.
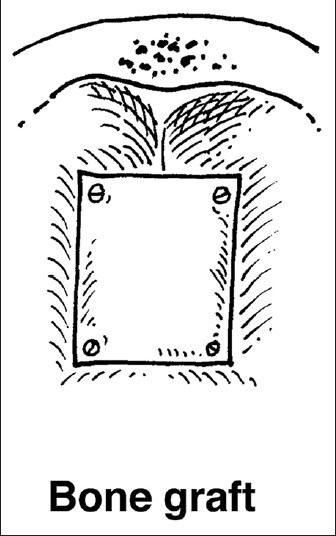
Piece of cadaveric bone or titanium mesh shaped to the defect and fastened to the medial orbital bones provides scaffolding and separates the intranasal and intracranial compartments
Figure 5.
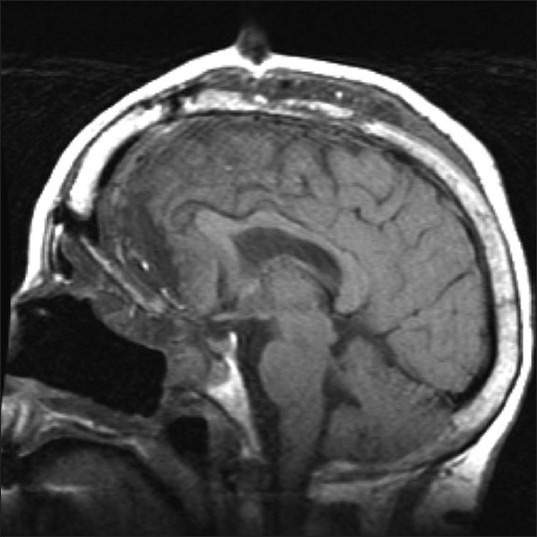
Postoperative T1-weighted MRI demonstrates expansion of the frontal lobe reinforcing the reconstructed, basal-frontal dura
METHODS
In accordance with the Institutional Review Board at our hospital, we identified 21 patients who underwent craniotomies for resection of disparate primary pathologies followed by reconstruction of their large anterior skull base and dural defects using the senior author's proposed technique. This was the only surgical reconstruction technique utilized at our institution by the senior author, regardless of the pathology or extent of dural and cranial defects. The rate of postoperative CSF leak, meningitis, or intracranial abscess formation was calculated by screening patient charts for complications.
RESULTS
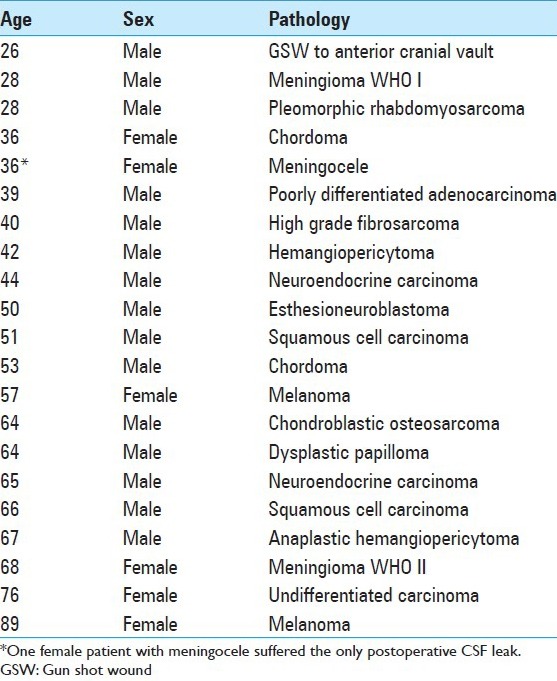
Of the 21 patients included in this study, 71% were male and 29% female with an age range of 26–89 years. The pathologic diagnosis varied from benign meningioma to pleomorphic rhabdomyosarcoma and included a patient with ballistic trauma to the anterior cranial vault. Only one female patient with a meningocele suffered a postoperative CSF leak early in our experience with this closure technique and required a second, endoscopic transnasal operation for definitive repair [Table 1]. None of the patients developed meningitis or intracranial abscess. There were no mortalities related to delayed CSF leak. The median follow-up was 10 months with a range of 1–99 months.
Table 1.
Patient demographics and pathologic diagnoses
DISCUSSION
Hugh Cairns, a British neurosurgeon, was the first to introduce a classification scheme for CSF rhinorrhea in 1937 and differentiated between spontaneous and postoperative CSF leak.[1] In 1926, Dandy was the first to successfully repair a CSF fistula using a tensor fascia lata graft through a transcranial, intradural approach.[4] Since then, various techniques for anterior cranial fossa reconstruction after extensive craniotomy for extirpation of various pathologies have been described in the literature, ranging from no formal reconstruction to elaborate free flaps with microvascular anastomosis. Although no one technique is superior in any given situation, Gil et al. emphasized the importance of tailored reconstruction depending on the extent of resection and degree of dural and cranial defects.[5] In simple cases, meticulous dural closure is sufficient where all small defects are closed primarily. A graft of temporalis fascia can be used for small defects, while harvested fascia lata sheaths are used for bigger and more extensive skull base and dural defects.
Ketcham et al.'s initial series reported in 1963 popularized craniofacial resection approaches to neoplasms of the anterior skull base.[9,10] The key to reducing morbidity of these elegant approaches is a meticulous reconstructive closure; yet, there remains no gold standard technique to close the surgical defects. This is in part due to the small number of patients treated in any one center and the preference of individual surgeons as to which reconstructive techniques are used.
In his series, Ketcham described using only a split-thickness skin graft placed on dura.[9,10] This simplistic approach had its shortcomings when used to reconstruct large defects. This method was eventually modified by Schramm et al. in 1979 who used a vascularized pedicled galeal flap over fascia lata.[20]
Schafer et al. then described what probably is the most commonly utilized method of reconstructing the anterior skull base today, which involves the pericranial flap.[18] The appeal of this flap comes from its ease of harvesting (no second incision), rich blood supply, and minimal cosmetic disturbance. Recent modifications of the pericranial flap include the galeal-pericranial and galeal frontalis myofacial flaps, which add more layers to the construct.
The use of temporalis muscle flap has also been described in situations with superior orbital wall involvement. The muscle and its investing fascia are dissected down to their insertion point with preservation of the coronoid process to protect the blood supply. The muscle is then rotated to cover the defect. Additionally, free muscle flaps (such as the rectus abdomenins) are also used for reconstruction of extensive anterior skull base defects.
All these techniques can be combined and augmented with composite split-calvarial grafts and porcine dermis allografts, as well as numerous synthetic material such as titanium mesh and high-viscosity polymethylmethacrylate (PMMA). In some cases, the repaired dural defect is covered with a second layer of fascia applied against the entire surface of frontal fossa. Fibrin glue is used to provide additional protection against CSF leakage.[3,8,11,12,14,15,17,21,22,23]
Ever since the German otolaryngologist Malte Wigand pioneered the use of intraoperative endoscope for repair of spontaneous CSF rhinorrhea in 1981,[24] rapid advances in endoscopic techniques have popularized the use of endoscopy for repair of anterior cranial fossa CSF leaks.[6] While endoscopic techniques prove advantageous in the repair of small, spontaneous, and localizable CSF fistulas because they reduce blood loss and operative time,[12] classic surgical approaches still play a role and may, in fact, prove superior in select cases where the dural defect is extensive or the CSF fistula is not localizable.[16,19]
Here we present our experience with a simple technique for watertight dural reconstruction following repair of large anterior cranial fossa defects. The rationale behind the need for a watertight dural closure is to effectively separate the intradural and extradural compartments to reduce the postoperative morbidity and mortality associated with persistent CSF leak. In our case series of 21 patients, after craniofacial approach for primary pathology resection and/or repair, all patients were left with extensive dural and bony defects. Early in our experience, we reconstructed large anterior cranial fossa dural defects with a smaller tensor fascia lata patch and an abdominal fat graft anterior to the dural repair, and reinforced the floor of the frontal fossa with vascularized pericranium without a scaffold to separate the intracranial and intranasal compartments. The limited flexibility of our tensor fascia lata graft prevented re-expansion of the frontal lobe into the frontal fossa and the continuity between the intranasal and intracranial potential spaces resulted in significant extradural pneumocranium and CSF leaks that necessitated a change in our technique [Figure 6]. Additionally, early in our experience and prior to using the aforementioned technique, we left spinal drains in our patients but, unfortunately, one of our earlier patients herniated as a result of over-drainage. Since that incident, we have removed all spinal drains from our patients prior to their leaving the operating room. The use of a calibrated CSF drainage reservoir is a potential alternative to our technique; however, it may result in a higher risk of postoperative infection and meningitis. We prefer to make a demonstrably water-tight dural closure and, in so doing, have not felt it necessary to continue spinal drainage in the postoperative phase.
Figure 6.
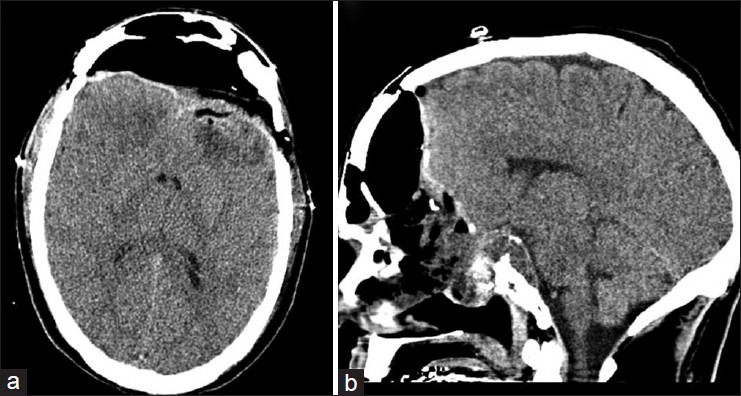
Postoperative sagittal (a) and axial (b) NCCT demonstrating pneumocranium following closure of the primary frontal dura
We have no strict criteria for selecting cadaveric bone versus a titanium mesh for re-establishment of the anterior cranial fossa floor because our primary objective is to buttress the frontal dural repair. In cases where we could harvest a flat piece of cadaveric bone that would fit the anterior cranial fossa defect relatively snugly, we preferentially used cadaveric bone. Otherwise we used a titanium mesh and shaped it to appropriately fit the frontal fossa floor defect. We understand that the theoretical risk of biologic or cadaveric bone buttress failure may be higher in patients who will receive postoperative radiation, however, thus far in our experience we have not encountered any radiation-induced bone resorption or structural failures.
We think the advantage of our closure technique is that it utilizes multiple layers of tissue to repair the frontal fossa dura, while the underlying reconstructed anterior cranial base provides a solid scaffold and reestablishes separate intracranial and sinus compartments. Using generously sized fascia lata graft allows the brain to relax into its normal anatomical position while the natural weight of the frontal lobe may further fortify this layered closure. Defect size is not a limiting factor because large vascularized pericranium or fascia lata grafts can be easily harvested and sewn into position. More importantly, this technique does not require a significant learning curve and is easily mastered. A potential disadvantage of our technique is that it relies on the integrity of an extension of the posterior frontal dura, which could be compromised during lesion resection or trauma, leaving little to no intact dural cuff to sew the graft. However, with care, a small remnant of dura can almost always be left intact. Another potential disadvantage of this technique is in leaving a possibly tumor-infiltrated piece of dura, which may become a site of recurrence. This has not occurred in our series and if it were to occur, some form of radiation therapy would likely be required.
CONCLUSION
Reconstruction of complex anterior skull base defects remains a challenge for otolaryngologists and neurosurgeons despite numerous advances in diagnostic capabilities, endoscopic techniques, surgical approaches, and availability of various materials for grafting. Regardless of the reconstruction methods used, the primary goals of any reconstruction should focus on attaining a watertight seal, providing a durable barrier between the sinonasal tract and intracranial compartment, and providing structural integrity to prevent brain herniation into the surgical defect. While this case series of 21 patients is a relatively small cohort, we feel that the 95% success rate heralds a robust technique for reconstruction of large anterior skull base defects.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2015/6/1/20/151259
Contributor Information
Kevin Reinard, Email: kreinar1@hfhs.org.
Azam Basheer, Email: abashee1@hfhs.org.
Lamont Jones, Email: ljones5@hfhs.org.
Robert Standring, Email: rstandr1@hfhs.org.
Ian Lee, Email: ilee1@hfhs.org.
Jack Rock, Email: jrock1@hfhs.org.
REFERENCES
- 1.Cairns H. Injuries of the frontal and ethmoidal sinuses with special reference to cerebrospinal rhinorrhoea aeroceles. J Laryngol Otol. 1937;52:589–623. [Google Scholar]
- 2.Chang DW, Langstein HN, Gupta A, De Monte F, Do KA, Wang X, et al. Reconstructive management of cranial base defects after tumor ablation. Plast Reconstr Surg. 2001;107:1346–55. doi: 10.1097/00006534-200105000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Chiu ES, Kraus D, Bui DT, Mehrara BJ, Disa JJ, Bilsky M, et al. Anterior and middle cranial fossa skull base reconstruction using microvascular free tissue techniques: Surgical complications and functional outcomes. Ann Plast Surg. 2008;60:514–20. doi: 10.1097/SAP.0b013e3181715707. [DOI] [PubMed] [Google Scholar]
- 4.Dandy WE. Pneumocephalus (intracranial penumatocele or aerocele) Arch Surg. 1926;12:949–82. [Google Scholar]
- 5.Gil Z, Abergel A, Leider-Trejo L, Khafif A, Margalit N, Amir A, et al. A comprehensive algorithm for anterior skullbase reconstruction after oncological resections. Skull Base. 2007;17:25–37. doi: 10.1055/s-2006-959333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gun R, Tosun F, Durmaz A, Yorgancilar E, Bakir S, Kamasak K, et al. Predictors of surgical approaches for the repair of anterior cranial base encephaloceles. Eur Arch Otorhinolaryngol. 2013;270:1299–305. doi: 10.1007/s00405-012-2174-5. [DOI] [PubMed] [Google Scholar]
- 7.Imola MJ, Sciarretta V, Schramm VL. Skull base reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2003;11:282–90. doi: 10.1097/00020840-200308000-00012. [DOI] [PubMed] [Google Scholar]
- 8.Kantrowitz AB, Hall C, Moser F, Spallone A, Feghali JG. Split-calvaria osteoplastic rotational flap for anterior fossa floor repair after tumor excision. Technical note. J Neurosurg. 1993;79:782–6. doi: 10.3171/jns.1993.79.5.0782. [DOI] [PubMed] [Google Scholar]
- 9.Ketcham AS, Chretien PB, Van Buren JM, Hoye RC, Beazley RM, Herdt JR. The ethmoid sinuses: A re-evaluation of surgical resection. Am J Surg. 1973;126:469–76. doi: 10.1016/s0002-9610(73)80032-7. [DOI] [PubMed] [Google Scholar]
- 10.Ketcham AS, Wilkins RH, Van Buren JM, Smith RR. A combined intracranial facial approach to the paranasal sinuses. Am J Surg. 1963;106:698–703. doi: 10.1016/0002-9610(63)90387-8. [DOI] [PubMed] [Google Scholar]
- 11.Lesavoy MA, Lee GK, Fan K, Dickinson B. Split, temporalis muscle flap for repair of recalcitrant cerebrospinal fluid leaks of the anterior cranial fossa. J Craniofac Surg. 2012;23:539–42. doi: 10.1097/SCS.0b013e3182418f18. [DOI] [PubMed] [Google Scholar]
- 12.Locatelli D, Rampa F, Acchiardi I, Bignami M, De Bernardi F, Castelnuovo P. Endoscopic endonasal approaches for repair of cerebrospinal fluid leaks: Nine-year experience. Neurosurgery. 2006;58(4 Suppl 2):ONS 246–56. doi: 10.1227/01.NEU.0000193924.65297.3F. [DOI] [PubMed] [Google Scholar]
- 13.Loew F, Pertuiset B, Chaumier EE, Jaksche H. Traumatic, spontaneous and postoperative CSF rhinorrhea. Adv Tech Stand Neurosurg. 1984;11:169–207. doi: 10.1007/978-3-7091-7015-1_6. [DOI] [PubMed] [Google Scholar]
- 14.Moliterno JA, Mubita LL, Huang C, Boockvar JA. High-viscosity polymethylmethacrylate cement for endoscopic anterior cranial base reconstruction. J Neurosurg. 2010;113:1100–5. doi: 10.3171/2010.3.JNS09453. [DOI] [PubMed] [Google Scholar]
- 15.Quinones-Hinojosa A, Schmidek HH. 6th ed. Philadelphia: PA: Elsevier/Saunders; 2012. Schmidek and Sweet operative neurosurgical techniques: Indications, methods, and results. [Google Scholar]
- 16.Rocchi G, Caroli E, Belli E, Salvati M, Cimatti M, Delfini R. Severe craniofacial fractures with frontobasal involvement and cerebrospinal fluid fistula: Indications for surgical repair. Surg Neurol. 2005;63:559–63. doi: 10.1016/j.surneu.2004.07.047. [DOI] [PubMed] [Google Scholar]
- 17.Sakas DE, Beale DJ, Ameen AA, Whitwell HL, Whittaker KW, Krebs AJ, et al. Compound anterior cranial base fractures: Classification using computerized tomography scanning as a basis for selection of patients for dural repair. J Neurosurg. 1998;88:471–7. doi: 10.3171/jns.1998.88.3.0471. [DOI] [PubMed] [Google Scholar]
- 18.Schaefer SD, Close LG, Mickey BE. Axial subcutaneous scalp flaps in the reconstruction of the anterior cranial fossa. Arch Otolaryngol Head Neck Surg. 1986;112:745–9. doi: 10.1001/archotol.1986.03780070057012. [DOI] [PubMed] [Google Scholar]
- 19.Scholsem M, Scholtes F, Collignon F, Robe P, Dubuisson A, Kaschten B, et al. Surgical Management of anterior cranial base fractures with cerebrospinal fluid fistulae: A single-institution experience. Neurosurgery. 2008;62:463–71. doi: 10.1227/01.neu.0000316014.97926.82. [DOI] [PubMed] [Google Scholar]
- 20.Schramm VL, Myers EN, Maroon JC. Anterior skull base surgery for benign and malignant disease. Laryngoscope. 1979;89:1077–91. [PubMed] [Google Scholar]
- 21.Snyderman CH, Janecka IP, Sekhar LN, Sen CN, Eibling DE. Anterior cranial base reconstruction: Role of galeal and pericranial flaps. Laryngoscope. 1990;100:607–14. doi: 10.1288/00005537-199006000-00011. [DOI] [PubMed] [Google Scholar]
- 22.Spear S, Iskandar J, Seaquist D, Sorensen D. Nasoseptal chondrosarcoma resection requiring anterior fossa floor repair: A case report. Ear Nose Throat J. 2008;87:696–9. [PubMed] [Google Scholar]
- 23.Thakker JS, Fernandes R. Evaluation of reconstructive techniques for anterior and middle skull base defects following tumor ablation. J Oral Maxillofac Surg. 2014;72:198–204. doi: 10.1016/j.joms.2013.05.017. [DOI] [PubMed] [Google Scholar]
- 24.Wigand ME. Transnasal ethmoidectomy under endoscopical control. Rhinology. 1981;19:7–15. [PubMed] [Google Scholar]
- 25.Ziu M, Savage JG, Jimenez DF. Diagnosis and treatment of cerebrospinal fluid rhinorrhea following accidental traumatic anterior skull base fractures. Neurosurg Focus. 2012;32:E3. doi: 10.3171/2012.4.FOCUS1244. [DOI] [PubMed] [Google Scholar]