

Abstract
Background
We estimated medical costs attributable to venous thromboembolism (VTE) among patients currently or recently hospitalized for major surgery.
Methods
Using Rochester Epidemiology Project (REP) resources, we identified all Olmsted County, MN residents with objectively-diagnosed incident VTE within 92 days of hospitalization for major surgery over the 18-year period, 1988–2005 (n=355). One Olmsted County resident hospitalized for major surgery without VTE was matched to each case on event date (± 1 year), surgery type, duration of prior medical history and active cancer status. Subjects were followed in REP provider-linked billing data for standardized, inflation-adjusted direct medical costs from 1 year before index (case’s VTE event date and control’s matched date) to earliest of death, emigration, or 12/31/2011. We used generalized linear modeling to predict costs for cases and controls, and employed bootstrapping methods to assess uncertainty and significance of mean adjusted cost differences.
Results
Adjusted mean predicted costs were more than 1.5-fold higher for cases ($55,956) than for controls ($32,718) (P=<0.001) from index to up to 5 years post-index. Cost differences between cases and controls were greatest within the first 3 months after index (mean difference=$12,381). Costs were significantly higher for cases than controls (mean difference=$10,797) from 3 months to up to 5 years post-index and together accounted for about half of the overall cost difference.
Conclusions
VTE during or after recent hospitalization for major surgery contributes a substantial economic burden; VTE-attributable costs are highest in the initial 3 months but persist for up to 5 years.
Keywords: cost analysis, medical care utilization, deep vein thrombosis, pulmonary embolism, venous thromboembolism, cost of Illness
INTRODUCTION
Venous thromboembolism, consisting of deep vein thrombosis (DVT) and its complication, pulmonary embolism (PE), causes substantial morbidity and mortality among persons currently or recently hospitalized for major surgery.1 Moreover, the long-term complications and costs associated with an incident VTE may also represent a significant economic burden. Cost-of-illness estimates related to VTE among those currently or recently hospitalized for major surgical procedures are essential for informing allocation of scarce resources, targeting efforts toward prevention, identifying best practices, addressing future care needs, and implementing cost-effective treatments.2 However, the few existing estimates of VTE-associated costs have largely focused on orthopedic surgery.3 Previous studies typically failed to include subjects currently or recently hospitalized for other major surgical procedures such as general, gynecological, cardiothoracic, and neurosurgery.
To address these limitations, we performed a population-based matched-cohort study to estimate excess medical costs attributable to VTE that occurred during or recently after hospitalization for surgery, independent of potential confounding due to VTE risk factors. We took advantage of Rochester Epidemiology Project (REP) resources, including a previously identified population-based inception cohort consisting of all Olmsted County, MN residents with objectively-diagnosed incident VTE as well as previously identified matched non-VTE controls drawn from the same population.4 REP resources also afforded provider-linked objective estimates of direct medical costs based on line item detail for every service and procedure over extended periods of time.5 Combining objectively-diagnosed VTE cases and controls with objective cost data for each individual afforded the opportunity to estimate medical care costs attributable to VTE among those currently or recently hospitalized for major surgery, 1) across the full spectrum from symptomatic through fatal events, 2) from before the event until death or emigration from the area, 3) adjusting for age, sex and calendar year, and 4) adjusting for prevalent co-morbid conditions. Thus, we were able to estimate the excess cost of medical care that is attributable to VTE independent of potential confounding due to VTE risk factors.6
METHODS
Study Setting and Design
Olmsted County, MN (2010 census population=144,248), provides a unique opportunity for investigating the natural history of VTE.7–9 Rochester, the county seat, is approximately 80 miles from the nearest major metropolitan area. Mayo Clinic, together with Olmsted Medical Center (OMC), a second group practice and their affiliated hospitals, provide over 95% of all medical care delivered to local residents.10 Since 1907, every Mayo patient has been assigned a unique identifier; all information from every provider contact is contained within a unit record for each patient. Diagnoses assigned at each visit are coded and entered into continuously updated files. Under auspices of the REP, the unique identifiers, diagnostic index, and medical records linkage were expanded to include the other providers of medical care to local residents, including OMC and the few private practitioners in the area in 1965, thereby linking the medical records for community residents at the individual level.4,11 Using REP resources, we performed a cohort study. The study was approved by the Mayo Clinic and OMC Institutional Review Boards.
Study Population
All Olmsted County, MN residents with incident DVT or PE over the 40-year period, 1966–2005, were identified as previously described.7 REP records of individuals who refused authorization for use of medical records in research (typically <5%) were excluded from review.10,12 The medical records for remaining individuals were reviewed from date first seen until date last seen at any REP provider to identify, confirm, and characterize each VTE event. Incident events were limited to persons residing in Olmsted County for whom this was a first lifetime symptomatic VTE. Record review was performed by trained, experienced nurse abstractors. The review included all outpatient, emergency department and hospitalization records (including nursing notes), radiological, ultrasound and nuclear medicine imaging reports, surgical records, vascular laboratory reports, echocardiography reports, autopsy reports and death certificates.
Study nurses recorded method of VTE diagnosis, VTE event type (DVT, PE, or both; chronic thromboembolic pulmonary hypertension), date of VTE (i.e., “index date” for cases), location at onset of VTE symptoms and/or signs (hospital, nursing home, and community), and patient age and sex, and presence of active cancer and cancer type as of the VTE event date. The present study was limited to “objectively-diagnosed” events, as previously described, 1,7,9,13 and included all incident VTE cases with recent hospitalization for major surgery (i.e., hospitalization discharge within 92 days [365 days/4 or ~3 months] before VTE event date); residents admitted to hospital for VTE treatment were not included. The surgical hospitalization closest to but before VTE or the surgical hospitalization during which VTE occurred was selected as the “baseline hospitalization”. Cases with a hospitalization for acute medical illness within 92 days before baseline were included if they also had a surgery hospitalization within 92 days.
REP also provides enumeration of the entire Olmsted County population from which potential controls can be sampled.4 Using this system, we identified all Olmsted County residents with hospitalization for major surgery within ±1 year of each case’s VTE event date, length of medical record similar to the matched VTE case, and no prior VTE.8 For patients with multiple surgical hospitalizations per year, one hospitalization was randomly chosen to comprise the sampling frame. From this, a random sample of potential controls was identified of which two were matched on case VTE event date ± 1 year, International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) Procedure (surgery) Code and active cancer status. One control was randomly chosen for the current study. The hospitalization identified in the sampling frame was selected as the control’s “index hospitalization”. Assignment of the control’s index date depended on whether the matched case’s VTE event occurred during or after the case’s index hospitalization (Figure 1). For cases whose VTE occurred during the index hospitalization, the control’s index date was randomly assigned to be between a day after the control’s surgery and discharge dates to ensure that direct surgical costs were not included in post-index costs. For cases whose VTE occurred within 92 days after discharge from the index hospitalization, the control’s index date was randomly assigned to be a day within 92 days after the control’s index hospitalization discharge date. Medical records of potential controls were reviewed to confirm Olmsted County residency and that they matched the case with respect to active cancer status and specific ICD-9-CM procedure (surgery) codes as of index.
Figure 1.

Flow diagram on the identification and selection of a matched non-VTE control for each VTE case.
Collection of Medical Costs
Through an electronic data-sharing agreement between Mayo Clinic and OMC, patient-level administrative data on healthcare utilization and associated billed charges incurred at these institutions are shared and archived within the Olmsted County Healthcare Expenditure and Utilization Database (OCHEUD) for use in approved research studies. Data are electronically linked, affording complete information on all hospital and ambulatory care delivered by these providers to area residents from 1/1/1987 through 12/31/2011. OCHEUD includes information on all Olmsted County residents (i.e., both sexes, all ages, and all payer types, including the uninsured) and contains line-item detail on date, type, frequency, and billed charge for every good or service provided. Because of well-known discrepancies between billed charges and true resource use, utilization in OCHEUD is valued using standard methods by grouping services into the Medicare Part A and B classifications; Part A billed charges (hospital-billed services and procedures) are adjusted using hospital cost-to-charge ratios at the departmental level and wage indexes. Medicare Part B items (primarily physician-billed services) are valued using national average Medicare reimbursement rates. Costs are adjusted for inflation to express costs in constant dollars; cost estimates in this study were adjusted to 2011 dollars. The combination of OCHEUD and REP resources makes population-based health economic research feasible for numerous medical conditions.5,14–16 Because cost data are only available electronically since 1987 and we wished to obtain costs in the year before index, the present study was limited to all Olmsted County residents with a first lifetime objectively-diagnosed DVT or PE, 1988–2005.1,7 Each case and control was followed forward in time for costs from 1 year before their respective index date to the earliest of death, emigration from Olmsted County, or 12/31/2011 (study end date). We ensured similar periods of observation for each case and matched control by censoring both members of each pair as of the shortest length of follow-up for either member.
Pre-index Comorbid Conditions
To compare baseline characteristics and comorbidities between cases and controls, we obtained all ICD-9-CM diagnoses codes assigned to each individual in OCHEUD 1 year before index and categorized every diagnosis code assigned each individual into the 17 ICD-9-CM chapters and approximately 114 subchapters. A summary measure of medical conditions in the year before index was obtained using Johns Hopkins Adjusted Clinical Groups (ACG) System® software.17 ACG software categorizes individual’s diagnosis codes into groupings based on persistence, severity, and etiology of the condition, as well as diagnostic certainty, and need for specialty care.17 ACG software was also used to assign a Resource Utilization Band (RUB) value to each individual. RUB categories are aggregations of ACGs that have similar expected resource use, with values ranging from 0 (no relevant diagnosis codes) to 5 (diagnosis codes associated with very high use).18
Statistical Analyses
Analyses were conducted in SAS version 9.02 (SAS Institute, Cary, NC). Statistical testing used the two-tailed alpha level of 0.05. The principal outcome was direct medical costs associated with VTE. We analyzed costs from 1 year before index to index to a maximum of 5 years post-index. Post-index analyses were also subdivided into index-3 months, 3–6 months, 6-months-1 year, 1–2 years, 2–3 years, 3–4 years, and 4–5 years. Models from post-index to 5 years and 3 months to 5 years included length of follow up from index. For each subdivided post-index period, analyses were limited to those who were eligible for costs in each interval period. In initial analyses, the unadjusted costs for each control were subtracted from costs for his/her case in each time period; statistical significance was assessed using Wilcoxon signed-rank test to account for the highly skewed nature of cost data and paired observations.5,15,16,19,20 To isolate the costs attributable to VTE, we used general linear multivariate modeling to examine the extent to which age, sex, RUB measure of pre-index comorbidity, and pre-index costs accounted for post-index cost differences between cases and controls. This adjusted approach employed two-part models to account for zero costs21,22 when appropriate, and incorporated a generalized linear model with family distribution based on the modified Park test recommended by Manning and Mullahy.23 This analytic approach accounts for the skewed cost distribution while enabling coefficients to be directly back-transformed into the original dollar scale.24,25 We analyzed differences in costs between cases and controls using the method of recycled predictions, setting all individuals as cases with VTE or as controls without VTE, while all other individual characteristics remain as observed.26,27 Mean values and bootstrapped 95% confidence intervals of the mean difference were calculated.
RESULTS
Demographic and baseline clinical characteristics
We identified 355 VTE cases and matched controls who were hospitalized for major surgery within 92 days before index (i.e., VTE event for cases and approximate matched date for control). The mean ± SD (median; range) patient age for cases and controls was 62 ±16 (63; 1–96) and 60 ±18 (63; 16–101) years, respectively (p=0.12), and 55% of cases and 52% of controls were female (p=0.5). The mean body mass index (BMI) for VTE cases and matched controls was 28.3 and 27.8 kg/m2, respectively, and did not differ significantly (p=0.23). The length of follow-up post-index ranged from 1 day to 23 years. Of all VTE events, 152 (43%) occurred during the baseline hospitalization and 203 (57%) occurred within 92 days after discharge. The VTE event type distribution was DVT alone (n=214; 60%), PE alone (n=105; 30%), PE with DVT (n=36; 10%) and chronic thromboembolic pulmonary hypertension (n=0; 0%). In the year before index, significant differences between cases and controls were observed in 6 of 17 ICD-9-CM chapters (Supplementary Table). Within the chapters, there were several significant differences at the subchapter level. Figure 2 provides the RUB summary measure of pre-index comorbidity for cases and controls. In the year before index, 50% (n=176) of cases had a RUB value indicative of very high use compared to 38% (n=133) of controls.
Figure 2.
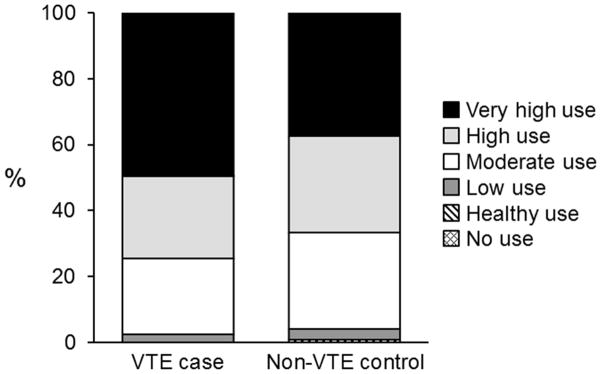
Distribution of RUB values in the 1-year before index for VTE cases and non-VTE controls.
Observed cost comparisons
Table 1 provides unadjusted mean, median (interquartile range [IQR]), minimum and maximum direct medical costs for case/control pairs and mean cost differences between case/control pairs from 1 year before index, index to 5 years post-index and selected periods within index to 5-years post-index. During the period, index to 5 years post-index, nine matched pairs had at least 1 member who did not accrue any costs and both members of the pair were excluded. In the year before index, both mean and median costs for cases were slightly higher compared to controls, in part reflecting the highly skewed distribution for cases compared to that for controls. The unadjusted mean difference in pre-index annual costs between cases and controls was $6,867 (95% CI: $2,791–$11,483). Overall 5 years post-index and within each post-index period up to 2 years, the mean unadjusted costs were significantly higher for cases. Unadjusted costs were non-significantly higher in post-index periods 2–3, 3–4, and 4–5 years.
TABLE 1.
Unadjusted Direct Medical Costs for Venous Thromboembolism Case/Control Pairs by Time Period
| Time Period | Case/Control Pairs (n) | Case ($) | Control ($) | Mean Difference ($) | Wilcoxon Signed Rank P-Value |
|---|---|---|---|---|---|
| Year before index | 355 | ||||
| mean | 35,410 | 28,543 | 6,867 | p= 0.001 | |
| median | 22,879 | 19,522 | 2,646 | ||
| P25* | 14,043 | 12,401 | −7,558 | ||
| P75* | 42,473 | 34,189 | 16,568 | ||
| Min | 399 | 657 | −197,842 | ||
| Max | 260,056 | 259,780 | 243,635 | ||
| Index to 5 years | 355 | ||||
| mean | 57,887 | 28,397 | 29,490 | p<0.001 | |
| median | 31,991 | 14,889 | 12,109 | ||
| P25 | 15,596 | 5,837 | −3,086 | ||
| P75 | 61,324 | 35,124 | 41,269 | ||
| min | 0 | 0 | −194,958 | ||
| max | 1,060,138 | 214,112 | 1,045,370 | ||
| Index to 3 months | 355 | ||||
| mean | 23,154 | 7,259 | 15,895 | p<0.001 | |
| median | 9,519 | 1,961 | 6,989 | ||
| P25 | 5,325 | 354 | 2,051 | ||
| P75 | 23,833 | 7,332 | 18,236 | ||
| min | 0 | 0 | −93,610 | ||
| max | 442,015 | 122,358 | 429,062 | ||
| 3 to 6 months | 306 | ||||
| mean | 4,799 | 2,433 | 2,366 | p<0.001 | |
| median | 750 | 295 | 301 | ||
| P25 | 213 | 33 | −233 | ||
| P75 | 2,666 | 1,553 | 1,848 | ||
| min | 0 | 0 | −57,622 | ||
| max | 102,411 | 61,212 | 102,411 | ||
| 6 months to 1 year | 285 | ||||
| mean | 6,613 | 3,566 | 3,047 | p<0.001 | |
| median | 1,230 | 765 | 195 | ||
| P25 | 336 | 154 | −1,010 | ||
| P75 | 5,437 | 2,703 | 2,878 | ||
| min | 0 | 0 | −85,583 | ||
| max | 232,455 | 85,897 | 230,580 | ||
| 1 year to 2 years | 266 | ||||
| mean | 10,952 | 5,984 | 4,967 | p=0.034 | |
| median | 2,363 | 2,073 | 126 | ||
| P25 | 793 | 675 | −2,208 | ||
| P75 | 8,148 | 5,823 | 5,783 | ||
| min | 0 | 0 | −113,374 | ||
| max | 339,919 | 113,861 | 337,983 | ||
| 2 to 3 years | 252 | ||||
| mean | 9,633 | 6,570 | 3,063 | p=0.134 | |
| median | 2,779 | 1,764 | 302 | ||
| P25 | 740 | 601 | −2,479 | ||
| P75 | 8,402 | 5,982 | 4,680 | ||
| min | 0 | 0 | −88,668 | ||
| max | 174,796 | 92,861 | 173,974 | ||
| 3 to 4 years | 237 | ||||
| mean | 8,885 | 5,733 | 3,151 | p=0.086 | |
| median | 2,069 | 1,670 | 326 | ||
| P25 | 673 | 438 | −2,375 | ||
| P75 | 6,299 | 6,018 | 3,929 | ||
| min | 0 | 0 | −65,110 | ||
| max | 196,820 | 65,110 | 167,847 | ||
| 4 to 5 years | 219 | ||||
| mean | 6,990 | 5,192 | 1,798 | p=0.312 | |
| median | 1,691 | 1,485 | 109 | ||
| P25 | 488 | 540 | −1,971 | ||
| P75 | 6,394 | 5,092 | 3,193 | ||
| min | 0 | 0 | −59,635 | ||
| max | 87,086 | 59,635 | 87,086 |
25th and 75th interquartile range
Adjusted cost comparisons
Table 2 provides adjusted mean direct medical costs for cases and controls, and the adjusted cost difference, for the overall time period, index to 5 years post-index, and for intervals within that period. After adjusting for group differences in age at index, sex, costs incurred 1 year before index and RUB values, the mean predicted costs for cases ($55,956) were significantly higher than those for controls ($32,718), with a mean predicted cost difference of $23,238 (Bootstrapped 95% CI: $15,521–30,934), as compared to the unadjusted difference of $29,490. The adjusted mean cost was significantly higher for VTE cases than controls for index to 3 months post-index. Although adjusted predicted costs were not significantly different from controls for any of the periods from 3 months to 5 years post-index, all these periods showed strong trends to higher costs for cases, and together they accounted for about half of the overall cost difference. Moreover, when the time period, 3 month to 5 years post-index, was combined, the adjusted mean predicted cost for cases ($36,749) were significantly higher than those for controls ($25,952), with a mean predicted difference of $10,797 (Bootstrapped 95%CI: $4,152–18,034). Among DVT alone cases, the adjusted mean cost for index to 3 months was $25,146 compared to $8,918 for controls (mean difference=$16,228). Among PE alone cases, the adjusted mean cost for index to 3 months was $19,630 compared to $5,710 for controls (mean difference=$13,920).
TABLE 2.
Adjusted* Mean Direct Medical Costs for Venous Thromboembolism Case/Control Pairs by Time Period
| Time Period | Cases ($) | Controls ($) | Mean Difference (95% CI; $) |
|---|---|---|---|
| Index to 5 years | 55,956 | 32,718 | 23,238 (15,521, 30,934) |
| Index to 3 months | 21,236 | 8,855 | 12,381 (9,516, 16,653) |
| 3 to 6 months | 4,135 | 3,564 | 571 (−1,159, 1,987) |
| 6 months to 1 year | 5,951 | 4,833 | 1,118 (−735, 3,017) |
| 1 to 2 years | 9,835 | 7,613 | 2,222 (−891, 5,533) |
| 2 to 3 years | 9,609 | 7,771 | 1,838 (−1,104, 5,216) |
| 3 to 4 years | 8,617 | 6,741 | 1,876 (−875, 4,777) |
| 4 to 5 years | 6,925 | 6,422 | 503 (−1,668, 2,610) |
| 3 months to 5 years | 36,749 | 25,952 | 10,797 (4,152, 18,034) |
Predicted cost adjusted for age, sex, costs in the year prior to index and Resource Utilization Band
COMMENT
This population-based study was conducted to quantify the extent to which VTE contributes to excess medical costs among those currently or recently hospitalized for major surgery and the duration of time any excess costs persist. The present study followed individuals who were hospitalized for major surgery to compare total direct medical costs between patients who did and did not experience an objectively-confirmed VTE during or within 92 days after hospitalization for major surgery, the time period of highest VTE risk. The adjusted predicted mean direct medical costs were significantly higher for cases than for controls from index to 5-years post-index. The adjusted predicted mean cost for VTE cases was 1.5-fold higher ($55,956) compared to controls ($32,718; mean difference=$23,238). VTE-attributable costs were highest within 3-months following VTE; the adjusted predicted mean difference in direct medical costs between persons who did and did not experience VTE was $12,381.
In comparison, the costs of VTE related to hospitalization for acute medical illness exceed costs of VTE related to hospitalization for surgery.28 The adjusted mean predicted costs in those hospitalized for acute medical illness were 2.5-fold higher for cases ($62,838) than for controls ($24,464) (P=<0.001) from index to up to 5 years post-index. Similar to VTE related to surgery, cost differences between cases and controls were greatest within the first 3 months after index for those hospitilized for acute medical illness (mean difference=$16,897).
While adjusting for age, sex, costs in the year prior to index and RUB reduced the predicted mean difference in costs for all time period (Tables 1 and 2), the adjusted mean cost difference remained significantly increased. The observed increased costs for cases compared to controls from 3 months to 5 years post-index could reflect incremental costs for management of VTE complications (i.e., post thrombotic syndrome, chronic thromboembolic pulmonary hypertension) and VTE recurrence. Over the full 5-year post-index time period, 61 (17%) VTE cases had recurrent VTE with a median time to recurrence of 49 days (IQR: 4 days–4.7 years). From index to 5 years post-index, the adjusted predicted mean cost for the 61 VTE cases with recurrent VTE was $93,446 versus $33,145 for their matched non-VTE controls (mean difference=$60,301; 95% CI: $33,889; $100,600). The adjusted predicted mean cost of the 294 VTE cases without recurrent VTE was $48,503 compared to $31,863 for their matched controls (mean difference=$16,640; 95% CI: $8,991; $23,947). While the number of cases with both DVT and PE (n=36) was too small for meaningful analysis, the similar mean cost difference for DVT alone and PE alone cases ($16,228 and $13,920, respectively) suggests that VTE event type (DVT vs. PE) is an unlikely explanation for the significant difference in mean costs for VTE cases compared to matched controls. Moreover, since mean BMI was not significantly different between cases, BMI is also an unlikely explanation for the significant difference in mean costs. Furthermore, RUB scores indirectly adjust for BMI to the extent that the consequences of BMI contribute to higher healthcare utilization and the associated costs of care.
There are very few studies of VTE-attributable costs among patients with VTE related to hospitalization for surgery. In a study of claims data from adult patients undergoing total hip or knee replacement surgery, the all-cause inpatient costs among patients with a primary or secondary diagnosis code for VTE (cases; n=8042) and controls matched on age, sex, risk factors for VTE, risk factors for bleeding, anticoagulant prophylaxis and propensity score were $21,014 and $18,350 for cases and controls, respectively (difference=$2,663).3 Due to marked differences in study populations, data sources, methods and length of follow-up, the absolute difference in costs between VTE cases and controls in this study cannot be compared to those in our study, but the costs are consistently higher for VTE cases in both studies.
Our study has important limitations. The cost estimates are for a single geographic population which in 2010 was 90% white. The age-, sex- and racial-distribution of Olmsted County is similar to that for Minnesota, the upper mid-west, and the U.S. white population; however, residents of Olmsted County exhibit higher median income and education level compared to these geographic regions.4,10 While no single geographic area is representative of all others, the under-representation of minorities may compromise the generalizability of our findings to different racial and ethnic groups. Indeed, our VTE-attributable cost estimates may be conservative compared with results in a different more diverse population (such as a hospital serving an underserved low healthcare access population). Costs associated with pharmacologic treatments were not included in this analysis due to lack of electronically available data on outpatient pharmacological costs throughout the total time period. However, the incremental costs of VTE pharmacologic treatment likely would increase the cost difference between cases and controls. Cost estimates were limited to direct medical care costs and did not include indirect or nursing home costs. Finally, despite adjusting for age, sex, costs in the 1 year prior to index and RUB, we may not have accounted for all baseline differences (observed or unobserved) between cases and controls.
In conclusion, VTE contributes a substantial economic burden to patients hospitalized for major surgery. Our findings will inform models that assess the cost-effectiveness of alternative interventions to reduce VTE occurrence and guide reimbursement policy.
Supplementary Material
SUPPLEMENTARY TABLE. Baseline Patient Characteristics and Comorbidities by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9CM) Code*
Acknowledgments
Research reported in this publication was supported in part by grants from the National Heart Lung and Blood Institute under Award Numbers R01HL66216 and K12HL83141 (a training grant in Vascular Medicine [KPC]) to JAH, National Institute of General Medical Sciences under Award Number K08GM093133-05 to MSP, and was made possible by the Rochester Epidemiology Project (Award Number R01AG034676 of the National Institute on Aging, National Institutes of Health). Research support also was provided by Mayo Foundation.
We gratefully acknowledge Catherine L. Brandel, R.N., Diadra H. Else, R.N., Jane A. Emerson, R.N., and Cynthia L. Nosek, R.N. for excellent data collection and Cynthia E. Regnier, R.N., as research project manager. Research reported in this publication was supported in part by grants from the National Heart Lung and Blood Institute under Award Numbers R01HL66216 and K12HL83141 (a training grant in Vascular Medicine [KPC]) to JAH, and was made possible by the Rochester Epidemiology Project (Award Number R01AG034676 of the National Institute on Aging, National Institutes of Health). Research support also was provided by Mayo Foundation.
Footnotes
All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analyses.
All authors report no conflict of interest.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Heit JA. The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28:370–372. doi: 10.1161/ATVBAHA.108.162545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13:475–486. doi: 10.18553/jmcp.2007.13.6.475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vekeman F, LaMori JC, Laliberte F, Nutescu E, Duh MS, Bookhart BK, et al. In-hospital risk of venous thromboembolism and bleeding and associated costs for patients undergoing total hip or knee arthroplasty. J Med Econ. 2012;15:644–653. doi: 10.3111/13696998.2012.669438. [DOI] [PubMed] [Google Scholar]
- 4.Melton LJ., 3rd History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71:266–274. doi: 10.4065/71.3.266. [DOI] [PubMed] [Google Scholar]
- 5.Leibson CL, Katusic SK, Barbaresi WJ, Ransom J, O’Brien PC. Use and costs of medical care for children and adolescents with and without attention-deficit/hyperactivity disorder. JAMA. 2001;285:60–66. doi: 10.1001/jama.285.1.60. [DOI] [PubMed] [Google Scholar]
- 6.Larg A, Moss JR. Cost-of-illness studies: a guide to critical evaluation. PharmacoEconomics. 2011;29:653–671. doi: 10.2165/11588380-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 7.Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162:1245–1248. doi: 10.1001/archinte.162.11.1245. [DOI] [PubMed] [Google Scholar]
- 8.Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ., 3rd Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. 2000;160:809–815. doi: 10.1001/archinte.160.6.809. [DOI] [PubMed] [Google Scholar]
- 9.Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ., 3rd Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158:585–593. doi: 10.1001/archinte.158.6.585. [DOI] [PubMed] [Google Scholar]
- 10.St Sauver JL, Grossardt BR, Yawn BP, Melton LJ, 3rd, Rocca WA. Use of a medical records linkage system to enumerate a dynamic population over time: the Rochester epidemiology project. Am J Epidemiol. 2011;173:1059–1068. doi: 10.1093/aje/kwq482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.St Sauver JL, Grossardt BR, Leibson CL, Yawn BP, Melton LJ, 3rd, Rocca WA. Generalizability of epidemiological findings and public health decisions: an illustration from the Rochester Epidemiology Project. Mayo Clin Proc. 2012;87:151–160. doi: 10.1016/j.mayocp.2011.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Melton LJ., 3rd The threat to medical-records research. N Engl J Med. 1997;337:1466–1470. doi: 10.1056/NEJM199711133372012. [DOI] [PubMed] [Google Scholar]
- 13.Leibson CL, Needleman J, Buerhaus P, Heit JA, Melton LJ, 3rd, Naessens JM, et al. Identifying in-hospital venous thromboembolism (VTE): a comparison of claims-based approaches with the Rochester Epidemiology Project VTE cohort. Med Care. 2008;46:127–132. doi: 10.1097/MLR.0b013e3181589b92. [DOI] [PubMed] [Google Scholar]
- 14.Gabriel SE, Tosteson AN, Leibson CL, Crowson CS, Pond GR, Hammond CS, et al. Direct medical costs attributable to osteoporotic fractures. Osteoporos Int. 2002;13:323–330. doi: 10.1007/s001980200033. [DOI] [PubMed] [Google Scholar]
- 15.Long KH, Rubio-Tapia A, Wagie AE, Melton LJ, 3rd, Lahr BD, Van Dyke CT, et al. The economics of coeliac disease: a population-based study. Aliment Pharmacol Ther. 2010;32:261–269. doi: 10.1111/j.1365-2036.2010.04327.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leibson CL, Brown AW, Hall Long K, Ransom JE, Mandrekar J, Osler TM, et al. Medical care costs associated with traumatic brain injury over the full spectrum of disease: a controlled population-based study. Journal of neurotrauma. 2012;29:2038–2049. doi: 10.1089/neu.2010.1713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Johns Hopkins Bloomberg School of Public Health. 2010 [computer program] [Google Scholar]
- 18.Johns Hopkins Bloomberg School of Public Health. 2002. [computer program] [Google Scholar]
- 19.Leibson CL, Hu T, Brown RD, Hass SL, O’Fallon WM, Whisnant JP. Utilization of acute care services in the year before and after first stroke: A population-based study. Neurology. 1996;46:861–869. [PubMed] [Google Scholar]
- 20.Leibson CL, Long KH, Maraganore DM, Bower JH, Ransom JE, O’Brien PC, et al. Direct medical costs associated with Parkinson’s disease: a population-based study. Mov Dosord. 2006;21:1864–1871. doi: 10.1002/mds.21075. [DOI] [PubMed] [Google Scholar]
- 21.Buntin MB, Zaslavsky AM. Too much ado about two-part models and transformation? Comparing methods of modeling Medicare expenditures. J Health Econ. 2004;23:525–542. doi: 10.1016/j.jhealeco.2003.10.005. [DOI] [PubMed] [Google Scholar]
- 22.Newhouse JP, Manning WG, Morris CN, Orr LL, Duan N, Keeler EB, et al. Some interim results from a controlled trial of cost sharing in health insurance. N Engl J Med. 1981;305:1501–1507. doi: 10.1056/NEJM198112173052504. [DOI] [PubMed] [Google Scholar]
- 23.Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ. 2001;20:461–494. doi: 10.1016/s0167-6296(01)00086-8. [DOI] [PubMed] [Google Scholar]
- 24.Birnbaum HG, Ben-Hamadi R, Greenberg PE, Hsieh M, Tang J, Reygrobellet C. Determinants of direct cost differences among US employees with major depressive disorders using antidepressants. Pharmaco Economics. 2009;27:507–517. doi: 10.2165/00019053-200927060-00006. [DOI] [PubMed] [Google Scholar]
- 25.Mullahy J. Much ado about two: reconsidering retransformation and the two-part model in health econometrics. J Health Econ. 1998;17:247–281. doi: 10.1016/s0167-6296(98)00030-7. [DOI] [PubMed] [Google Scholar]
- 26.Basu A, Arondekar BV, Rathouz PJ. Scale of interest versus scale of estimation: comparing alternative estimators for the incremental costs of a comorbidity. Health Econ. 2006;15:1091–1107. doi: 10.1002/hec.1099. [DOI] [PubMed] [Google Scholar]
- 27.Esposito D, Bagchi AD, Verdier JM, Bencio DS, Kim MS. Medicaid beneficiaries with congestive heart failure: association of medication adherence with healthcare use and costs. Am J Manag Care. 2009;15:437–445. [PubMed] [Google Scholar]
- 28.Cohoon KP, Ransom JE, Ashrani AA, Petterson TM, Hall Long K, Bailey KR, et al. Costs of Venous Thromboembolism Associated with Hospitalization for Medical Illness. Am J Manag Care. 2014 in submission. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
SUPPLEMENTARY TABLE. Baseline Patient Characteristics and Comorbidities by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9CM) Code*