

Abstract
Background:
Intelligence quotient (IQ) but not the core symptoms have been known to predict outcomes in autism. Besides resource issues in India, assessing IQ in presence of autistic symptoms is challenging in general.
Materials and Methods:
In a pilot study, we explored different global indices of development in 30 children with confirmed autism. These included Wechsler intelligence scale for children or Wechsler preprimary scale of intelligence-revised (n = 10), Raven's progressive matrices (RPM) (n = 10), Vineland adaptive behavior scales II, parent report version (VABS) (n = 30) and teacher's estimate of mental age (TIQ) (n = 30). Three subgroups (Group A) with Wechsler's scales derived IQ (WISIQ), (Group B) with RPM derived IQ and (Group C) those without a formal IQ measure were compared.
Results:
All groups were comparable on age and their scores on Childhood Autism Rating Scale and Indian Scale for Assessment of Autism Adaptive behavior composite scores (Ad Bh composite) derived from VABS and WISIQ showed significant correlations with each other in Group A; TIQ significantly correlated with Ad Bh composite scores, but not with the WISIQ, although the latter two scores themselves did not significantly differ from each other. RPM consistently overestimated children's performance compared to Ad Bh composite or TIQ in Group B, but the Ad Bh composite and TIQ were themselves significantly correlated. In Group C, there were poor correlations between Ad Bh composite and TIQ. The Ad Bh composite score in this group was significantly different from the other two groups.
Conclusion:
There is a need to fine tune the assessment for global cognitive measures in autism and explore their real world importance.
Keywords: Adaptive behavior, autism, cognition, intelligence quotient
INTRODUCTION
There is no reliable index of cognitive/global functioning such as intelligence quotient (IQ) in children with autism. It has been reported that IQ and not the severity of autism related behaviors is a better predictor of outcome in children with autism. However, assessment of intelligence in autism poses numerous challenges. The nature of difficulties associated with autism (e.g., difficulties in communication) makes the use of standardized intelligence tests contentious.[1] Interpretation of success and failure on a test may be difficult as failure may be due to wrong response, refusal to respond, need for prompts, or lack of demonstration of knowledge.[2] The profile obtained on IQ tests like the Wechsler scales of intelligence is generally marked by a scatter where performance is low on verbal subtests like comprehension and high on performance subtests like block design.[3] In their study, Dawson et al. found that scores on Ravens progressive matrices (RPM), a nonverbal test of intelligence were 30-70 percentile points higher than scores on the Wechsler scales. Therefore, there is a need for a global index of functioning and more reliable and flexible means of assessment of cognitive functioning.
Adaptive behavior can be defined as the skills in conceptual, social and practical domains that an individual is able to demonstrate on a daily basis.[4] The utility of assessment of adaptive behavior in autism has been discussed in the literature. As adaptive behavior measures are usually informant based they are more feasible for assessment in presence of autism.[1] Vineland adaptive behavior scales II (VABS) has been increasingly used in the Indian context[5] and is undergoing normative compilation in our institution.[6] Apart from this, teachers who have an intimate knowledge of the child's abilities are an indispensible source of information in all clinical assessments. Using simple measures such as asking parents or teachers to guess the approximate mental age of children is part of clinical teaching in India. Such measures have not been systematically evaluated against formal measures although they often form the basis for selection in school-based epidemiological studies.[7,8] In any case, their use in the context of understanding autism has not been evident.
A variety of phenotypical assessments have been carried out as part of an ongoing database of pervasive developmental disorders within greater Bengaluru. We have obtained data on measures of adaptive behavior, intelligence, autism related behaviors and teacher's estimate of mental ages of children. In this study, we present data on 30 children in an effort to explore the utility of some of these measures to describe the overall cognitive development in children with autism. This work has been approved by St. John's Medical College, Institutional Ethics committee.
In brief, this study aims to highlight the challenges of assessing IQ in children with autism and explore the relationship between adaptive behavior and IQ. If this relationship is strong, then adaptive behavior as reported by parents may be potentially used in lieu of IQ. We also wished to explore how teacher's estimate of mental age of children with autism compares with other formal scaled measures available such as IQ and adaptive behavior.
MATERIALS AND METHODS
Thirty children who were diagnosed to have autism by two clinicians as per Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria and who were part of a larger database compiled by the Department of Psychiatry, St John's Medical College Hospital were taken for the study. The selection was dependent upon availability of all measures, especially the teacher estimated measure (TIQ).
The children were divided into three Groups A, B, and C depending on their amenability for assessment. Children who were co-operative and had sufficient verbal abilities were included in Group A and IQ was measured using the Wechsler's Scales (WISIQ) (n = 10). Children who were primarily nonverbal were included in Group B and IQ was measured using RPM (n = 10). Group C consisted of children on whom any form of IQ assessment was not feasible and hence did not have a formal IQ measure (n = 10). VABS was rated by parents of all the children, with clinician's assistance (Pavana A Rao). Childhood Autism Rating Scale (CARS) and Indian Scale for Assessment of Autism (ISAA) were administered to the parents. Direct observations as suggested in the respective manuals was also used to score these measures. We have used the adaptive behavior composite scores (Ad Bh composite) for our purposes here as this represents a global measure. Teachers’ estimate of intelligence was calculated for all the groups, in terms of their best estimate of current mental age in months. Teachers had at least a year's knowledge of the respective children. The details of assessments done can be seen in Table 1.
Table 1.
Details of assessments done

Statistical analysis
In view of the small sample and nonnormality, all data are presented as median and interquartile range. The test scores/scaled measures were compared between the three groups using Kruskal–Wallis test. The WISIQ estimates and adaptive behavior scores were compared between Groups A and B using Mann–Whitney U-test. The scores obtained on two tests within a group were compared using Wilcoxon sign rank test. The association between adaptive behavior and IQ within groups was assessed using Spearman's rank order correlation. All analysis was performed using IBM Statistical Package for the Social Sciences version 20. Statistical significance was considered at P < 0.05.
RESULTS
The median ages of the children were 8, 9, and 11 years in Groups A, B, and C respectively, but the difference was not statistically significant [Table 2]. On the Kruskal–Wallis test, the TIQ and Ad Bh composite scores were significantly different between the three groups (P = 0.023 and P = 0.01, respectively). All the other test scores were comparable across the groups.
Table 2.
Descriptive statistics for Groups A, B, C for all measures

In Group A, the Ad Bh composite correlated with both WISIQ and TIQ [Table 3, P = 0.68 and P = 0.69]. However, WISIQ estimate and TIQ were not correlated. This may perhaps be explained by limited sample size. There was no significant difference between WISIQ and TIQ. In Group B, Ad Bh composite was correlated with TIQ alone and the RPM derived IQ (RPMIQ) differed from that of Ad Bh composite and TIQ. In Group C where any formal measure of IQ could not be administered, TIQ and Ad Bh composite were not correlated (P = 0.101, P < 0.781). In fact, the Ad Bh composite tended to be higher compared to TIQ in Group C [P = 0.059, Figure 1].
Table 3.
Correlation and difference in IQ estimates from different tests within Groups A and B

Figure 1.

Comparison of adaptive behavior scores and teachers intelligence quotient in Group C
Though Groups A and B are comparable on TIQ and Ad Bh composite, they are significantly different on the formal IQ measure. The IQ estimate from RPM was significantly higher in Group B compared to WISIQ in Group A, while TIQ and Ad Bh composite were not different between the groups [Figure 2].
Figure 2.
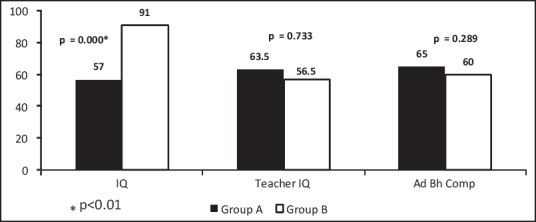
Comparison of Raven's progressive matrices derived intelligence quotient (IQ) and Wechsler's scales derived IQ, teachers IQ and Vineland adaptive behavior scales based adaptive behavior composite scores between Groups A and B
DISCUSSION
The results reveal that the three groups are comparable on age and autism severity. There was no significant difference between Groups A and B in their level of adaptive behaviors, symptomatology and estimate of intelligence by teachers, while there was a significant difference in IQ scores. Even within Group B, RPMIQ differed significantly from TIQ and Ad Bh composite, which were themselves not significantly different. Dawson et al.[3] have shown that RPM overestimates IQ in the same children compared to Wechsler's scales. As there is convergence between adaptive behavior measure and teacher's estimates in Group A, if we keep such measures as a reliable indicator of global intelligence, then our findings also suggest that RPM may be overestimating the intelligence, unlike WISIQ (where feasible).
In Groups A and B where different ways of assessing intelligence was possible, it was observed that adaptive behavior scores and teachers estimate of intelligence were higher when compared with Group C, where assessment of IQ was not feasible. Further, it was noted that in Group C the teachers estimate differed significantly from the Ad Bh composite score. The results seem to suggest that teachers IQ may be a potential alternative option for the global measure of cognition in those children who have attained a particular level of adaptive behavior skills. This may find a use in epidemiological studies. On the other hand, in such children where adaptive behavior is better, and some formal IQ assay is possible, the need for teacher's estimate may not be felt clinically necessary. Given the wide experience that teachers have with children, it may be then more useful to have a more formal measure from teacher, for example, the teacher's version of the VABS. It may be worthwhile exploring the utility of the teacher's report on VABS.
The difficulties in determining IQ in presence of autism have been highlighted in our study. It was observed that the focus on the known strengths in visuo-spatial skills in these children may end up overestimating their IQ scores as seen by the IQ scores on RPM. No single global measure of cognition/ability/functioning appears to perform consistently across varied cognitive capabilities. When possible to carry it out reliably, it has been reported that IQ and adaptive behavior are seen to have a strong correlation where cognitive functioning is low (IQ <70).[10] Another study however has found that adaptive measures correlate better with IQ in higher functioning children.[11] The measure of adaptive behaviors with adequate norms and standardization is thus emerging as a reliable alternative. Using such measures from both teachers and parents needs further exploration. Supplementary norms for children with autism on the Vineland scales has been reported.[12] Such an exercise in the Indian context may be conceptualized after clear norms for children in general are available. This latter exercise is underway in our center.[6] Apart from such a measure, given the increase in reports of comfort with a tablet computer based activities in children with autism, the use of tablet based assessment tools may also prove useful. Such methods remain largely unexplored.
Challenges in assessment
There are definite difficulties in the use of standardized intelligence tests due to limitations in verbal communication and problems with social interaction. Associated problems in autism like hyperactivity make the administration of tests difficult and sometimes not feasible. A wide scatter in the profiles on Wechsler scales was seen revealing the drawbacks of using this measure. Further, it is difficult to adhere to prescribed time limits and instructions for the tests, and this raises the question of reliability of obtained scores. For many children, it was not possible to assess IQ using either the Wechsler's scales or the RPM.
SUMMARY AND CONCLUSION
We have explored different forms of global indices to describe functioning/ability in autism. A global index can provide a clinically heuristic measure. This can help in discussing prognosis and making overall sense of the clinical issues. Adaptive behaviors as rated by parents show some degree of promise in this regard, while direct clinical assessments available today are likely to remain of uncertain relevance. We are exploring if teacher reported measures of adaptive behaviors can improve their general estimate of these children's ability. Our report needs further support from larger multi-centric samples.
Footnotes
Source of Support: St. John's Medical College Research Society
Conflict of Interest: None declared.
REFERENCES
- 1.Wells K, Condillac RA, Perry A, Factor DC. Comparison of three adaptive behaviour measures in autism in relation to cognitive level and severity of autism. J Dev Disabil. 2009;15:55–63. [Google Scholar]
- 2.Eagle RS. Accessing and assessing intelligence in individuals with lower functioning autism. J Dev Disabil. 2002;9:45–53. [Google Scholar]
- 3.Dawson M, Soulières I, Gernsbacher MA, Mottron L. The level and nature of autistic intelligence. Psychol Sci. 2007;18:657–62. doi: 10.1111/j.1467-9280.2007.01954.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Washington, DC: American Association on Mental Retardation; 2002. American Association on Mental Retardation. Mental Retardation. Definition, Classification and Systems of Supports. [Google Scholar]
- 5.Manohari SM, Raman V, Ashok MV. Use of Vineland adaptive behavior scales – II in children with autism – An Indian experience. J Indian Assoc Child Adolesc Ment Health. 2013;9:5–12. [Google Scholar]
- 6.Selvam S, Jianjun Z, Thomas T, Shetty P, Raman V, Khanna D, Mehra R, Kurpad AV, Srinivasan K. Being submitted for publication; Personal Communication first author; Norms for developmental milestones and its association with anthropometric measures among preschool children in Urban South India. [Google Scholar]
- 7.Emerson E, Hatton C. The mental health of children and adolescents with learning disabilities in Britain. Adv Ment Health Learn Disabil. 2007;1:62–3. [Google Scholar]
- 8.Malhi P, Kashyap S, Dua S. Maternal estimates of mental age in developmental assessment. Indian J Pediatr. 2005;72:931–4. doi: 10.1007/BF02731666. [DOI] [PubMed] [Google Scholar]
- 9.Reynolds CR, Fletcher JE, editors. 3rd ed. New York, USA: Springer Science + Business Media; 2009. Handbook of Clinical Child Neuropsychology. [Google Scholar]
- 10.Bölte S, Poustka F. The relation between general cognitive level and adaptive behavior domains in individuals with autism with and without co-morbid mental retardation. Child Psychiatry Hum Dev. 2002;33:165–72. doi: 10.1023/a:1020734325815. [DOI] [PubMed] [Google Scholar]
- 11.Kenworthy L, Case L, Harms MB, Martin A, Wallace GL. Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. J Autism Dev Disord. 2010;40:416–23. doi: 10.1007/s10803-009-0911-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Carter AS, Volkmar FR, Sparrow SS, Wang JJ, Lord C, Dawson G, et al. The Vineland adaptive behavior scales: supplementary norms for individuals with autism. J Autism Dev Disord. 1998;28:287–302. doi: 10.1023/a:1026056518470. [DOI] [PubMed] [Google Scholar]