

Abstract
[Purpose] The aim of this study was to evaluate the effects of scapula-upward taping (SUT) in a patient with shoulder pain caused by scapular downward rotation (SDR). [Subject] A 26-year-old male with SDR experienced severe pain in the left shoulder when he lifted his left upper extremity to hold the handle in a bus and during and after push-up exercise. [Methods] The patient underwent SUT for a period of 1 month, 5 times per week, for an average of 9 h/d. [Results] The patient’s radiographs showed that the degree of SDR had decreased; the left shoulder pain also decreased in the resting state and during and after push-up exercise. The manual muscle strength test grades of the upper trapezius, lower trapezius, and serratus anterior had increased. The patient was able to lift the left upper extremity to hold the handle in a bus and perform the push-up exercise without experiencing any pain. [Conclusion] Repeated SUT application may be a beneficial treatment method for alleviating the degree of SDR and shoulder pain in SDR patients.
Key words: Muscle imbalance, Scapular upward rotation, Push-up exercise
INTRODUCTION
Assessment of scapula static position is an essential component of a shoulder examination1, 2) because impaired postural alignment may cause excessive compression and stress and, consequently, pain involving the muscles, joints, and ligaments3).
In scapular downward rotation (SDR), the inferior angle of the scapula is more medial than the superior angle, thereby affecting the compressive loading of the cervical vertebra through transfer of the weight of the upper arm to the cervical area due to the attachments of the cervicoscapular muscles such as the upper trapezius (UT) and levator scapulae (LS)4). In addition, the pain caused by SDR is the result of decreased scapular upward rotation during upper extremity elevation5).
We report the application of scapula-upward taping (SUT) with kinesiology tape to facilitate upward rotation of the scapula in a patient with shoulder pain caused by unilateral SDR.
SUBJECT AND METHODS
A 26-year-old man experienced severe pain in the left shoulder for 6 months when lifting the left upper extremity to hold the handle in a bus and during and after push-up exercise. This study was approved by the Ethics Committee of Dong-Eui University, in accordance with the ethical standards of the Declaration of Helsinki (DIRB-201405-HR-R-024). The initial radiography performed to determine the static location of the scapula showed that the inferior border of the scapula was more medial than the superior border, and this observation was more prominent on the left side than on the right side.
To assess the level of pain in the left shoulder, the pressure pain threshold (PPT) was measured using an algometer (Pain Test Model FPK; Wagner Instruments, Greenwich, CT, USA)6); the instrument was placed between the acromion and spinous process of the second thoracic vertebra while the patient was in the sitting position. The PPT was found to be 1 kg. In addition, the numeric pain rating scale (NPRS) (0, no pain; 10, worst possible pain) was also used: a score of 3/10 was observed in the resting state, and a score of 7/10 was observed during and after push-up exercise.
Manual muscle strength testing of the shoulder musculature was performed as stated by Kendall2). At the initial assessment, the strength values of the UT, lower trapezius (LT), and SA were 3+/5, 3/5, and 4/5, respectively.
Methods
We applied SUT for 1 month, 5 times per week, for an average of 9 h each day, to facilitate upward rotation of the scapula. The SUT was applied by a physical therapist with high expertise in kinesiology taping. To induce the mechanical correction effect of rotating the scapula upward, the kinesiology tape (BB TAPE, WETAPE Inc., Seoul, Korea) was applied with approximately 50–60% stretch from the acromion to the cervical spine (Fig. 1A), from the midpoint of the UP to the inferior scapular angle (Fig. 1B), from the inferior scapular angle to the posterior deltoid (Fig. 1C), and from the scapular spine to the spinous process of the twelfth thoracic vertebrae (Fig. 1D) according to the order in the upper extremity elevation position to facilitate scapular upward rotation. Because skin problems caused by the tension of the tape often appear clinically at the beginning and end of tape application, the ends of the kinesiology tape (approximately 4–5 cm) were not stretched. In addition, to prevent any skin allergies during the SUT intervention, the tape was removed instantly if the patient felt any itching sensation or after sweating due to exercise. Further, even if the skin was not itchy, the tape was not applied for more than one day. Other therapeutic interventions were not applied to treat the SDR or the pain in the left shoulder.
Fig. 1.
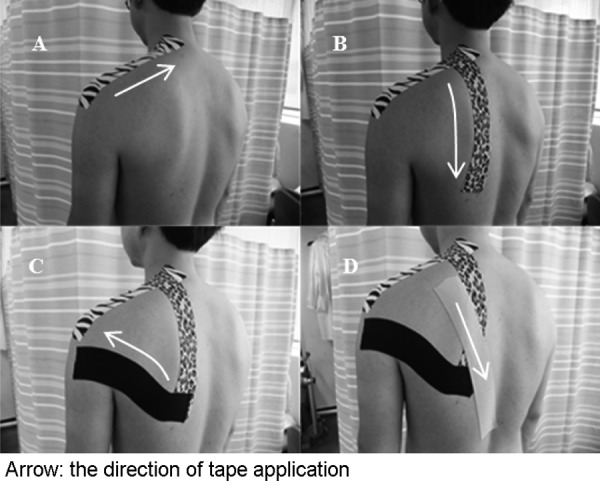
Kinesiology tape application to facilitate left scapular upward rotation
RESULTS
After the SUT intervention, the PPT of the UP increased from 1 to 6.6 kg, and the NPRS of the left shoulder decreased from 3/10 to 0/10 in the resting state and from 7/10 to 0/10 during and after push-up exercise. The final radiograph showed that the degree of SDR had decreased. The manual muscle strength test grades of the UT, LT, and SA had increased to 4+/5, 4+/5, and 4+/5, respectively. Further, the patient experienced no pain when lifting the left upper extremity to hold the handle in a bus and during and after push-up exercise.
DISCUSSION
This study showed that repeated SUT application helps decrease the degree of SDR and pain and increase the strength of the muscles that work in scapular upward rotation such as the UT, LT, and SA. The decrease in the degree of SDR can be achieved by reducing the elasticity of the scapula after SUT application and assisting in scapular upward rotation, as the tape is flexible enough to recoil back to its original length during shoulder activity7,8,9). This can be done by applying the tape with approximately 50–60% stretch in the scapular upward rotation position.
The relationship between misalignment and pain is not yet clear; however, misalignment is one of the many factors leading to mechanical pain1). Recent studies reported a decrease in shoulder pain owing to the mechanical correction effect of scapular elevation7). Therefore, correction of the left scapular alignment by decreasing the degree of SDR through SUT application may help alleviate mechanical shoulder pain.
Muscle imbalance occurs when an agonist is abnormally shortened or lengthened more than an antagonist10). Muscle imbalance may lead to changes in the structure of the body tissues and body function10). Therefore, passive correction of the scapular position through repeated SUT application may induce the recovery of the UT, LT, and SA muscle function and muscle power improvement.
The limitations of this study were that the electromyographic activity of the UT, LT, and SA were not measured because the surface electrodes for the UT and LT overlapped with the position for SUT application; in addition, the duration of maintenance of scapula alignment after SUT application was not assessed. Further studies are needed to evaluate the clinical effect of SUT on patients with shoulder pain caused by SDR.
Acknowledgments
This work was supported by Dong-Eui University Research Grant No. 2014AA127.
REFERENCES
- 1.Sahrmann SA: Diagnosis and treatment of movement impairment syndromes. St Louis: Mosby, 2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kendall FP, McCreary EK, Provance PG, et al. : Muscles: Testing and Function, with Posture and Pain, 5th ed. Baltimore: Lippincott Williams & Wilkins, 2005. [Google Scholar]
- 3.Tüzün C, Yorulmaz I, Cindaş A, et al. : Low back pain and posture. Clin Rheumatol, 1999, 18: 308–312. [DOI] [PubMed] [Google Scholar]
- 4.Van Dillen LR, McDonnell MK, Susco TM, et al. : The immediate effect of passive scapular elevation on symptoms with active neck rotation in patients with neck pain. Clin J Pain, 2007, 23: 641–647. [DOI] [PubMed] [Google Scholar]
- 5.Jason Sweas: http://jasonsweas.wordpress.com/patient-education/shoulder-scapula/.
- 6.Lee JH, Han JT: The dose-dependent effect of an 830-nm, 450-mW low-level laser therapy on the myofacial trigger point of the upper trapezius muscle: a randomized, double blinded, clinical trial. J Phys Ther Sci, 2011, 23: 933–935. [Google Scholar]
- 7.Lee JH, Yoo WG: Effect of scapular elevation taping on scapular depression syndrome: a case report. J Back Musculoskeletal Rehabil, 2012, 25: 187–191. [DOI] [PubMed] [Google Scholar]
- 8.Lee JH, Yoo WG: Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Phys Ther Sport, 2012, 13: 279–285. [DOI] [PubMed] [Google Scholar]
- 9.Kim BJ, Lee JH: Efficacy of kinesiology taping for recovery from occupational wrist disorders experienced by a physical therapist. J Phys Ther Sci, 2014, 26: 941–943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Norris CM: Back Stability: Integrating Science and Therapy, 2nd ed. Champaign: Human Kinetics, 2008. [Google Scholar]