

Abstract
Background:
Delay to neurosurgical care can result in significant morbidity and mortality. In this study, we aim to identify and quantify the sources of delay to neurosurgical consultation and care at a rural setting in Kenya.
Methods:
A mixed-methods, cross-sectional analysis of all patients admitted to the neurosurgical department at Kijabe Hospital (KH) was conducted: A retrospective analysis of admissions from October 1 to December 31, 2013 and a prospective analysis from June 2 to June 20, 2014. Sources of delay were categorized and quantified. The Kruskal–Wallis test was used to identify an overall significant difference among diagnoses. The Mann–Whitney U test was used for pairwise comparisons within groups; the Bonferroni correction was applied to the alpha level of significance (0.05) according to the number of comparisons conducted. IBM SPSS version 22.0 (SPSS, Chicago, IL) was used for statistical analyses.
Results:
A total of 332 admissions were reviewed (237 retrospective, 95 prospective). The majority was pediatric admissions (median age: 3 months). Hydrocephalus (35%) and neural tube defects (NTDs; 27%) were most common. At least one source of delay was identified in 192 cases (58%); 39 (12%) were affected by multiple sources. Delay in primary care (PCPs), in isolation or combined with other sources, comprised 137 of total (71%); misdiagnosis or incorrect management comprised 46 (34%) of these. Finances contributed to delays in 25 of 95 prospective cases. At a median delay of 49 and 200.5 days, the diagnoses of hydrocephalus and tumors were associated with a significantly longer delay compared with NTDs (P < 0.001).
Conclusion:
A substantial proportion of patients experienced delays in procuring pediatric neurosurgical care. Improvement in PCP knowledge base, implementation of a triage and referral process, and development of community-based funding strategies can potentially reduce these delays.
Keywords: Delay, developing nations, neurosurgery, outcome, rural
INTRODUCTION
Although the provision of medical care in Sub-Saharan Africa has improved significantly in the past few decades, there remain significant deficiencies with regard to accessibility of care, resulting in potentially serious and irreversible consequences for patients.[10,18,28] In addition to the individual patient, the consequences of delay in care pose a significant pressure on patients’ families and dependents, along with a large burden of cost to the public healthcare system.[10] Through the analysis of sources of delay in accessing medical care in low-income nations, the following themes have emerged as the fundamental causes: Cultural beliefs and practices, financial restrictions, knowledge and skills of primary care providers and the public's perception of same, and transportation.[8,9,11,22,29,31]
While consequences of delay pertain to virtually all medical specialties, the field of neurosurgery is particularly time-sensitive and minutes to hours may mean the difference between life and death and/or disability. Access to timely neurosurgical care is problematic in many low and middle-income nations but few studies have been devoted to its characterization and quantification.[10]
The dearth of access to neurosurgical care in Sub-Saharan nations such as Kenya is a serious issue. In Kenya, there is one neurosurgeon for every 3.2 million residents; for comparison, there is 1 per 60,000 in the United States.[26] In the current study, we have sought to identify and quantify the sources of delay to neurosurgical care at Kijabe Hospital (KH) in Kijabe, Kenya. This choice of setting was based on the expanding role of Kenya's neurosurgical presence in East and Central Africa with regard to both number of staff neurosurgeons and the presence of the only neurosurgical residency programs in the region.[24] Particularly, we have aimed to focus on KH, a center offering primarily pediatric neurosurgical care for Kijabe and surrounding regions. Our goal was to identify influential factors that, if improved, could improve the delivery of neurosurgical care for the regional population served by KH. A study by Idowu and Apemiye, assessing an adult population of brain tumors presenting to a neurosurgical unit in Lagos, Nigeria, had shown that the greatest period of delay was in the prepresentation (following symptoms but prior to seeking medical attention) phase followed by the prediagnostic interval.[19] Therefore, our hypothesis was that a similar trend would be found in our sample population as well.
METHODS
Design
In this cross-sectional study, a combination of a retrospective and prospective chart review analysis of patient admissions was undertaken. For the retrospective component, an arbitrary time frame of October–December, 2013 was selected. This was based on prior knowledge regarding the average volume of admissions to the neurosurgical department at KH. For the prospective component, admissions during an arbitrary time frame of June 2–20, 2014 were recorded and analyzed. Prior admissions for the same patient (applicable to the retrospective part of the study) were also collected and analyzed. These repeat admissions were not used in the calculation of distances travelled by patients.
Demographic information, details with regard to presenting pathology, and management timing and strategy were recorded. Categories of pathologies managed were as follows: Hydrocephalus – or procedures related to its management – (HCP); isolated neural tube defects (NTD); combined HCP + NTD; tumor; trauma; infections; and other miscellaneous categories (e.g. scalp lesions).
With regard to the identification and quantification of sources of delay, the following time periods were recorded (median values):
Time Frame #1: Time period between recognition of symptoms to seeking medical attention (days) [prehospital delay]
Time Frame #2: Time period between seeking medical attention to neurosurgical consultation (days) [delay at primary care]
Time Frame #3: Time to procurement of neurosurgical care upon admission (or diagnosis in cases where conservative/medical management was selected) (days) [neurosurgical in-service delay]
Time Frame #4: Length of stay (days).
In cases where the chart data were not clear with regard to time frame #1 (prehospital delay), this field was left blank. Accurate documentation of these time frames was limited by the values entered on the initial consultation upon admission to KH.
In the prospective component of the investigation, a more comprehensive assessment of the patient's social and medical history was attained. As a result, additional information such as method (s) of travel and data regarding time of travel from the patient's initial starting point to KH were recorded.
Data regarding the causes of delay to KH and subsequent disposition were categorized as follows:
Source #1: Patient/caregiver-related factors such as lack of recognition of symptoms
Source #2: Financial issues – delay in seeking medical attention in order to gather finances
Source #3: Medical-related factors such as a misdiagnosis, incorrect management of the correct diagnosis, or the limited availability of resources at outside institutions
Source #4: Delays in the provision of neurosurgical care (e.g., availability of operating room time).
In cases of difficulty determining whether a time period would be classified as a source of delay, discussions were held between authors to reach a resolution. For example, if the parents of a child born at home noticed a myelomeningocele at birth but sought medical attention 2–3 days later, this was considered a Source #1 delay. Meanwhile, a prolonged admission to the local hospital for the management of sepsis in a patient with a nonleaking myelomeningocele was not considered as a source of delay. A Source #4 delay would be a case in which the delay to procurement of neurosurgical care was attributed to resource limitations (e.g. OR time) or a delay in diagnosis.
Average distances from KH were estimated based on the patient's city/town of origin and Google Maps™.
Description of center
KH is situated in Kijabe, a small town located just over an hour by road north-west of Nairobi, Kenya. The neurosurgical department at the center has been developed only recently and is headed by an American academic neurosurgeon formerly practicing in the United States (ALA). It currently offers neurosurgical care primarily to the pediatric patients from various locations across Kenya and some neighboring countries. Adult neurosurgical care is provided on an emergent or a limited elective basis.
Study population
All patients admitted to the neurosurgical department at KH (adult or pediatric), within the selected time intervals, and regardless of whether operative or medical/conservative intervention was selected.
Statistical analysis
Descriptive statistics were used for assessment of demographics and epidemiology of pathologies. The Kruskal–Wallis test for nonparametric variables was used to determine whether an overall significant difference with regard to the amount of delay was present among the various diagnoses. Should this be the case, the Mann–Whitney U test would be used as a post-hoc test to conduct pairwise comparisons within groups. Based on the availability of prior data regarding the extent of delay with congenital anomalies and intracranial tumors (adults),[2,19,20] we wished to determine whether there would be a significant difference with regard to the median period of delay in the “prehospital” and “primary care” frames of possible delay between HCP vs NTD, HCP vs NTD + HCP, NTD vs NTD + HCP, HCP vs tumors, and NTD vs tumors. The Bonferroni correction was applied to the alpha level of significance (0.05) according to number of comparisons conducted; therefore, for any of these comparisons to be considered significant, an alpha level of 0.01 (0.05/5) was used. IBM SPSS version 22.0 (SPSS, Chicago, IL) was used to conduct all statistical analyses.
Ethics
This study was approved by the Institutional Research Ethics Board at KH.
RESULTS
As part of the retrospective component of this study, a total of 197 patient charts were obtained by the health records department at KH. Nine charts did not belong to neurosurgical patients and were erroneously selected, resulting in 188 charts available for review. Thirty-one patients admitted during this 3-month period had been previously admitted to KH; inclusion of these records yielded an additional 49 records for a total of 237 admissions. A total of 95 admissions over a period of 3 weeks (June 2–20, 2014) were available for analysis in the prospective segment of the study.
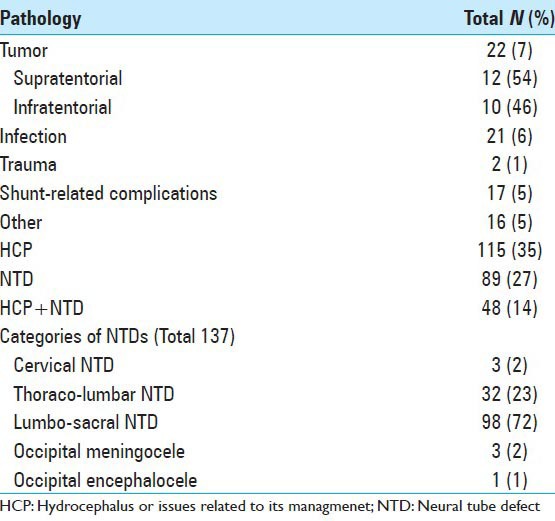
Patient demographics, both in the retrospective and prospective segments of the study, have been summarized in Table 1. There was an approximately even distribution with regard to gender. While the majority of patients were in the pediatric age range, patients aged as old as 56 years were also admitted and managed at KH. The majority of admissions were on an emergent basis, rather than elective, and most were managed operatively. The average distance travelled by patients varied from 25 to 2313 km. Patients had reached KH from cities as far as Mogadishu (Somalia) and Mwanza (Tanzania). The admitting diagnosis was HCP or related issues in 115 cases (35%), NTDs (in isolation or in combination with HCP) in 137 cases (41%), and infectious etiologies (e.g. UTI, exposed shunt tubing, cerebral abscess) in 21 cases (6%) [Table 2]. Accurate documentation of the root cause of HCP was not available.
Table 1.
Demographic summary of admissions to Kijabe Hospital
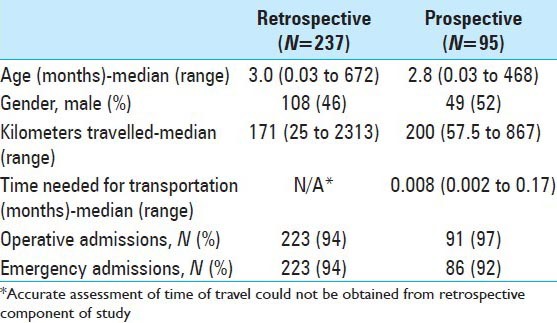
Table 2.
Analysis of the primary pathologies managed at Kijabe Hospital
From the retrospective component of the study, documentation of the length of time for Frame #1 (prehospital delay) was not available in 130 of the admission records, which affected the estimations for both Frame #1 and Frame #2 (delay at primary care). Similarly, it was not possible to accurately determine whether financial barriers or means of transportation contributed to the delay in presentation from this retrospective component of the study (Figure 1a). These gaps were overcome using the prospective component (Figure 1b). Delay at primary care (Time frame #2) were the leading contributor (statistically significant) while financial constraints (Source #2, applicable to all Time frames) were second [Table 3]. Thirty-nine cases were affected by multiple sources of delay. Travel time was not a significant source of delay contributing a median of only 6 h [Table 1]. Patients most often utilized a combination of methods of travel with private automobiles being the most frequently used, followed by buses and motorcycles (data not shown).
Figure 1.
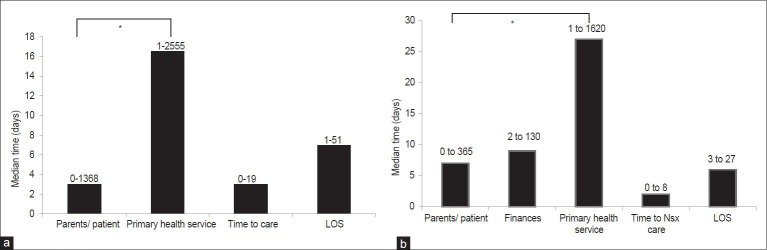
The median time (days) experienced by patients from symptom onset to disposition as obtained from the retrospective (a) and prospective (b) components of the study
Table 3.
The incidence of various sources of delay affecting care of patients admitted to Kijabe Hospital
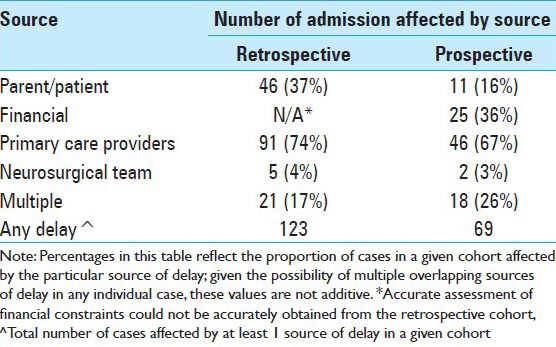
A total of seven cases (2%) were affected by delay secondary to factors influenced by the neurosurgical service affecting the time to the procurement of neurosurgical care [Table 3]. Overall, the median time to receiving neurosurgical care and the overall length of stay was 3 and 7 days, respectively.
Combining the data from the two components of the study, it was found that patients experiencing the longest period of delay were primarily those with CNS tumors, followed by HCP [Figure 2]. Upon identifying a significant within-group difference among the various pathologic entities using the Kruskal–Wallis test (P < 0.05), post-hoc pairwise comparisons were conducted using the Mann–Whitney U test. With a combined prehospital and primary care median delay of 49 days, the diagnosis of HCP was associated with a significantly longer delay compared with NTD which had a combined median prehospital and primary care delay of 16 days (Mean rank 119 vs 89, P < 0.01). At a combined median prehospital and primary care delay of 19.5 days, HCP + NTD had a significantly lower amount of delay compared with HCP (Mean rank 44 vs 119, P < 0.01). At a combined median prehospital and primary care delay of 200.5 days, tumors were also statistically more likely to present with a significant delay compared with NTDs (Mean rank 22 vs 89, P < 0.01). The difference in delay between HCP and tumors was not significant (P = 0.06).
Figure 2.
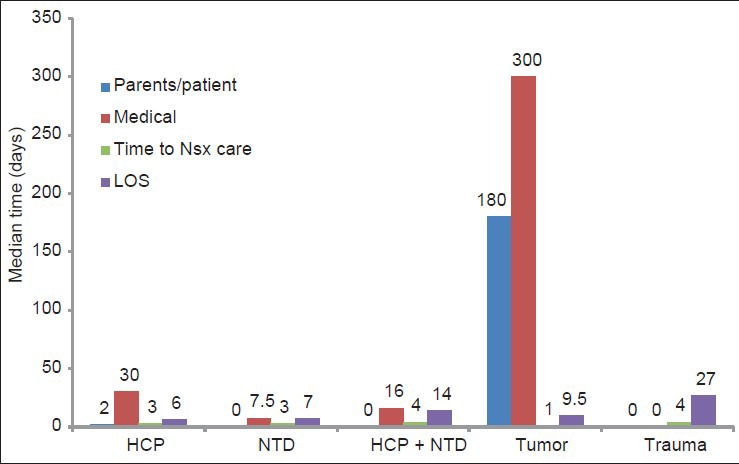
The median time (days) experienced by patients at various stages of their care, based on pathology. For this analysis, data from the retrospective and prospective arms of the study were combined
DISCUSSION
This cross-sectional, mixed-methods study is the first of its kind to be conducted with the purpose of assessing and quantifying the sources of delay to the provision of primarily pediatric neurosurgical care with a broad range of presenting pathologies in the developing world. While the focal point of this study was based in KH, the principal findings of this study may be applicable to the needs of other rural neurosurgical centers as well. Strengthened by the relatively large sample size analyzed, we have identified areas of deficiency in the regional healthcare and local administrative system, which can be improved in order to decrease delay and improve the delivery of patient care.
Seldom were patients admitted on an elective basis at KH. This not only reflects the urgent nature of neurosurgical pathologies but also the fact that many out of hospital cases are not recognized in time and present at an advanced stage of the pathology. The majority of admissions (76%) were attributable to HCP and NTDs. In a prospective study conducted during the year 2005 at a neurosurgical center in Ikeja, Nigeria, 64% of the pediatric patients were found to be affected by congenital anomalies.[2] Therefore, it is disappointing that these highly preventable pathologies continue to be prevalent. With regards to identifying the factors responsible for delayed presentations in strictly congenital anomalies (as defined by >6 months from birth) another prospective study in Nigeria found finances and lack of knowledge (e.g., assuming child's pathology to be fatal, other competing life priorities) to be the main culprits.[20] In our study, the underlying cause of HCP was not distinctly quantifiable in this study. Although previous studies have suggested that postinfectious HCP is the most common form in East African countries such as Uganda,[17,32] clinical experience suggests that HCP secondary to spina bifida is the most prevalent in Kenya. Despite the drive to improve peri-natal care of mothers and infants and the well-documented benefits of folic acid supplementation, postinfectious HCP and NTDs continue to be a great public health concern.[12,21]
Although previous epidemiological studies assessing the burden of surgical disease in developing nations have found trauma to be one of the most common reasons for admission,[6,30] trauma-related cases comprised the lowest percentage of admission to KH. While this can be related to the lower incidence of trauma in the pediatric population, the difficulty with regard to timely accessibility to KH, secondary to distance and road conditions, cannot be overlooked.[24]
While a great proportion of delays were attributable to patients/parents not recognizing the signs and symptoms of the pathology, delays faced within the health care system represented the highest incidence and time quantity within our study. This is in contrast to our original hypothesis and the findings of the study by Idowu and Apemiye in which patient-related matters contributed to 62% of the delays.[19] The root cause of both patient- and healthcare-related sources of delay is multi-factorial and each need to be addressed adequately in order to alleviate delay.
In seeking medical attention, possible factors for delay include lack of patient awareness about signs and symptoms, geographical accessibility, and resource-related barriers.[25] Idowu's study highlights the faith of the general population in traditional medicine and spiritual healers instead of modern medical care.[19] As suggested by these authors, to address the issue of awareness, education is paramount. At the level of the individual, improving knowledge and skills with regard to peri-natal care and the typical signs and symptoms of common pathologies is essential. Education can help increase overall awareness within communities as well. While these needs can be addressed through formal academic means, simple advertisements and governmental public service announcements can be of great utility.
The cost of transportation and hospitalization are a major deterrent for patients.[25] Currently organizations such as WATSI (named after the city in Costa Rica where the founder of the organization first formulated the idea), a crowd-gathering mode of fundraising, have played a pivotal role for gathering the necessary finances for individual patients in need of medical care.[1] While the development/expansion of such movements is helpful, more grass-roots forms of community funding are necessary as well. For example, a community-based risk sharing scheme has been previously developed in northern Kenya whereby individual members and health providers work together to collect funds for emergency medical situations; this not only helps alleviate financial constraints to some extent, it also helps build trust between the community and the health system.[23] Similar community measures have been implemented elsewhere as well.[16]
Many cases of HCP or malignancy were wrongfully diagnosed and managed as infectious diseases such as malaria, typhoid, and brucellosis. This was reflected in the significantly prolonged period of delay in presentation of patients with these diagnoses compared with NTD. Furthermore, several cases were noted in which a patient with a myelomeningocele was managed at the outside institution with daily dressing changes with no definitive intervention planned. While inadequate knowledge on behalf of the local physicians regarding the pathology is a likely factor,[4] the lack of awareness of KH as a resource or the absence of an established referral process are other possible contributors to this issue. Through improved access to the world-wide web, even in developing nations, many physicians have been able to consult the neurosurgical service at KH for an opinion. However, this accessibility is not universal. Thus, an increased exposure of KH as an established pediatric neurosurgical center and improvements in online access create the opportunity for timely specialist opinions and referrals. Unfortunately, many hospitals in developing nations either lack an established triage and referral process or the guidelines are not followed formally.[8,14]
The role of nongovernmental organizations as the missing link
The importance of nongovernmental organizations (NGOs) in developing nations cannot be underestimated. The mandate of most NGOs is typically focused on a specific field within a specific cohort of the community. Successful NGOs possess proficiency of knowledge and/or technical expertise in their field of focus, along with a good rapport with the community they serve.[13] Issues preventing further success of NGOs relate to financial and infrastructural support, which can be provided by corporate and governmental organizations, respectively. A transparent partnership between government bodies, NGOs, and the corporate sector can provide a solution to many of the health-related issues in the developing world. While there are many ethical considerations, a functional partnership can provide positive results as demonstrated with the achievements gained by the World Heart Foundation in the past decade.[3] Other such successful partnerships include the coalition between Merck, Onchocerciasis Elimination Program for the Americas, and the Carter Center to raise funds for the several South and Central American governments to battle Onchocerciasis through the free distribution of ivermectin. In this example, NGOs contributed expertise on research and development, disease screening and prevention, and outcome monitoring while Merck contributed financially.[7]
As an adjunct to the aforementioned community-based measures of financial support, NGOs can participate in fundraising activities and coordinating medical insurance foundations serving the local community.[13] In order to develop triage and referral guidelines, a concerted effort between NGOs, public health researchers, and governmental agencies will be necessary.[5] Organizations with expertise in administrative or managerial positions can be recruited to maintain quality control and guideline adherence.[13] These efforts can be further expanded to develop and streamline standardized methods of data collection (e.g., through the use of forms), which would not only improve organization but would also enable internal reviews and epidemiological analyses in the future.[15] Government and corporate institutions can assist in financing these endeavors.
Limitations
This study was limited by several factors that prevented a comprehensive quantification and analysis of factors resulting in delay. The subjective nature of classifying cases of delay introduces a source of bias. The retrospective component of the study was in some cases limited by inaccurate chart retrieval and inconsistent documentation of history. These deficiencies have been previously identified as substantial barriers to instituting standardized measures of success in developing nations, which prevent progress at the institution and in the field in general.[27] In addition, they also result in an inefficient use of health care workers as valuable resources due to the time investment required to gather necessary medical information.[15] Although the prospective component improved upon these short-comings, the cross-sectional nature of the study and the fact that it was conducted over an arbitrary 2-week period introduces the possibility of sampling bias. During this short period of analysis, it is possible that a true representation of disease epidemiology or delay factors was not captured. For example, while HCP and NTDs together comprised 76% of admission in this study, they typically constitute 65% of admissions to KH (data not shown).
With these limitations considered, the current study represents the first of its kind to assess and quantify the sources of delay to the provision of primarily pediatric neurosurgical care, assessing a variety of diagnoses, in a high-volume rural setting in the developing world. In addition, we have also identified and analyzed various cultural, academic, infrastructural, and administrative factors that contribute to the overall delay to care. Furthermore, we have provided an outline of steps that can be taken to improve upon these issues. Future prospective studies, conducted over a longer time period and sampling neurosurgical settings from a diverse set of developing nations, would assist in better identifying and quantifying additional sources of delay; findings from such multi-centric studies would be of particular value given their improved external validity. Studies such as the current one help initiate the drive toward devising strategies that can be used to decrease delays in a field in which time is of the essence. A strong and ethically sound partnership between NGOs, government organizations, and corporate sponsors can provide the means necessary for the development and success of initiatives aimed at reducing these delays.
CONCLUSIONS
Public health outreach efforts, particularly targeting rural regions, need to be expanded as preventative strategies for some of the most common pediatric nervous system disorders. Such efforts would include education about the importance of folic acid and its cost-free distribution within local governmental health centers
Community-based strategies can be effective means of addressing many financial and logistic issues with regard to accessing timely medical care; these need to be explored and developed further
Formal triage guidelines and referral protocols are needed, both at the local hospital level and at the level of the ministry of health, in order to create a safer and more efficient strategy that would ensure access to timely medical care for all patients
Strategies aimed at improving data collection and storage are necessary to increase the efficiency of the work flow and to enable self-evaluation and improvements by hospitals
A transparent and ethical collaboration between NGOs, governmental organizations, and corporate partners has great potential for advancing these efforts.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2015/6/1/32/152141
Contributor Information
Alireza Mansouri, Email: alireza.mansouri@utoronto.ca.
Vivien Chan, Email: vivvy.chan@utoronto.ca.
Veronica Njaramba, Email: nveronicahwacu@yahoo.com.
David W. Cadotte, Email: davecadotte@gmail.com.
A. Leland Albright, Email: l.albright@neurosurgery.wisc.edu.
Mark Bernstein, Email: mark.bernstein@uhn.ca.
REFERENCES
- 1.2014. [Last cited on 2014 Jun 21]. Available from: https://watsi.org/about. WATSI .
- 2.Adeleye AO, Olowookere KG. Central nervous system congenital anomalies: A prospective neurosurgical observational study from Nigeria. Congenit Anom (Kyoto) 2009;49:258–61. doi: 10.1111/j.1741-4520.2009.00241.x. [DOI] [PubMed] [Google Scholar]
- 3.Bayes de Luna A, Tse TF, de Figueiredo MB, Maranhao M, Voute J, Nishtar S, et al. World Heart Day: A World Heart Federation enterprise promoting the prevention of heart disease and stroke across the world. Circulation. 2003;108:1038–40. doi: 10.1161/01.CIR.0000089504.27796.2C. [DOI] [PubMed] [Google Scholar]
- 4.Bickler G. Getting ahead of the curve while shifting the balance of power--how will they work at local level? Commun Dis Public Health. 2002;5:167. [PubMed] [Google Scholar]
- 5.Bickler SW, Kyambi J, Rode H. Pediatric surgery in sub-Saharan Africa. Pediatr Surg Int. 2001;17:442–7. doi: 10.1007/s003830000516. [DOI] [PubMed] [Google Scholar]
- 6.Bickler SW, Sanno-Duanda B. Epidemiology of paediatric surgical admissions to a government referral hospital in the Gambia. Bull World Health Organ. 2000;78:1330–6. [PMC free article] [PubMed] [Google Scholar]
- 7.Blanks J, Richards F, Beltran F, Collins R, Alvarez E, Zea Flores G, et al. The Onchocerciasis Elimination Program for the Americas: A history of partnership. Rev Panam Salud Publica. 1998;3:367–74. doi: 10.1590/s1020-49891998000600002. [DOI] [PubMed] [Google Scholar]
- 8.Bossyns P, Van Lerberghe W. The weakest link: Competence and prestige as constraints to referral by isolated nurses in rural Niger. Hum Resour Health. 2004;2:1. doi: 10.1186/1478-4491-2-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bronsard A, Geneau R, Shirima S, Courtright P, Mwende J. Why are children brought late for cataract surgery? Qualitative findings from Tanzania. Ophthalmic Epidemiol. 2008;15:383–8. doi: 10.1080/09286580802488624. [DOI] [PubMed] [Google Scholar]
- 10.Cadotte DW, Viswanathan A, Cadotte A, Bernstein M, Munie T, Freidberg SR, et al. The consequence of delayed neurosurgical care at Tikur Anbessa Hospital, Addis Ababa, Ethiopia. World Neurosurg. 2010;73:270–5. doi: 10.1016/j.wneu.2010.02.017. [DOI] [PubMed] [Google Scholar]
- 11.Dye TD, Bogale S, Hobden C, Tilahun Y, Hechter V, Deressa T, et al. Complex care systems in developing countries: Breast cancer patient navigation in Ethiopia. Cancer. 2010;116:577–85. doi: 10.1002/cncr.24776. [DOI] [PubMed] [Google Scholar]
- 12.Eichholzer M, Tonz O, Zimmermann R. Folic acid: A public-health challenge. Lancet. 2006;367:1352–61. doi: 10.1016/S0140-6736(06)68582-6. [DOI] [PubMed] [Google Scholar]
- 13.Ejaz I, Shaikh BT, Rizvi N. NGOs and government partnership for health systems strengthening: A qualitative study presenting viewpoints of government, NGOs and donors in Pakistan. BMC Health Serv Res. 2011;11:122. doi: 10.1186/1472-6963-11-122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.English M, Esamai F, Wasunna A, Were F, Ogutu B, Wamae A, et al. Assessment of inpatient paediatric care in first referral level hospitals in 13 districts in Kenya. Lancet. 2004;363:1948–53. doi: 10.1016/S0140-6736(04)16408-8. [DOI] [PubMed] [Google Scholar]
- 15.English M, Esamai F, Wasunna A, Were F, Ogutu B, Wamae A, et al. Delivery of paediatric care at the first-referral level in Kenya. Lancet. 2004;364:1622–9. doi: 10.1016/S0140-6736(04)17318-2. [DOI] [PubMed] [Google Scholar]
- 16.Essien E, Ifenne D, Sabitu K, Musa A, Alti-Mu’azu M, Adidu V, et al. Community loan funds and transport services for obstetric emergencies in northern Nigeria. Int J Gynaecol Obstet. 1997;59(Suppl 2):S237–44. doi: 10.1016/s0020-7292(97)00171-9. [DOI] [PubMed] [Google Scholar]
- 17.Garton HJ, Piatt JH., Jr Hydrocephalus. Pediatr Clin North Am. 2004;51:305–25. doi: 10.1016/j.pcl.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 18.Heinsbergen I, Rotteveel J, Roeleveld N, Grotenhuis A. Outcome in shunted hydrocephalic children. Eur J Paediatr Neurol. 2002;6:99–107. doi: 10.1053/ejpn.2001.0555. [DOI] [PubMed] [Google Scholar]
- 19.Idowu OE, Apemiye RA. Delay in presentation and diagnosis of adult primary intracranial neoplasms in a tropical teaching hospital: A pilot study. Int J Surg. 2009;7:396–8. doi: 10.1016/j.ijsu.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 20.Komolafe EO, Komolafe MA, Adeolu AA. Factors implicated for late presentations of gross congenital anomaly of the nervous system in a developing nation. Br J Neurosurg. 2008;22:764–8. doi: 10.1080/02688690802485113. [DOI] [PubMed] [Google Scholar]
- 21.Laurence KM, James N, Miller M, Campbell H. Increased risk of recurrence of pregnancies complicated by fetal neural tube defects in mothers receiving poor diets, and possible benefit of dietary counselling. Br Med J. 1980;281:1592–4. doi: 10.1136/bmj.281.6255.1592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Levine AC, Presser DZ, Rosborough S, Ghebreyesus TA, Davis MA. Understanding barriers to emergency care in low-income countries: View from the front line. Prehosp Disaster Med. 2007;22:467–70. doi: 10.1017/s1049023x00005240. [DOI] [PubMed] [Google Scholar]
- 23.Macintyre K, Hotchkiss DR. Referral revisited: Community financing schemes and emergency transport in rural Africa. Soc Sci Med. 1999;49:1473–87. doi: 10.1016/s0277-9536(99)00201-4. [DOI] [PubMed] [Google Scholar]
- 24.Mansouri A, Okechi H, Albright AL, Bernstein M. Reconnaissance mission to the neurosurgical department in Kijabe Hospital, Kenya: A call for the submission of ideas and strategies. World Neurosurg. 2014;81:e14–6. doi: 10.1016/j.wneu.2013.09.049. [DOI] [PubMed] [Google Scholar]
- 25.Mwangome FK, Holding PA, Songola KM, Bomu GK. Barriers to hospital delivery in a rural setting in Coast Province, Kenya: Community attitude and behaviours. Rural Remote Health. 2012;12:1852. [PubMed] [Google Scholar]
- 26.Park BE. The African experience: A proposal to address the lack of access to neurosurgery in rural sub-Saharan Africa. World Neurosurg. 2010;73:276–9. doi: 10.1016/j.wneu.2010.02.016. [DOI] [PubMed] [Google Scholar]
- 27.Reynolds TA, Mfinanga JA, Sawe HR, Runyon MS, Mwafongo V. Emergency care capacity in Africa: A clinical and educational initiative in Tanzania. J Public Health Policy. 2012;33(Suppl 1):S126–37. doi: 10.1057/jphp.2012.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tarcan T, Onol FF, Ilker Y, Alpay H, Simsek F, Ozek M. The timing of primary neurosurgical repair significantly affects neurogenic bladder prognosis in children with myelomeningocele. J Urol. 2006;176:1161–5. doi: 10.1016/j.juro.2006.04.042. [DOI] [PubMed] [Google Scholar]
- 29.Telfer ML, Rowley JT, Walraven GE. Experiences of mothers with antenatal, delivery and postpartum care in rural Gambia. Afr J Reprod Health. 2002;6:74–83. [PubMed] [Google Scholar]
- 30.Thanni LO, Shonubi AM, Akiode O. A retrospective audit of paediatric surgical admission in a sub-urban tertiary hospital. West Afr J Med. 2005;24:10–2. doi: 10.4314/wajm.v24i1.28154. [DOI] [PubMed] [Google Scholar]
- 31.Urassa E, Massawe S, Lindmark G, Nystrom L. Operational factors affecting maternal mortality in Tanzania. Health Policy Plan. 1997;12:50–7. doi: 10.1093/heapol/12.1.50. [DOI] [PubMed] [Google Scholar]
- 32.Warf BC. Hydrocephalus in Uganda: The predominance of infectious origin and primary management with endoscopic third ventriculostomy. J Neurosurg. 2005;102(1 Suppl):S1–15. doi: 10.3171/ped.2005.102.1.0001. [DOI] [PubMed] [Google Scholar]