

Abstract
Context:
Cognitive behavior therapy (CBT) is the treatment of choice in anxiety disorders. However, there is little evidence for the effectiveness brief CBT in social anxiety.
Aims:
We examined the effectiveness of a brief CBT of six sessions in patients with social anxiety disorder.
Settings and Design:
A single case design study baseline; post and 1 month follow-up was adopted.
Materials and Methods:
Seven patients with a DSM IV diagnosis of social anxiety underwent 6 weekly sessions of brief CBT. Their diagnosis was confirmed using structured diagnostic interviews. They were assessed at baseline, post and 1-month follow-up on CGI- Severity, Leibowitz Social Anxiety Scale (LSAS), Social Phobia Rating Scale, Brief Fear of Negative Evaluation, and Beck's Depression Inventory.
Statistical Analysis:
Data were analyzed using the method of clinical significance.
Results:
Results indicated that brief CBT was effective in reducing social anxiety in all patients. Brief CBT was also effective in reducing social avoidance and self consciousness. However, brief CBT was not effective in reducing fear of negative evaluation in all patients, suggesting the need for longer duration for cognitive changes in some dysfunctional beliefs.
Conclusions:
This preliminary case series indicates that brief CBT may be a promising and a cost and time effective approach to managing for social anxiety.
Keywords: Avoidance single case design, brief CBT, cognitive behavior therapy, social anxiety
INTRODUCTION
Social anxiety disorder (SAD) is a common anxiety disorder[1] associated with significant impairment in overall functioning and a poor rate of spontaneous remission.[2,3,4] SAD has been found to be associated with co morbid depression, suicide, and alcohol abuse.[5]
Pharmacological interventions for SAD include selective serotonin reuptake inhibitors (SSRIs), serotonin, and norepinephrine reuptake inhibitors (SNRIs).[3] However, a large number of patients do not respond adequately and require psychological interventions.[6]
The efficacy of cognitive-behavioral interventions for SAD is well established. Meta analytical studies indicate that exposure alone (EXP) and EXP with cognitive restructuring (CR) are equally effective and have significantly greater effect sizes than wait list control.[7,8,9] Further, CT and EXP, either alone or in combination yield larger effect sizes as compared to social skills training.[7]
Meta analysis comparing pharmacological treatments and cognitive behavior therapy (CBT) have yielded mixed results. Some studies have shown no significant differences between the two approaches, but that both were superior to control conditions,[8] while others indicates that pharmacotherapy yields larger effect sizes in the short term.[10] There is some evidence for higher relapse rate in patients receiving pharmacological treatment in the longer term.[11]
Typically, standard CBT consists of 14-16 weekly or session[12] and adequate medications require 6-12 months in routine practice for response. With increase in number of sessions required, there is an increased cost as well. Further with a greater demand for psychological interventions for social anxiety, there is a need to identify time and cost-effective methods of this anxiety disorder. These concerns have led to the development of brief formats of CBT. The effectiveness of brief CBT with sessions ranging from 4-8 sessions has been reported in depression,[13] panic disorder,[14,15] posttraumatic stress disorder (PTSD),[16] and generalized anxiety disorder (GAD).[17] However, studies on the efficacy of brief CBT in SAD are limited, with considerable variation in methodology and duration of therapy.[18,19,20,21]
Social anxiety is emerging as a significant mental health concern in India.[22] A majority of treatment seeking individuals are young adults, employed, and face considerable distress and dysfunction due to their symptoms.[23] A few studies in the Indian setting support the effectiveness of standard CBT in SAD, using a single case design.[24] However, there is no systematic research on the efficacy of a brief format of CBT in SAD in the Indian clinical setting. Establishing the feasibility and effectiveness of a brief format of CBT in SAD would address the needs of a large number of patients who seek help, but may be unable to attend therapy over longer duration time. Further the number of patients who could benefit from such a program would be large, given the paucity of trained professionals in India.
This study is a preliminary attempt to examine the feasibility and effectiveness of a brief format of CBT based on the program described by Clark (1997) and Wells’ (1997) for SAD. The total number of sessions in this study was arrived at based on previous studies using the model proposed by.[21,25,26] It was planned that six sessions of therapy would be conducted.
MATERIALS AND METHODS
A single case design with pre–post and 1-month follow-up assessment was adopted. Seven consecutive patients, who fulfilled the DSM-IV[27] criteria for a primary diagnosis of social anxiety disorder, were included in the study. Patients were recruited from the outpatient psychiatric services of the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, India, between January 2008 and July 2008. The Institute Ethics Committee approved the study and all patients gave written informed consent to participate. Inclusion criteria were a primary diagnosis of SAD, aged between 18 and 50 years, stabilization on medication for at least 2 months period prior to entry into the study. Patients with a life time diagnosis of schizophrenia, psychosis, bipolar affective disorder, severe depressive episode with psychotic symptoms, current substance dependence (except nicotine), and/or mental retardation were excluded. Patients who had received structured psychotherapy/CBT for social anxiety in the preceding 1 year were also excluded.
Of the seven patients four were married and three were single. The mean age of the sample was 30 years (range = 21-48 years) and the mean duration of illness was 10 years (range = 3-20 years). Majority of the patients had generalized SAD (71.42%). Two participants had mild severity of SAD, three reported moderate severity and two patients had severe social anxiety. There was comorbid diagnosis of depressive disorder in two patients, one patient was also diagnosed with obsessive compulsive disorder with moderate depression, and one patient had GAD in addition to SAD. Axis II comorbidity was present in four of the seven patients, one had obsessive compulsive personality disorder and three had mixed personality disorder- Cluster C.
Procedure and materials
Clinical diagnosis of social anxiety disorder was reviewed by the first author using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) for Axis I disorders[28] and the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II) for Axis II disorders.[29]
Patients were assessed at baseline, postintervention and 1-month follow-up. The clinical global impressions (CGI) scale[30] was administered by an independent rater (SBM). The Leibowitz social anxiety scale[31] was administered by a second independent rater (PMS). Patients received 6 weekly sessions of CBT, which was carried out by the first author under the supervision of the second author (PMS), a senior clinical psychologist.
Treatment response and severity of illness was assessed using the CGI.[30] Participants who obtained a score of 1 (very much improved) or 2 (much improved) on CGI (Improvement subscale) (CGI-I) were considered as improved. Patients who obtained ratings below 2 on CGI-I were considered as not improved. Patients were considered to be completers if they attended 80% of the therapy.
The Liebowitz Social Anxiety Scale,[31] is a 24 item clinician-administered scale that assesses fear and avoidance separately as well as an overall total score and was used to assess social anxiety. The LSAS has adequate psychometric properties.
In addition, patients were also assessed on the Social Interaction Anxiety Scale-SIAS[32] a 20 item scale that assesses fear of interaction in dyads and groups and the social phobia rating scale (SPRS)[12] which consists of five rating scales assessing key components of distress, avoidance, self-consciousness, frequency of safety-seeking behaviors, and negative beliefs in recent anxiety-provoking social situations.
Fear of negative evaluation was assessed using the 12 item, self-administered, brief fear of negative evaluation scale (BFNE).[33] The scale has adequate psychometric properties and has been validated against the longer version.[34] The Beck's Depression Inventory-II-BDI- II;[36] a 21 item self-report rating scale was administered to assess severity of depression.
Treatment program
The therapeutic program (brief CBT) was developed on the basis of the cognitive behavioral intervention program for social anxiety disorder by Clark (1997) and Wells (1997). Modifications and changes were made after a careful review of the components as well as the literature on cognitive behavioral interventions for SAD. A brief version of this program has been reported in an earlier study.[21] Patients received 6 weekly individual sessions of CBT on an outpatient basis. The duration of each session was approximately 1.5 h. The components of the program included socialization to a cognitive behavioral model, modification of safety behaviors, shifting focus of attention, video feedback, verbal reattribution, and behavioral experiments. A blueprint of social anxiety and ways of dealing with possible future setbacks was discussed in the last session. Homework was assigned after every session and reviewed at the start of the next session. Written transcripts of sessions of each patient was reviewed and discussed by the supervisor in order to ensure that treatment components developed for the study were adhered to.
Statistical analysis
Data analysis included analysis of scores obtained by the seven patients on the outcome measures are baseline, post therapy and at follow-up. Clinically significant changes (50% and above) were calculated using Blanchard and Schwartz (1988) formula. Pre- and post-therapy and follow up data were used to assess the effectiveness of the therapeutic intervention.[37]

and

Using this formula the percentage of change between pre- and post-therapy points and pre to follow-up was calculated.
RESULTS AND DISCUSSION
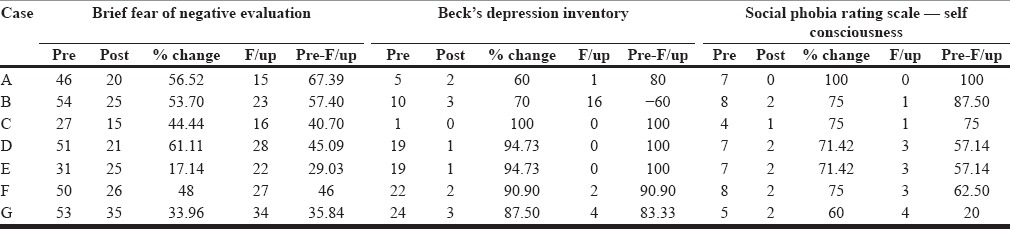
The aim of this study was to examine the feasibility and effectiveness of a brief CBT in SAD. Table 1 shows baseline, post and 1-month follow scores and percentage of improvement of the seven patients on CGI-Severity and social anxiety (LSAS-T and SIAS); Table 2 shows the results on the measures of fear and avoidance (LSAS-F, LSAS-A and SPRS-A), while Table 3 shows the results on fear of negative evaluation (BFNE), depression (BDI-II) self consciousness (SPRS-C) at baseline, post and one month follow-up.
Table 1.
Baseline, post and follow-up scores and changes on severity and social anxiety measures
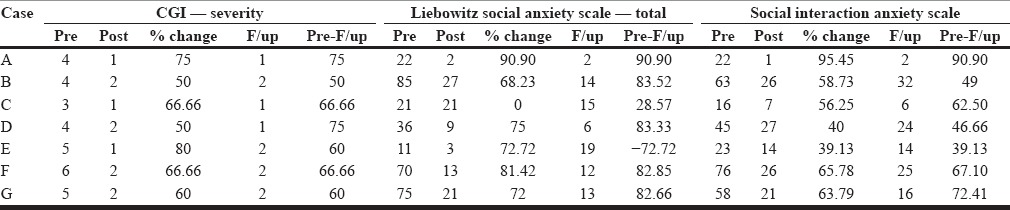
Table 2.
Baseline, post and follow up changes on fear and avoidance measures
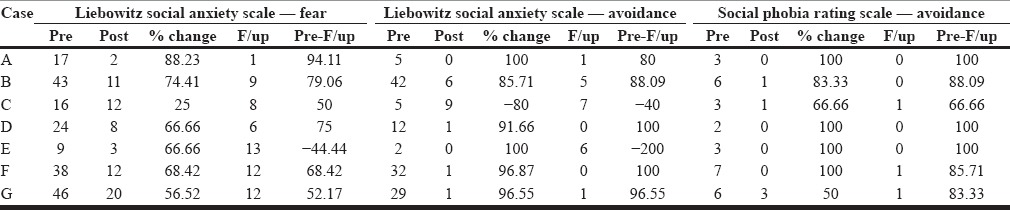
Table 3.
Baseline, post and follow up and changes on fear of negative evaluation, depression, and self-consciousness
Results indicate that brief CBT was effective in reducing social anxiety. There was a clinically significant improvement (Table 1 range = 56% to 95%) seen in four patients (patient A, B, F, and G) on all the social anxiety measures at post treatment. Clinically significant improvement was also observed for patients D and E on all the social anxiety measures (range = 66% to 75%), except on SIAS [Table 1]. In patient C no improvement was observed on LSAS-T at post treatment. In patients D and E there was an improvement of 40% and 39%, respectively, at post-treatment on SIAS and on LSAS-Fear there was a 25% improvement for patient C at post-treatment. Significant change on most of the outcome measures for all the patients suggests the effectiveness of brief CBT in reducing social anxiety at post treatment. At one month follow-up, clinically significant change was noted in all the patients, except for patient E, on most the outcome measures, indicating the maintenance of improvement in social anxiety at 1 month post-treatment.
There was also a clinically significant improvement in overall symptoms severity for all patients on CGI-severity at post-treatment and 1-month follow-up [Table 1]. Patients’ severity on CGI-S had changed from ‘mildly ill’ or ‘severely ill’ at baseline to ‘normal’ or ‘borderline mentally ill’ at both post treatment as well as follow-up.
Self-focused attention, the use of safety behaviors, anticipatory, and post-event processing,[25,38,39,40] have been identified as significant maintaing factors in SAD.
There was a clinically significant improvement on SPRS-self-consciousness for all the patients at post treatment, indicating effectiveness of brief CBT in reducing self-consciousness [Table 3]. At post-treatment, significant change was observed for all the patients on SPRS-self-consciousness, except for patient G (IP = 20), indicating the maintenance of reducing in self-consciousness at 1-month post-treatment. Self-consciousness is believed to cause and maintain social anxiety.[25] Socially anxious individuals shift their attention focus toward detailed monitoring and observation of self this tends to make them aware of arousal symptoms which in turn create further anxiety.[21] Recent literature on CBT for social anxiety provides evidence for effectiveness of video-feedback in modifying negative self-image.[40,41,42,43,44] Self-consciousness is considered to be a general marker for maladaptive beliefs and cognitive processes.[45] In this study, patients were helped to understand and identify the content of self-consciousness and were instructed to shift focus of attention to external processing and video feedback was used to bring about cognitive change. Patients reported that when in anxious situations, shifting focus of attention helped to reduce their anxiety and made them feel comfortable.
There was a clinically significant change on avoidance (Table 2, LSAS-Avoidance and SPRS-Avoidance) in all patients, except in patient C on LSAS-Avoidance, indicating the effectiveness of Brief CBT in reducing social avoidance at post treatment. At follow-up, a significant change was noted in all patients on both the measures of social avoidance (LSAS-A and SPRS-A) except for patient C and E on LSAS-Avoidance. The follow-up results support the effectiveness of brief CBT in maintaining the reduction of social avoidance at 1-month following treatment.
Patient C showed a slight deterioration on LSAS-avoidance from score 5 at baseline to score 9 at post-treatment (IP = 80%) and some improvement at follow-up (IP = 40), though not clinically significant [Table 2]. At follow-up, patient E was observed to have worsened on LSAS-avoidance from score 2 at baseline to score 6 at post-treatment [Table 2].
According to the Clark and Wells (1995) model, postevent processing is an important factor that maintains social avoidance. Socially anxious individuals often brood and experience extreme distress following social events, leading to devaluation of self, increased anticipatory anxiety for future social interaction, and likelihood of avoidance behaviors.[46] Hence, one of the treatment components targeted reduction of post-event rumination. Decrease in post-event processing may lead to the prevention of negative appraisal of the situation and self, reduction in anxiety, thereby decrease in social avoidance. In situation safety behaviors are also believed to maintain social avoidance by preventing the disconfirmation of negative beliefs.[25] In this study, patients were instructed to drop safety behaviors during the exposure tasks and this could have contributed to decrease in social avoidance. This interpretation is supported by the literature that has specifically examined the effect of exposure plus dropping safety behaviors on social anxiety and avoidance.[47] Negative prediction prior to social interaction is another cognitive factor that is believed to lead to social avoidance.[25] In this treatment program, anticipatory processes were identified and modified through verbal challenging and behavioral experiments.
There was clinically significant reduction in fear of negative evaluation for three patients (A, B and D; Table 3) at post-treatment. Four out of the seven patients (C, E, F, G) reported changes from pre- to post-treatment; however, this change was not statistically significant and ranged from 17% to 48%. At 1-month follow-up, a significant change was observed for patients A and B. Results indicate that although six sessions of brief CBT were effective in modifying dysfunctional thoughts regarding negative evaluation, it was not sufficient to produce clinically significant change in most of the patients at post assessment and one month follow-up. This suggests that modification of dysfunctional cognitions may occur with more sessions focused on cognitive change and there is a need for long-term follow-up in order to establish this. Brief CBT was found to be effective in producing clinically significant improvement in depression for all the patients at post-treatment as well as at follow-up, except for patient no B at follow-up [Table 3].
In conclusion, the results of this preliminary case series are encouraging and suggest that brief CBT can effective and in the longer term, cost effective in the management of patients with SAD. The sample was clinically representative.
The results also indicate that CBT can be abbreviated by focusing on modification of biased cognitive processes and targeting negative beliefs that maintain social anxiety. The study has certain limitations. The aim of this study was to examine the initial feasibility and results of Brief CBT in this clinical condition. However, a small sample size, single case design, and short follow up are limitations of this study. Future research should focus on evaluating the brief CBT against the standard CBT for SAD with larger samples and long-term follow-up.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- 2.Bruce SE, Yonkers KA, Otto MW, Eisen JL, Weisberg RB, Pagano M, et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: A 12-year prospective study. Am J Psychiatry. 2005;162:1179–87. doi: 10.1176/appi.ajp.162.6.1179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jørstad-Stein EC, Heimberg RG. Social phobia: An update on treatment. Psychiatr Clin North Am. 2009;32:641–63. doi: 10.1016/j.psc.2009.05.003. [DOI] [PubMed] [Google Scholar]
- 4.Rapee RM. Descriptive psychopathology of social phobia. In: Clark DM, Heimberg RG, Liebowitz MR, Hope DA, Schneier FR, editors. Social Phobia: Diagnosis, Assessment, and Treatment. New York: The Guilford Press; 1995. pp. 41–66. [Google Scholar]
- 5.Schneier FF, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia: Comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282–8. doi: 10.1001/archpsyc.1992.01820040034004. [DOI] [PubMed] [Google Scholar]
- 6.Blanco C, Schneier FR, Schmidt A, Blanco-Jerez CR, Marshall RD, Sánchez-Lacay A, et al. Pharmacological treatment of social anxiety disorder: A meta-analysis. Depress Anxiety. 2003;18:29–40. doi: 10.1002/da.10096. [DOI] [PubMed] [Google Scholar]
- 7.Feske U. Cognitive behavioral versus exposure only treatment for social treatment: A meta-analysis. Behav Ther. 1995;26:695–720. [Google Scholar]
- 8.Gould RA, Buckminster S, Pollack MH, Otto MW, Massachusetts LY. Cognitive-behavioral and pharmacological treatment for social phobia: A meta-analysis. Clin Psychol Sci Pr. 1997;4:291–306. [Google Scholar]
- 9.Gil PJ, Carrillo FX, Meca JS. Effectiveness of cognitive-behavioural treatment in social phobia: A meta-analytic review. Psychology in Spain. 2001;5:17–25. [Google Scholar]
- 10.Fedoroff IC, Taylor S. Psychological and pharmacological treatments of social phobia: A meta-analysis. J Clin Psychopharmacol. 2001;21:311–24. doi: 10.1097/00004714-200106000-00011. [DOI] [PubMed] [Google Scholar]
- 11.Liebowitz MR, Heimberg RG, Schneier FR, Hope DA, Davies S, Holt CS, et al. Cognitive-behavioral group therapy versus phenelzine in social phobia: Long-term outcome. Depress Anxiety. 1999;10:89–98. [PubMed] [Google Scholar]
- 12.Wells A. Chichester, UK: Wiley; 1997. Cognitive Therapy of Anxiety Disorders: A Practice Manual and Conceptual Guide; pp. 166–199. [Google Scholar]
- 13.Scott C, Tacchi MJ, Jones R, Scott J. Acute and one-year outcome of a randomised controlled trial of brief cognitive therapy for major depressive disorder in primary care. Br J Psychiatry. 1997;171:131–4. doi: 10.1192/bjp.171.2.131. [DOI] [PubMed] [Google Scholar]
- 14.Clark DM, Salkovskis PM, Hackmann A, Wells A, Ludgate J, Gelder M. Brief cognitive therapy for panic disorder: A randomized controlled trial. J Consult Clin Psychol. 1999;67:583–9. doi: 10.1037//0022-006x.67.4.583. [DOI] [PubMed] [Google Scholar]
- 15.Craske MG, Maidenberg E, Bystritsky A. Brief cognitive-behavioral versus nondirective therapy for panic disorder. J Behav Ther Exp Psychiatry. 1995;26:113–20. doi: 10.1016/0005-7916(95)00003-i. [DOI] [PubMed] [Google Scholar]
- 16.Foa EB, Hearst-Ikeda D, Perry KJ. Evaluation of a brief cognitive- behavioral program for the prevention of chronic PTSD in recent assault victims. J Consult Clin Psychol. 1995;63:948–55. doi: 10.1037//0022-006x.63.6.948. [DOI] [PubMed] [Google Scholar]
- 17.Power KG, Simpson RJ, Swanson V, Wallace LA. A controlled comparison of cognitive-behavior therapy, diazepam, and placebo, alone and in combination, for the treatment of generalised anxiety disorder. J Anxiety Disord. 1990;4:267–92. [Google Scholar]
- 18.Herbert JD, Rheingold AA, Goldstein SG. Brief cognitive Behavioral group therapy for social anxiety disorder. Cogn Behav Pract. 2002;9:1–8. [Google Scholar]
- 19.Mörtberg E, Clark DM, Sundin O, Aberg Wistedt A. Intensive group cognitive treatment and individual cognitive therapy vs. treatment as usual in social phobia: A randomized controlled trial. Acta Psychiatr Scand. 2007;115:142–54. doi: 10.1111/j.1600-0447.2006.00839.x. [DOI] [PubMed] [Google Scholar]
- 20.Rapee RM. Recent advances in the treatment of social phobia. Aust Psychol. 1993;28:168–71. [Google Scholar]
- 21.Wells A, Papageorgiou C. Brief cognitive therapy for social phobia: A case series. Behav Res Ther. 2001;39:713–20. doi: 10.1016/s0005-7967(00)00036-x. [DOI] [PubMed] [Google Scholar]
- 22.Shah P, Kataria L. Social phobia and its impact in Indian university students. Internet J Ment Health. 2009;6:2. [Google Scholar]
- 23.Jain M, Sudhir PM. Dimensions of perfectionism and perfectionistic self-presentation in social phobia. Asian J Psychiatr. 2010;3:216–21. doi: 10.1016/j.ajp.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 24.Gannavaram K. Cognitive behaviour therapy in social phobia. In: Shah A, Rao K, editors. Psychological Research in Mental Health and Neurosciences, 1957-2007. Bangalore: NIMHANS Publication (Deemed University); 2007. p. 46. [Google Scholar]
- 25.Clark DM. Cognitive Therapy for Social Phobia: Some Notes for Therapists. 1997 [Google Scholar]
- 26.Clark DM, Wells A. A cognitive model of social phobia. In: Hiemberg R, Liebowitz M, Hope DA, Schneier FR, editors. Social Phobia: Diagnostic Assessment and Treatment. New York: Guildford Press; 1995. pp. 69–93. [Google Scholar]
- 27.4th ed. Washington, DC: American Psychiatric Association; 1994. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. [Google Scholar]
- 28.First MB, Spitzer RL, Gibbon M. Patient ed. New York: (SCID-I/P, version 20) New York State Psychiatric Institute: Biometrics Research Group; 1995. Structured Clinical Interview for DSM-IV Axis I Disorders. [Google Scholar]
- 29.Gibbon M, Spitzer RL, Williams JB, Benjamin LS, First MB, editors. Washington, DC: American Psychiatric Press Inc; 1997. Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II) [Google Scholar]
- 30.Guy W. Rockville, Md: US Dept Health, Education, and Welfare Publication (ADM) 76-338; 1976. ECDEU Assessment Manual for Psychopharmacology. National Institute of Mental Health; pp. 218–22. [Google Scholar]
- 31.Liebowitz MR. Social phobia. Mod Probl Pharmacopsychiatry. 1987;22:141–73. doi: 10.1159/000414022. [DOI] [PubMed] [Google Scholar]
- 32.Mattick RP, Clarke JC. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav Res Ther. 1998;36:455–70. doi: 10.1016/s0005-7967(97)10031-6. [DOI] [PubMed] [Google Scholar]
- 33.Leary MR. A brief version of the fear of negative evaluation scale. Pers Soc Psychol Bull. 1983;9:371–5. [Google Scholar]
- 34.Watson D, Friend R. Measurement of social-evaluative anxiety. J Consult Clin Psychol. 1969;33:448–57. doi: 10.1037/h0027806. [DOI] [PubMed] [Google Scholar]
- 35.Baker SL, Heinrichs N, Kim HJ, Hofmann SG. The Liebowitz social anxiety scale as a self-report instrument: A preliminary psychometric analysis. Behav Res Ther. 2002;40:1087–98. doi: 10.1016/s0005-7967(01)00060-2. [DOI] [PubMed] [Google Scholar]
- 36.Beck AT, Steer RA, Brown GK. San Antonio, TX: Psychological Corporation; 1996. Manual for the Beck Depression Inventory-II. [Google Scholar]
- 37.Blanchard EB, Schwarz SP. Clinically significant changes in behavioral medicine. Behav Assess. 1988;10:171–88. [Google Scholar]
- 38.Dodge CS, Hope DA, Heimberg RG, Becker RE. Evaluation of the social interaction self-statement test with a social phobia population. Cognit Ther Res. 1988;12:211–22. [Google Scholar]
- 39.Rapee RM, Gaston JE, Abbott MJ. Testing the efficacy of theoretically derived improvements in the treatment of social phobia. J Consult Clin Psychol. 2009;77:317–27. doi: 10.1037/a0014800. [DOI] [PubMed] [Google Scholar]
- 40.Woody SR, Rodriguez BF. Self-focused attention and social anxiety in social phobics and normal controls. Cognit Ther Res. 2000;24:473–88. [Google Scholar]
- 41.Harvey AG, Clark DM, Ehlers A, Rapee RM. Social anxiety and self-impression: Cognitive preparation enhances the benefecial effects of video feedback following a stressful social task. Behav Res Ther. 2000;38:1183–92. doi: 10.1016/s0005-7967(99)00148-5. [DOI] [PubMed] [Google Scholar]
- 42.Rodebaugh TL, Rapee RM. Those who think they look worst respond best: Self-observer discrepancy predicts response to video feedback following a speech task. Cognit Ther Res. 2005;29:705–15. [Google Scholar]
- 43.McEvoy PM. Effectiveness of cognitive behavioural group therapy for social phobia in a community clinic: A benchmarking study. Behav Res Ther. 2007;45:3030–40. doi: 10.1016/j.brat.2007.08.002. [DOI] [PubMed] [Google Scholar]
- 44.Hofmann SG. Treatment of social phobia: Potential mediators and moderators. Clin Psychol (New York) 2000;7:3–16. doi: 10.1093/clipsy/7.1.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wells A, Matthews G. NJ: Lawrence Erlbaum Associates Inc; 1994. Attention and Emotion: A Clinical Perspective; p. 402. [Google Scholar]
- 46.Rapee RN, Heimberg RG. A cognitive-behavioral model of anxiety in social phobia. Behav Res Ther. 1997;35:741–56. doi: 10.1016/s0005-7967(97)00022-3. [DOI] [PubMed] [Google Scholar]
- 47.Garcia-Palacios A, Botella C. The effects of dropping in-situation safety behaviors in the treatment of social phobia. Behav Interv. 2003;18:23–33. [Google Scholar]