

Abstract
Introduction
There are numerous genital complaints in women cyclists, including pain, numbness and edema of pelvic floor structures. Debate ensues about the best saddle design for protection of the pelvic floor.
Aim
To investigate the relationships between saddle design, seat pressures and genital nerve function in female, competitive cyclists.
Methods
We previously compared genital sensation in healthy, premenopausal, competitive women bicyclists and runners. The 48 cyclists from our original study comprise the study group in this sub-analysis.
Main Outcome Measures
(1) Genital vibratory thresholds (VT) were determined using the Medoc Vibratory Sensation Analyzer 3000. (2) Saddle pressures as determined using a specially designed map sensor.
Results
More than half of the participants (54.8%) used traditional saddles and the remainder (45.2%), rode with cut-out saddles. On bivariate analysis, use of traditional saddles was associated with lower mean perineal saddle pressures (MPSP) than riding on cut-out saddles. Peak perineal saddle pressures (PPSP) were also lower; however, the difference did not reach statistical significance. Saddle design did not affect mean or peak total saddle pressures (MTSP, PTSP). Saddle width was significantly associated with PPSP, MTSP and PTSP, but not with MPSP. Women riding cut-out saddles had, on average, a 4 and 11 kPa increase in MPSP and PPSP, respectively, compared to women using traditional saddles (p= 0.008 and p= 0.010), after adjustment for other variables. Use of wider saddles was associated with lower PPSP and MTSP after adjustment. Although an inverse correlation was seen between saddle pressures and VTs on bivariate analysis, these differences were not significant after adjusting for age.
Conclusion
Cut-out and narrower saddles negatively affect saddle pressures in female cyclists. Effects of saddle design on pudendal nerve sensory function were not apparent in this cross-sectional analysis. Longitudinal studies evaluating the long-term effects of saddle pressure on the integrity of the pudendal nerve, pelvic floor and sexual function are warranted.
Keywords: saddle design, saddle pressures, pudendal nerve
Introduction
Bicycle riding is a popular activity, commonly used for transportation, recreation and exercise. Both health and quality of life benefits have been reported in riders (1,2). Bicycle riding, notwithstanding its known benefits, is also associated with a number of health risks including orthopedic injuries, pelvic neurovascular compromise and erectile dysfunction (ED)(3-9).
Soloman and Cappa were the first to report the association between perineal pain, decreased pudendal sensation and transient ED in a case study involving a male subject exercising on a stationary bike (3). Desai et al. confirmed similar findings in a young male patient, unaccustomed to long distance riding, who presented with ED following a two-day bike race (4). Several observational studies have also substantiated these results (5-9). It is believed that the underlying pathology of ED in male cyclists, results from compression of the pudendal neurovascular bundle against the saddle while riding (6-9).
Although the exact cause of ED resulting from bicycle riding is not known, several studies support the supposition that nerve and vascular compression during riding play a role. Evaluating 40 healthy males, Sommer et al. noted a sharp decrease in penile O2 pressure within 5 minutes after transitioning from a standing to a seated position during cycling (9). In a subsequent study, evaluating the effect of different saddle designs on oxygen pressure, these same authors noted a decrease in pressure with all saddle types; however, use of wider saddles seemed to decrease pressure to a greater extent (10). To date, no studies have evaluated the associations between saddle design, seat pressures and neurovascular compromise in women.
In a prior study, our group evaluated neurological function in female cyclists (11). We identified significant decreases in pudendal nerve sensory function in women cyclists compared to runners. These findings suggest that, similar to men, women cyclists suffer from compression injuries that compromise normal function of the pudendal neurovascular bundle.
Aims
This study was conducted to investigate the relationships between saddle design, seat pressure and genital nerve function in female competitive cyclists, using data collected previously on the original group of 48 cyclists.
Methods
Recruitment
In 2003, we enrolled 48 cyclists and 22 runners in a cross-sectional study evaluating the effects of bicycle riding on the female pelvic floor. This paper focuses on the 48 cyclists from the original sample. After receiving investigational review board approval, all premenopausal, English-speaking women bicyclists who rode on average, at least 10 miles per week, 4 weeks per month were considered for participation. Exclusion criteria included women with central or peripheral neurological deficits as well any diseases that could cause neuropathy, such as a prior cerebral vascular accident, diabetes mellitus, or HIV/ AIDS. Women with hypertension requiring medications, or active vulvar lesions were also excluded from participation. Interested participants were prescreened through a telephone interview and written informed consent was obtained prior to enrollment. Detailed information about the study methods have been previously published (11).
Medical and Bicycling History Evaluation
Information about subjects’ medical, surgical, and biking histories was obtained by interview as well as questionnaires (11). The Reproductive History Questionnaire included questions about prior gynecologic surgeries and genital injuries and the Bicycling History Questionnaire inquired about bicycle specifications, saddle design and bicycle habits, as well as previous bicycling injuries, and bicycling-related neurological symptoms. All questionnaires were randomly distributed to participants to avoid order bias (11).
Neurological Assessment
Biothesiometry was performed, using the Medoc Model Vibratory Sensory Analyzer 3000 (VSA, Advanced Medical Systems, Ramat Yishai, Israel) to measure vibratory thresholds (VT). Sensory testing was performed on the clitoris, right and left perineum, distal anterior and posterior vagina, right and left labia majora, and external urethra meatus, known regions of pudendal nerve innervation. (11). The patients were in the lithotomy position and blinded to the voltage of the instrument being applied. The probe of the mounted VSA was placed flush against the designated skin regions, using the minimal pressure necessary to maintain the positioning. A computerized program was used to gradually increase the stimulus intensity of the probe until the participant clicked on a hand-held Patient Response Unit to indicate when the vibratory sensation was first noted. This response amplitude was recorded in microns and defined as the VT, the minimal energy needed to distinguish between vibration and static. Ascending VTs were chosen to evaluate neurological function because this method was found to have better reliability, validity, and reproducibility than other modalities (12). The test was repeated six times at each site, with a 4-second intermission between each cycle, in order to improve statistical accuracy.
Saddle design, seat width and saddle pressure measurements
Subjects were asked to bring the bicycle and saddle that they routinely rode, to the evaluation site. The saddles were classified into 2 main subtypes designated as “traditional” and “cut-out.” Traditional saddles included solid saddles that tapered to form a nose anteriorly, while nosed saddles in which a portion of the center section of the saddle was completely removed were classified as cut-out. (Figure 1).
Figure 1.
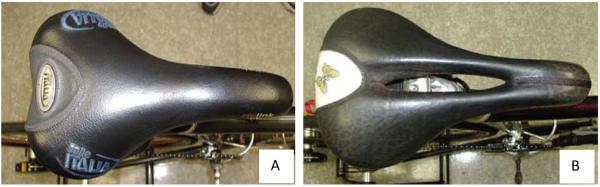
Two examples of saddles used by the riders; (A) Traditional saddle; (B) cut-out saddle
Photo images and saddle lengths were obtained for each of the saddles. The digital photo of the saddle was used to determine the ratio of the saddle width to saddle length. The saddle width was derived by multiplying the actual length of the saddle, measured by the investigators with a ruler, by the calculated width to length ratio.
Saddle pressure measurements were made using a pressure map employing the Novel Pliance pressure sensor system (Novel Electronics Inc., St. Paul, MN). The map consists of a 16 × 16 matrix of square sensing elements, each of which was 1.25 cm × 1.25 cm), yielding a total of 256 sensors (Fig. 1A). The bicycle saddle map was calibrated to 300 kPa (30 N/cm2).
Saddle pressure distributions were evaluated with cyclists using their own saddle and pedaling on their own bicycle and subjects were asked to position their saddles and handlebars in the typical position used for riding. Their bicycle was mounted in a rear-wheel supported magnetic resistance cycling trainer (Minoura “MagTurbo”; Minoura Co., Ltd., Hayward, CA). A moderate pedaling resistance was set and subjects were instructed to pedal at a comfortable cadence. Pedaling cadence, resistance, and thus power output were not controlled. As the cyclists pedaled on their mounted bicycles, pressures on the saddle were measured by the Novel system for 40-60 s at a sampling frequency of 20 Hz. The pressure time series for each individual sensor was low-pass filtered (5-Hz cut-off) before the pressure summary measures were calculated. All recorded pressures were analyzed using custom software written in Labview (National Instruments, Austin, TX).
Mean total and peak total saddle pressures were calculated by determining the average of all sensors recording pressure over the entire saddle over the recording period and the value for the individual sensor exhibiting the highest pressure averaged over the recording period. Perineal pressure determinations were made by identifying a region of interest assumed to correspond spatially to the cyclists perineum. This method was described in previous work (13) and was based on identifying high localized pressure landmarks associated with the ischial tuberoscities, and projecting a rectangular region anteriorly from the segment connecting the two ischial peaks in the pressure distribution. This rectangular region had a width of six sensors (7.5 cm) and was projected to the front of the pressure map. Only sensors registering non-zero pressure were included in the calculation of average pressure over the region. The average pressure of all of the sensors registering pressure in the perineum was used to calculate the mean perineal pressure. The pressure registered by the individual sensor exhibiting the highest average pressure within the perineal region was used to calculate the peak perineal pressure.
Saddle pressure calculations over a region (full saddle or perineal region) were made using the following equation:
where pij is the pressure on the sensor in row i, column j of the region, n is the number of sensors in the region registering nonzero pressure, and a is the area of an individual sensor (1.56 cm 2) (13).
Statistical Analysis
Statistical analyses were conducted using Stata 11 (StataCorp, College Station, TX) and Microsoft Excel 2007. For our initial study, questionnaires and biothesiometry data were entered with verification and variables were examined for implausible values and departures from normality (11).
While vibratory thresholds were the primary outcome of interest, factors that affect saddle pressure were also of interest and so a preliminary sub-analysis of saddle pressure as the outcome was conducted in tandem. Bivariate linear regression analysis was performed to assess relationships between biothesiometry medians, saddle pressure measures saddle characteristics as well as ride/rider characteristics. Multiplicative interaction was evaluated for models with VT and saddle pressures as the outcome and there were no significant interactions between the predictor variables. When evaluating the models using regression diagnostics, it was noted that eight observations deviated noticeably from the mean and these outliers exerted noticeable influence on the models. Investigators used 3 standard deviations above or below the mean as the cut-off to define outlying observations for separate analyses with outliers both “in” and “out” of the models. After removal from the model, the variable was re-evaluated and the model building process was repeated without those observations included in their respective variables.
Multivariable models were developed for the primary outcomes of interest, saddle pressures and genital sensation as measured by biothesiometry generated vibratory thresholds (VTs). The saddle pressure variables were also candidate predictors in the models for VTs. Based on the literature and using the analogous condition of carpal tunnel syndrome, other predictor variables that could account for degree of neurovascular compression or compromise, were also evaluated. The predictor variables included: age and BMI, as well as, saddle type and seat width. The number of hours (hours rode/ week) and distance (miles rode/ week) ridden per week were also included as predictor variables for genital sensation. However, these factors were not thought to influence the saddle pressures that were obtained and thus were excluded from these models. Forward stepwise selection of independent variables was conducted and only variables that were statistically significant (p<0.05) using two-tailed tests were retained in the final models.
Regression diagnostics were performed on bivariate and multivariable analyses to verify that the models did not violate linear regression assumptions. Bivariate models were evaluated using Box-Cox and log transformations due to concerns about normal distribution; the results obtained from the transformed and untransformed models were comparable. Similarly, due to concerns that some of the models had issues with the assumption of constant variance, the ordinary least squares (OLS) model was compared to the variance weighted least squares (VWLS) model and the results were equivalent. Similarly, kernel density plots showed that the outcome variables in the multivariable models displayed normally distributed form. In addition, Components-Plus-Residuals (CPR) plots showed a linear trend in the residuals of the models. As a further evaluative measure, the multivariable models were also log-transformed. After comparing the untransformed models with the log-transformed models, there were no substantial changes between the models. Therefore, in order to maintain interpretability, results from the untransformed models are reported.
Main Outcome Measures
Our primary outcome was genital VT determined by biothesiometry. The secondary outcome measure was saddle pressures as determined using the specially designed map employing the Novel Pliance pressure sensor system. All outcome measures were compared between bicyclists riding traditional and cut-out saddles. The effect of saddle width on the primary and secondary outcomes was evaluated using saddle width as a continuous variable.
Results
The baseline characteristics of the riders are provided in Table 1. The majority of the participants (54.8 %) used a traditional saddle, however, a higher than expected number of women cyclists (45.2 %) rode with cut-out saddles. Since 6 cyclists were missing saddle pressure values, the baseline characteristics of the riders were evaluated with those six women included and excluded from the analysis. There were no significant differences in the baseline characteristics between the women with and without saddle pressure values (data not shown).
Table 1.
Rider Demographics and Cycling Characteristics
| Variable | N | Mean ± SD or % |
|---|---|---|
| Age | 48 | 35.98 ± 6.90 |
| BMI | 48 | 22.55 ± 3.15 |
| Saddle Width | 42 | 5.81 ± 0.57 |
| Hours/week | 48 | 8.31 ± 5.97 |
| Miles/week | 48 | 99.24 ± 74.11 |
| Years riding | 48 | 8.02 ± 6.78 |
| Saddle Type | ||
| Traditional | 23 | 54.76 |
| Cut-out | 19 | 45.24 |
| Saddle Pressures | ||
| Mean Perineum | 42 | 18.90 ± 6.58 |
| Peak Perineum | 42 | 57.48 ± 19.83 |
| Mean Total | 42 | 15.18 ± 3.43 |
| Peak Total | 42 | 66.05 ± 21.55 |
| Vibratory Thresholds | ||
| Right Vulva | 46 | 3.72 ± 3.84 |
| Left Vulva | 46 | 3.52 ± 4.00 |
| Anterior Vagina | 48 | 2.84 ± 2.27 |
| Posterior Vagina | 48 | 2.78 ± 3.67 |
| Clitoris | 47 | 1.46 ± 1.02 |
| Left labia | 46 | 2.58 ± 1.93 |
| Right Labia | 48 | 3.53 ± 4.55 |
| Urethra | 48 | 3.11 ± 3.09 |
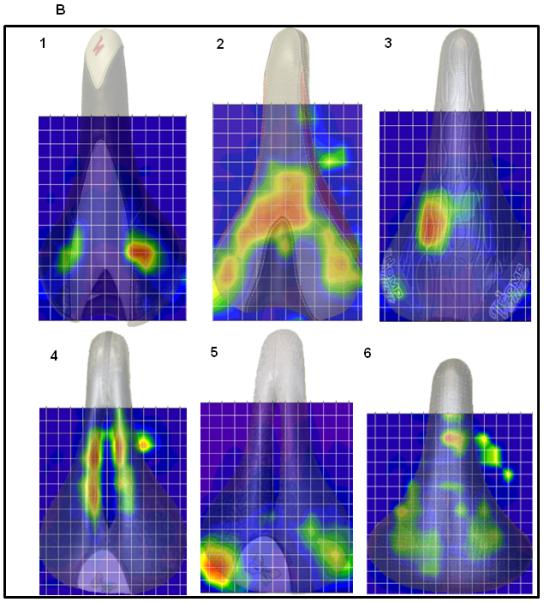
Reconstructed digital images of the saddle maps overlying the saddles were used to qualitatively assess riding patterns (Fig.2). These images showed that variable pressure distributions were seen for women riding with traditional saddles, with three primary patterns emerging (Fig. 2B. 1-3): 1. pressure over the bilateral ischial tuberosities; 2. pressure more widely distributed along the posterior saddle and ischial tuberosities; 3. pressure isolated to the perineal region. In contrast, for 80% of the women using a cut-out saddle, the highest pressures were in the perineal region, along the edges of the cut-out (Fig. 2B.4). Pressure was concentrated over the bilateral ischial tuberosities for the remaining subjects who rode with cut-out saddles (Fig. 2B.5). For a single rider with the widest saddle, low pressures were distributed across the entire saddle (Fig. 2B.6).
Figure 2.
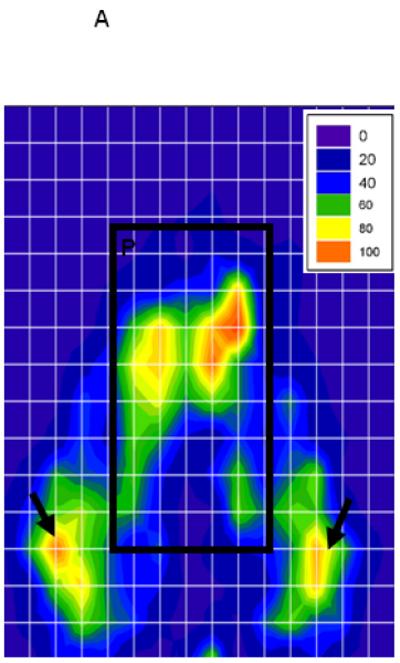
A. Representative image of the Pliance pressure map digital output after a typical riding session with a pressure scale in the upper right corner. Arrows indicate the presumed location of the ischial tuberosity pressure points. P designates the perineal region of the saddle. Pressure gradients are stratified by color maps representing scaled differences in pressure recorded in mmHg (12).
B. Reconstructed digital images of the saddles maps for women riding traditional (1-3,5) and cut-out (4-5) saddles using 2-dimentional overlays of rider saddles. 1. Pressure isolated to the bilateral ischial tuberosities (n =5); 2. Pressure more widely distributed along the posterior saddle and ischial tuberoscities (n=11); 3. Pressure isolated to the perineum (n=4); 4. Cut-out saddle with pressure in the perineal region, along the edges of the cut-out( n=15); 5. Cut-out saddle with pressure isolated to the bilateral ischial tuberosities (n=4). 6. Single wide saddle showing low pressure evenly distributed over the entire saddle (n =1);
Bivariate regression models for perineal and total saddle pressures are displayed in Table 2. Mean perineal saddle pressures were significantly lower in women riding with traditional saddles compared to women using cut-out saddles. Peak perineal saddle pressures were also lower for women using traditional saddles, although the difference did not reach statistical significance. An inverse relationship was seen between saddle widths and peak perineal saddle pressure as well as mean and peak total saddle pressures; increasing saddle widths were associated with decreasing saddle pressures. A significant negative association between age and mean and peak perineal saddle pressure, and a significant positive association between BMI and mean total saddle pressure were also noted.
Table 2.
Bivariate Regression Models of Saddle Pressures
| Saddle Pressures: Perineum | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Peak | |||||||
| N | Coef. | P<0.05 | 95% C.I. | N | Coef. | P<0.05 | 95% C.I. | |
| Age | 41 | −0.38 | 0.004* | −0.63,−0.13 | 41 | −0.74 | 0.026* | −1.38, −0.09 |
| BMI | 40 | 0.63 | 0.109 | −0.15, 1.41 | 40 | −0.19 | 0.853 | −2.20,1.83 |
| Traditional Saddle |
41 | −4.98 | 0.006* | −8.41,−1.54 | 41 | −6.64 | 0.148 | −15.74, 2.47 |
| Saddle Width |
41 | −0.63 | 0.704 | −3.93,2.68 | 41 | −8.86 | 0.024* | −16.51, −1.20 |
| Hours rode/ week |
40 | 0.149 | 0.518 | −0.31,0.61 | 40 | 0.57* | 0.316 | −0.57,1.71 |
| Miles rode/ week |
40 | 0.023 | 0.191 | −0.01,0.06 | 40 | 0.05 | 0.268 | −0.04, 0.13 |
| Saddle Pressures: Total | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Peak | |||||||
| N | Coef. | P<0.05 | 95% C.I. | N | Coef. | P<0.05 | 95% C.I. | |
| Age | 41 | −0.07 | 0.264 | −0.21,0.06 | 41 | −0.51 | 0.217 | −1.34,0.31 |
| BMI | 41 | 0.56 | 0.003* | 0.21,0.91 | 40 | 0.67 | 0.583 | −1.78, 3.12 |
| Traditional saddle |
41 | −0.57 | 0.535 | −2.40,1.27 | 41 | 0.15 | 0.979 | −11.36,11.66 |
| Saddle Width |
41 | −2.38 | 0.002* | −3.80, −0.97 | 41 | −11.29 | 0.019* | −20.66, −1.92 |
| Hours rode/ week |
39 | 0.15 | 0.118 | −0.04,0.33 | 40 | 1.08 | 0.117 | −0.29,2.45 |
| Miles rode/ week |
40 | 0.01 | 0.172 | <-0.00,0.03 | 40 | 0.07 | 0.217 | −0.04, 0.17 |
Model is significant at p <0.05
Analysis excludes outliers
Results from the multivariable models of mean and peak perineal and total saddle pressures and rider and bicycle characteristics are presented in Tables 3 and 4. Women riding cut-out saddles had, on average, a 4 and 11 kPa increase in mean and peak perineal saddle pressures, respectively, when compared to women using traditional saddles (p= 0.008 and p= 0.010, respectively), after adjustment for other variables. Saddle width was significantly associated with peak perineal and mean total saddle pressures, but not with mean perineal or peak total saddle pressures afteradjustment. Aging conferred a protective effect on mean perineal saddle pressure, while BMI was directly and significantly associated with mean total saddle pressure. There were no predictor variables for peak total saddle pressure.
Table 3.
Multivariable Regression Model of Mean and Peak Perineal Saddle Pressure
|
Final Model for Mean Perineal Saddle Pressure (F(2 , 38) = 9.51 , R2 = 0.3335, N=41) | ||
|---|---|---|
| Predictor Variable | Coef. (95% CI) | P value |
| Age | −0.34(−0.57, −0.11) | 0.005 |
| Traditional saddle | −4.41 (−7.57, −1.25) | 0.008 |
|
Final Model for Peak Perineal Saddle Pressure (F(2, 39) = 6.80 , R2 = 0.2636, N=41) | ||
|---|---|---|
| Predictor Variable | Coef. (95% CI) | P>/t/ |
| Saddle Width | −12.36(−19.04, −4.77) | 0.002 |
| Traditional saddle | −11.54(−20.22, −2.86) | 0.010 |
Analysis excludes outliers
Table 4.
Multivariable Regression Model of Mean Total Saddle Pressure
|
Final Model for Mean Total Saddle Pressure (F(3 , 37) = 24.53 , R2 = 0.6654, N=41) | ||
|---|---|---|
| Predictor Variable | Coef. (95% CI) | P>/t/ |
| BMI | 0.56(0.27, 0.86) | <0.000 |
| Saddle Width | −2.41(−3.62, −1.19) | <0.000 |
Analysis excludes outliers
Bivariate regression evaluation of genital sensation, demonstrated a negative association between mean perineal saddle pressure and VT in the vagina and urethra, indicating that increasing saddle pressures are associated with decreasing VT or improved neurological sensation (Table 5). Consistent with our previous findings, we also noted a positive association between age and vibratory thresholds (increasing age is associated with decreasing sensation- higher thresholds). After adjusting for age, the association between mean perineal saddle pressure and VT was no longer significant (data not shown).
Table 5.
Bivariate Regression Models of Biothesiometry
| VT Variable | N | Coef. | P<0.05 | 95% C.I. |
|---|---|---|---|---|
| Right Vulva | ||||
| BMI | 43 | −0.40 | 0.034 | −0.76, −0.03 |
| Vaginal Anterior | ||||
| Age | 48 | 0.151* | 0.001 | 0.064, 0.237 |
| Mean Perineum SP | 41 | −0.151* | 0.017 | −0.27, −0.029 |
| Vaginal Posterior | ||||
| Age | 48 | 0.197* | 0.010 | 0.051, 0.344 |
| Urethra | ||||
| Age | 48 | 0.175* | 0.006 | 0.053, 0.298 |
| Mean Perineum SP | 41 | −0.194* | 0.026 | −0.363, −0.024 |
Model is significant at p <0.05
Analysis excludes outliers
SP- Saddle Pressure
Importantly, our analyses were conducted with outliers “in” and “out”. Two women whose pressure values were above 3 standard deviations from the mean were excluded in the analysis with outliers “out”. One outlier was a woman whose mean and peak perineal pressures were more than 4 standard deviations above the mean. Additionally, both her peak perineum and peak total saddle pressures carried the same value, suggesting that there was an error in recording. The second outlier was obese and as such, her BMI was significantly higher than the other riders, which could have accounted for her higher saddle pressures. In the final saddle pressure regression models, the significant association between BMI and mean perineal saddle pressure (p = 0.03) was the only outcome that was affected, as BMI was no longer significantly associated with mean perineal saddle pressure when these two outliers were “out.” Similarly, two women were excluded because their right vulvar vibratory thresholds were greater than 3 standard deviations above the mean. One of the women was the oldest in the group. Still all of her other neurological findings were within the range of the other riders. The second woman had no other distinguishing characteristics and also had VT at the other sites, within the normal range. In the model with these two women “in” age was significantly, associated with vibratory thresholds; However, this association was no longer significant when they were removed. For both the saddle pressure and VT models, the outliers appeared to drive the significance and issues with variance were resolved when outliers these two outliers were “out”. Given this, we suspect that the exclusion of the outliers provides a more accurate account of findings among typical competitive cyclists. Results with outliers “out” are, therefore, presented in Tables 2-5.
Discussion
Recent reports of potential neurovascular compression injuries that can occur with cycling have resulted in a plethora of new saddles designed and marketed for women cyclists. One commonly advertised saddle is the cut-out, which has gained widespread popularity and was used by more than 45% of the women in our study. Notwithstanding the strategic marketing, limited studies including female cyclists have failed to elucidate a protective effect for women using these saddles.
Carpes et al. measured saddle pressures in both male and female recreational cyclists peddling on road bicycles with their trunks held static at 60° or 90° from the horizontal. (14) They found no differences in saddle pressures, regardless of which trunk position was assumed by the female riders. This was true of riders using both traditional and cut-out saddles; however a direct comparison between those riding traditional versus cut-out saddles was not reported. In a subsequent study, the authors compared the saddle pressures of the women using cut-out saddles to those using a gel cushioned, solid-nosed saddles and found that at a fixed workload of 150W, peak total saddle pressures were significantly increased when riding on a cut-out saddle compared to a traditional saddle (15).
Total saddle pressure also increased in women riding on a cut-out saddle in our study, although the difference did not reach statistical significance. It is interesting to note however, that by using the ischial tuberosities for spatial orientation, we found significantly higher pressures in the perineal region in women riding on cut-out saddles. Our finding showed that after adjusting for age, women riding with cut-out saddles had, on average, a 4 kPa increase in mean perineal saddle pressures and, on average, an 11 kPa increase in peak perineal saddle pressures compared to women riding with traditional saddles.
It is not surprising that perineal pressures are differentially altered in women riding with cut out saddles compared to traditional saddles. Froböse et al showed that the highest pressures are generated along the edges of the hole in women using cut-out saddles (16). Our reconstructed images also suggest that in the majority of women riding on cut-out saddles the highest pressures were in the perineal region. It is therefore possible that total saddle pressure measurements may underestimate the actual insult incurred from cut-out saddles, since the higher pressures in the perineal region may be blunted when averaged over the entire saddle.
In a previous study, Schrader et al. evaluated male cyclist and noted that when perineum saddle pressures were reduced from a mean of 20kPA to 7kPA using noseless saddles, perineal saddle pressures, genital sensation and International Index of Erectile Function Questionnaire scores improved significantly (17). This suggest that the 4 and 11 unit kPa reductions seen in our riders may not have practical significance, especially since no differences were observed in the biothesiometry findings in the women evaluated. It is possible that identifying and modifying various riding parameters that can result in cumulative improvements in perineal pressures in women riders, may result in changes that are large enough to have a clinical impact. Using MRI, Bressel et al. noted that under pressure, peak cavernous space compression occurred below the most inferior aspect of the pubic symphysis (18), the region corresponding to the area from which perineal saddle pressures were recorded in our study. This suggests that the higher pressures that occur in the perineal region of women using cut-out saddles, could also result in increased compression of the perineum and more pronounced neurovascular compromise. Longitudinal studies are needed to determine if and to what extent chronic exposure to high saddle pressures and or incremental increases in pressure, impact the female pelvic floor over time.
Interestingly, no correlation was seen between genital sensation in the perineum and saddle pressures, regardless of what type of saddle was used. These findings should be interpreted with caution due to the cross-sectional design of this study and the small sample size. It is possible that the pressures obtained do not reflect the actual pressures of the cyclists when riding. In an effort to reduce this likelihood, saddle pressure determinations were made with riders’ pedaling on their own personal bicycles with the handlebars and saddles in the positions habitually used when they ride. Cyclists were also asked to assume the natural positions routinely used when riding, to try to mimic the typical riding environment of the participants. Still, only pressures obtained at a single time point were obtained and other factors that might influence saddle pressures, such as the type of terrain on which the women ride, the position of the saddle in relationship to the handlebars while riding and the pressure fluctuations in response to weight shifts during the crank cycle (19) were not considered. In addition, our genital sensation data points were obtained after the subjects rode 40-60 s, which is likely an insufficient time to assess transient, reversible pudendal nerve compromise. It is also possible that consistent with the male study, noseless saddles may show a more dramatic and meaningful improvement in genital sensation in women riders; however, conclusions about the benefits of these saddles cannot be drawn from our study since only nosed- traditional and cut-out saddles were used by our riders.
It is important to note that increasing saddle width also conferred a protective effect on peak perineum and mean total saddle pressures. These findings are consistent with findings in males. Schwarzer et al. studied penile oxygen pressures in 20 healthy males and concluded that saddle width, and not the amount of padding was the most important factor in protecting penile perfusion (10). They speculated that a larger saddle width provides sufficient support to the pelvic bones thus preventing compression of the perineal tissues. Additionally, in their study, no difference was seen in pressures for those riding nosed and noseless saddles of wider widths. More studies evaluating the effect of the saddle nose on women’s pelvic floor integrity are indicated.
Consistent with our previous study, we noted that age was significantly associated with decreased genital sensation. Surprisingly, we noted that increasing age was associated with improved perineal saddle pressures. While there is no clear explanation for these findings, we hypothesize that women with increased saddle pressures may stop riding due to neurological problems, such as pain, numbness or tingling and thus, our current sample may include a biased group of older, premenopausal women who, having no pressure-related problems continue to ride. Therefore, longitudinal studies trying to understand the role of aging and menopause on saddle pressures are needed.
Our study evaluated premenopausal, competitive women cyclists. It is therefore important to note that while our findings provide important insight for avid riders, the findings may not be generalizable to recreational riders. In a cohort of 81 consecutive bicycle riders, road cyclists had lower rates of erectile dysfunction compared to weekend cyclist and young, novice riders. (20) Likewise, our competitive female cyclists may be a biased group of women with reduced risk of genital issues. Additionally, studies including larger cohorts of women of various riding practices are critical, in order to understand the relationships between saddle design, saddle pressures and neurological function in all women cyclists.
Conclusion
To our knowledge, this represents the largest group of women cyclists studied to evaluate for variables that could predict elevations in saddle pressure and altered neurological function. Consistent with the findings of previous, smaller studies, our findings suggest that cut-out saddles confer a negative impact on saddle pressures. Although our study did not identify an association between tactile neurological function and saddle pressures or seat design, our prior study found that baseline neurological function is significantly decreased in competitive riders. Longitudinal studies that include baseline and interval evaluations of neurological assessment are necessary to confirm or refute the lack of association between neurological function, seat design and saddle pressures. Additionally, it is critical to consider parameters associated with typical riding sessions, in order to comprehensively investigate hazardous riding practices. Results from such studies can be used to provide constructive, corrective recommendations to ensure safer riding practices for women.
Acknowledgement
This work was supported in part by NIH grants 3P01DK60037–03S1 and #5K12HD047018, The Robert Wood Johnson Foundation Harold Amos Faculty Development Program and the Bronx Center to Reduce & Eliminate Ethnic & Racial Health Disparities (Bronx CREED). The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the National Institute of Health, the National Institute for Occupational Safety and Health or The Robert Wood Johnson Foundation. Mention of company or product names does not constitute endorsement by the National Institute for Occupational Safety and Health, The National Institute of Health or The Robert Wood Johnson Foundation.
Footnotes
Conflict of Interest: None
References
- 1.Morris JN, Clayton DG, Everitt MG, Semmence AM, Burgess EH. Exercise in leisure time: coronary attack and death rates. Br Heart J. 1990 Jun;63(6):325–34. doi: 10.1136/hrt.63.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfeld B, Jacobs DR, Jr, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med. 2009 Jul 13;169(13):1216–23. doi: 10.1001/archinternmed.2009.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Solomon S, Cappa KG. Impotence and bicycling. A seldom-reported connection. Postgrad Med. 1987 Jan;81(1):99–100. 102. doi: 10.1080/00325481.1987.11699662. [DOI] [PubMed] [Google Scholar]
- 4.Desai KM, Gingell JC. Hazards of long distance cycling. BMJ. 1989 Apr 22;298(6680):1072–3. doi: 10.1136/bmj.298.6680.1072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ricchiuti VS, Haas CA, Seftel AD, Chelimsky T, Goldstein I. Pudendal nerve injury associated with avid bicycling. J Urol. 1999 Dec;162(6):2099–100. doi: 10.1016/S0022-5347(05)68116-5. [DOI] [PubMed] [Google Scholar]
- 6.Andersen KV, Bovim G. Impotence and nerve entrapment in long distance amateur cyclists. Acta Neurol Scand. 1997 Apr;95(4):233–40. doi: 10.1111/j.1600-0404.1997.tb00104.x. [DOI] [PubMed] [Google Scholar]
- 7.Marceau L, Kleinman K, Goldstein I, McKinlay J. Does bicycling contribute to the risk of erectile dysfunction? Results from the Massachusetts Male Aging Study (MMAS) Int J Impot Res. 2001 Oct;13(5):298–302. doi: 10.1038/sj.ijir.3900733. [DOI] [PubMed] [Google Scholar]
- 8.Schrader SM, Breitenstein MJ, Clark JC, Lowe BD, Turner TW. Nocturnal penile tumescence and rigidity testing in bicycling patrol officers. J Androl. 2002 Nov-Dec;23(6):927–34. [PubMed] [Google Scholar]
- 9.Sommer F, König D, Graft C, Schwarzer U, Bertram C, Klotz T, Engelmann U. Impotence and genital numbness in cyclists. Int J Sports Med. 2001 Aug;22(6):410–3. doi: 10.1055/s-2001-16248. [DOI] [PubMed] [Google Scholar]
- 10.Schwarzer U, Sommer F, Klotz T, Cremer C, Engelmann U. Cycling and penile oxygen pressure: the type of saddle matters. Eur Urol. 2002 Feb;41(2):139–43. doi: 10.1016/s0302-2838(01)00028-8. [DOI] [PubMed] [Google Scholar]
- 11.Guess MK, Connell K, Schrader S, Reutman S, Wang A, LaCombe J, Toennis C, Lowe B, Melman A, Mikhail M. Genital sensation and sexual function in women bicyclists and runners: are your feet safer than your seat? J Sex Med. 2006 Nov;3(6):1018–27. doi: 10.1111/j.1743-6109.2006.00317.x. [DOI] [PubMed] [Google Scholar]
- 12.Vardi Y, Gruenwald I, Sprecher E, Gertman I, Yartnitsky D. Normative values for female genital sensation. Urology. 2000;56:1035–40. doi: 10.1016/s0090-4295(00)00850-5. [DOI] [PubMed] [Google Scholar]
- 13.Lowe BD, Schrader SM, Breitenstein MJ. Effect of bicycle saddle designs on the pressure to the perineum of the bicyclist. Med Sci Sports Exerc. 2004 Jun;36(6):1055–62. doi: 10.1249/01.mss.0000128248.40501.73. [DOI] [PubMed] [Google Scholar]
- 14.Carpes FP, Dagnese F, Kleinpaul JF, de Assis Martins E, Mota C Bolli. Bicycle Saddle Pressure: Effects of Trunk Position and Saddle Design on Healthy Subjects. Urol Int. 2009;82:8–11. doi: 10.1159/000176017. [DOI] [PubMed] [Google Scholar]
- 15.Carpes FP, Dagnese F, Kleinpaul JF, Ede A Martins, Mota CB. Effects of workload on seat pressure while cycling with two different saddles. J Sex Med. 2009 Oct;6(10):2728–35. doi: 10.1111/j.1743-6109.2009.01394.x. [DOI] [PubMed] [Google Scholar]
- 16.Frobose I, Baeyens L, Tofaute K. Ergonomics of 2 bicycle saddles—pressure at the pudendal area in women of a normal saddle with gel and of a saddle with a hole. The Bicycle Saddle Report 2003. 2003:A1–15. [Google Scholar]
- 17.Schrader SM, Breitenstein MJ, Lowe BD. Cutting off the nose to save the penis. J Sex Med. 2008 Aug;5(8):1932–40. doi: 10.1111/j.1743-6109.2008.00867.x. [DOI] [PubMed] [Google Scholar]
- 18.Bressel E, Reeve T, Parker D, Cronin J. Influence of bicycle seat pressure on compression of the perineum: a MRI analysis. J Biomech. 2007;40(1):198–202. doi: 10.1016/j.jbiomech.2005.11.017. [DOI] [PubMed] [Google Scholar]
- 19.Bressel E, Cronin J. Bicycle seat interface pressure: reliability, validity, and influence of hand position and workload. J Biomech. 2005 Jun;38(6):1325–31. doi: 10.1016/j.jbiomech.2004.06.006. [DOI] [PubMed] [Google Scholar]
- 20.Sommer F, Goldstein I, Korda JB. Bicycle riding and erectile dysfunction: A Review. J Sex Med. 2010 Jul;7(7):2346–58. doi: 10.1111/j.1743-6109.2009.01664.x. [DOI] [PubMed] [Google Scholar]