

Several small molecule tyrosine kinase inhibitors (TKIs) inhibit c-Kit, an effect associated with myelosuppression and hair depigmentation. We studied a panel of approved and investigational TKIs for inhibitory activity against FLT3 and c-Kit, and on hematopoietic progenitor cells. Potent c-Kit inhibitors such as dasatinib, pazopanib, and quizartinib demonstrated the greatest disruption of hematopoietic progenitor cells, while sorafenib, which has negligible activity against c-Kit, demonstrated only minimal disruption. Our data highlight the importance of determining a therapeutic index between the targeted receptor and c-Kit for TKIs used to treat malignancies in order to maintain normal hematopoiesis and improve outcomes.
Myelosuppression is a common adverse event in new drug development in oncology. Many tyrosine kinase inhibitors (TKIs) have activity against c-Kit, a receptor tyrosine kinase (RTK) which is essential for normal hematopoiesis.1 The c-Kit receptor is an important marker of long-term hematopoietic stem cells, and it also plays an important role in hair and skin pigmentation. For example, the W mouse, in which the function of c-Kit is impaired, has white spots, anemia, and reduced megakorycytes, and c-Kit knockouts in transgenic mice is embryonic lethal (reviewed by Lyman and Jacobsen1). Patients treated with TKIs that inhibit c-Kit, therefore, are at risk for myelosuppression.2 In vivo c-Kit inhibition is also associated with hair depigmentation (Figure 1A).3 Drugs such as pazopanib and sunitinib, which have activity against c-Kit, do not induce myelosuppression in solid tumor patients when used as single agents. In contrast, dasatinib and imatinib, which also inhibit c-Kit, have been associated with myelosuppression in patients with Philadelphia-positive (Ph+) leukemia.4 In patients with relapsed/refractory FLT3/ITD acute myeloid leukemia (AML), treatment with the FLT3 inhibitor quizartinib was associated with myelosuppression, whereas in a similar patient population, a different FLT3 inhibitor, sorafenib, induced no myelosuppression.5,6 To better understand the relationship between inhibition of c-Kit, FLT3, and marrow suppression, we studied a series of different TKIs using bone marrow progenitor cell assays and immunoblots.
Figure 1.
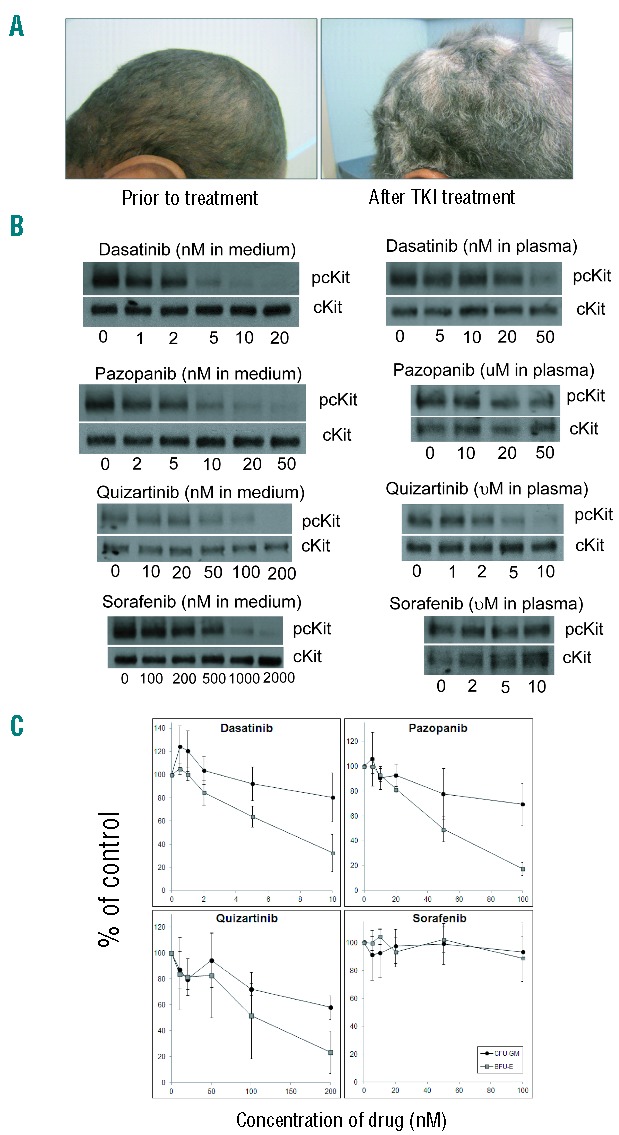
(A) An acute myeloid leukemia patient before treatment (left) and 54 days 15 after treatment (right) with the c-Kit/FLT3 inhibitor, PLX3397. This compound is currently being studied in a phase I trial (clinicaltrials.gov identifier 01349049); pharmacokinetic data are not yet available for PLX3397, and so it was not included in this study. (B) TF-1 cells were treated with drug for 1 h in cell culture medium or plasma, lysed, and immunoblotted for phospho- and total c-Kit. (C) Normal human bone marrow was collected and mononuclear cells were isolated. Mononuclear cells were plated in 35 mm dishes at a concentration of 100,000 cells per mL in MethoCult containing various concentrations of the indicated TKI in quadruplicate. Plates were analyzed 10–14 days later by morphology for total number of CFU-GM and BFU-E colonies. For each drug, the assay was performed using three separate marrow samples and the results were averaged.
Cell lines were cultured as previously described.2 TF-1 cells were obtained from the American Type Culture Collection (ATCC; Manassas, VA, USA) and grown in RPMI supplemented with GM-CSF (Invitrogen, Grand Island, NY, USA). Quizartinib was obtained from Ambit Biosciences (San Diego, CA, USA). Crenolanib was obtained from Arog Pharmaceuticals (Dallas, TX, USA). Dasatinib, pazopanib, and imatinib were obtained from LC Laboratories (Woburn, MA, USA). Electrophoresis, immunoblotting, and hematopoietic progenitor cell assays were performed as described.2 Cytokines used included SCF, G-CSF, GM-CSF, IL-3, IL-6, and erythropoietin. Unused portions of bone marrow from normal donors were collected under an institutional review board-approved Tumor and Cell Procurement Bank at Johns Hopkins (supported by grant P30CA006973-44). All donors gave informed consent according to the Declaration of Helsinki.
Dasatinib is a multi-targeted TKI with activity against Bcr-Abl, SRC, and c-Kit.5 The concentration of dasatinib necessary to inhibit 50% of base-line c-Kit activity (IC50) in TF-1 cells stimulated with stem cell factor (SCF) is 1.5 nM in culture medium and 30 nM in 100% human plasma (Figure 1B). The drug has a relatively short half-life of 3–5 h and steady state concentrations are in the range of 20–40 nM.5 In progenitor cell assays, dasatinib had a modest effect on the formation of GM-CFUs (granulocyte-monocyte colony forming units), and a greater effect on the formation of erythroid colonies (Figure 1C). Dasatinib has been reported to cause myelosuppression in leukemia patients,4 as well as hair depigmentation.6 Pazopanib, a TKI approved for use in some solid tumors, is reported to be a potent inhibitor of VEGFR, PDGFR, and c-Kit.7 We found it to have an IC50 against c-Kit in culture medium of 3.7 nM. While pazopanib has a seemingly high IC50 against c-Kit in human plasma of 36 μM (due to high plasma protein binding) (Figure 1B), patients achieve trough drug levels over 50 μM.7 In progenitor cell assays, pazopanib, at concentrations corresponding to those routinely achieved in patients, inhibited erythroid and myeloid progenitor cell activity to a similar degree as dasatinib (Figure 1C). Hair depigmentation is listed as a common adverse event in the FDA label for pazopanib, again, indicative of in vivo c-Kit inhibition. While both dasatinib and pazopanib are potent vivo inhibitors of c-Kit, of the two drugs, only dasatinib has been reported to cause myelosuppression as monotherapy.4,7 Pazopanib is used exclusively to treat patients with solid tumors (who presumably have intact marrow function). However, when combined with cytotoxic drugs, pazopanib appears to exacerbate the chemotherapy-induced myelosuppression.8 Similarly, sunitinib, as monotherapy for solid tumor patients, is not associated with significant myelosuppression. However, in leukemia patients or in solid tumor patients in combination with chemotherapy, sunitinib exacerbates myelosuppression.9,10 A simple explanation for these findings is that c-Kit inhibition by itself does not induce clinically significant myelosuppression in the setting of normal bone marrow function.
Inhibition of c-Kit, therefore, correlates with hair depigmentation, inhibition of erythroid precursor activity in vitro, and, in leukemia patients, myelosuppression. Given the redundant signaling properties of c-Kit and FLT3,1 simultaneous inhibition of FLT3 and c-Kit could result in profound myelosuppression. Sorafenib is a potent FLT3 TKI (IC50 in culture medium 3–5 nM) that has demonstrated efficacy in the treatment of relapsed/refractory FLT3/ITD AML patients.11 There is no reported inhibition of c-Kit by sorafenib, nor have there been any reports of myelosuppression (even in combination with chemotherapy). These observations are consistent with the results of our immunoblot (Figure 1B) and with progenitor cell assays (Figure 1C). In contrast, quizartinib is a potent FLT3 inhibitor (IC50 in culture medium 2 nM; in plasma 18 nM), and a modestly potent c-Kit inhibitor with an IC50 in culture medium of 28 nM. AML patients readily achieve micromolar plasma concentrations of this agent,12 and myelosuppression was observed in leukemia patients treated with quizartinib.13 Quizartinib inhibits both myeloid and erythroid hematopoietic progenitor cell activity (Figure 1C). Given that FLT3 inhibition alone (by sorafenib) did not inhibit colony activity, we conclude that quizartinib-induced myelosuppression is probably mediated through inhibition of c-Kit, rather than inhibition of FLT3. Interestingly, the most common clinical response to single agent therapy with quizartinib has been a complete remission with incomplete count recovery (“CRi”).5,13 The failure to recover normal hematopoietic function may be due in part to the inhibition of c-Kit by quizartinib.
While FLT3 inhibition by itself has no effect on hematopoiesis, it possibly still contributes to c-Kit-induced marrow suppression. Exogenous FLT3 ligand (FL) shifts the dose response to FLT3 inhibitors upward.14 If FLT3 inhibition were contributing to the suppression of hematopoietic progenitor cell induced by quizartinib, then the addition of FL would be predicted to blunt the inhibitory effect of quizartinib. In progenitor cell assays, we saw no significant difference in effect with 200 nM quizartinib with or without exogenous FL (10 ng/mL) (data not shown), suggesting that FLT3 inhibition does not contribute to marrow suppression from quizartinib.
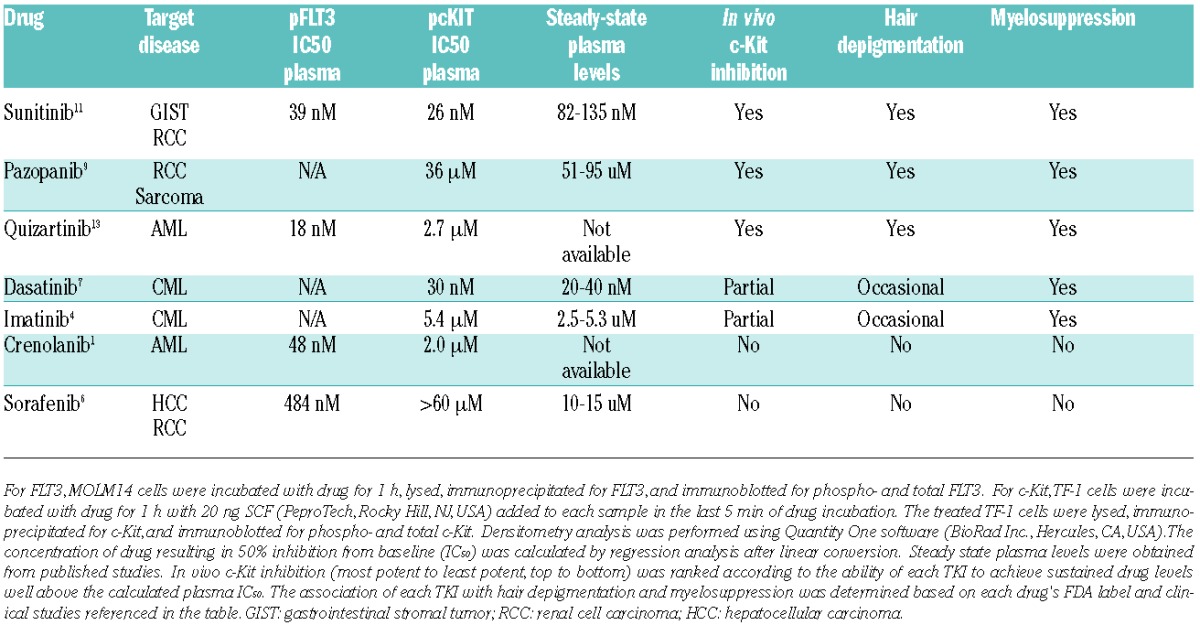
We conclude that inhibition of c-KIT can translate into clinically significant marrow suppression, particularly when it occurs in the setting of cytotoxic chemotherapy, or when it is induced in a patient with a marrow disorder such as leukemia. The more potent c-Kit inhibitors impair erythroid, and myeloid progenitor cell function, but FLT3 inhibition probably has little effect on hematopoiesis. Table 1 lists seven TKIs according to their activity against both FLT3 and c-Kit receptors in culture medium and 100% human plasma. Each TKI was ranked according to its relative potency against c-Kit in vivo, using published pharmacokinetic data (when available), in vitro potency, the occurrence of hair depigmentation and myelosuppression. Given the clinical consequences of myelosuppression, the relative difference in inhibitory activity between the targeted kinase and c-Kit represents an important therapeutic index that must be accounted for in the development of TKIs. Hair depigmentation can represent a useful clinical surrogate for this phenomenon.
Table 1.
Relative activity against FLT3 and c-KIT, and myelosuppressive activity of tyrosine kinase inhibitors.
Footnotes
Funding: This work was supported by the NCI Leukemia SPORE P50 CA100632-11.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Lyman SD, Jacobsen SE. c-kit ligand and Flt3 ligand: stem/progenitor cell factors with overlapping yet distinct activities. Blood. 1998;91(4):1101–34. [PubMed] [Google Scholar]
- 2.Galanis A, Ma H, Rajkhowa T, et al. Crenolanib is a potent inhibitor of FLT3 with activity against resistance-conferring point mutants. Blood. 2014;123(1):94–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moss KG, Toner GC, Cherrington JM, Mendel DB, Laird AD. Hair depigmentation is a biological readout for pharmacological inhibition of KIT in mice and humans. J Pharmacol Exp Ther. 2003;307(2):476–80. [DOI] [PubMed] [Google Scholar]
- 4.Talpaz M, Shah NP, Kantarjian H, et al. Dasatinib in imatinibresis tant Philadelphia chromosome-positive leukemias. N Engl J Med. 2006;354(24):2531–41. [DOI] [PubMed] [Google Scholar]
- 5.Demetri GD, Lo Russo P, MacPherson IR, et al. Phase I dose-escalation and pharmacokinetic study of dasatinib in patients with advanced solid tumors. Clin Cancer Res. 2009;15(19):6232–40. [DOI] [PubMed] [Google Scholar]
- 6.Brazzelli V, Grasso V, Barbaccia V, et al. Hair depigmentation and vitiligo-like lesions in a leukaemic paediatric patient during chemotherapy with dasatinib. Acta dermato-venereologica. 2012; 92(2):218–9. [DOI] [PubMed] [Google Scholar]
- 7.Hurwitz HI, Dowlati A, Saini S, et al. Phase I trial of pazopanib in patients with advanced cancer. Clin Cancer Res. 2009. 15;15(12):4220–7. [DOI] [PubMed] [Google Scholar]
- 8.Plummer R, Madi A, Jeffels M, et al. A Phase I study of pazopanib in combination with gemcitabine in patients with advanced solid tumors. Cancer Chemother Pharmacol. 2013;71(1):93–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fiedler W, Serve H, Dohner H, et al. A phase 1 study of SU11248 in the treatment of patients with refractory or resistant acute myeloid leukemia (AML) or not amenable to conventional therapy for the disease. Blood. 2005;105(3):986–93. [DOI] [PubMed] [Google Scholar]
- 10.Crown JP, Dieras V, Staroslawska E, et al. Phase III trial of sunitinib in combination with capecitabine versus capecitabine monotherapy for the treatment of patients with pretreated metastatic breast cancer. J Clin Oncol. 2013;31(23):2870–8. [DOI] [PubMed] [Google Scholar]
- 11.Borthakur G, Kantarjian H, Ravandi F, et al. Phase I study of sorafenib in patients with refractory or relapsed acute leukemias. Haematologica. 2011;96(1):62–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cortes JE, Kantarjian H, Foran JM, et al. Phase I study of quizartinib administered daily to patients with relapsed or refractory acute myeloid leukemia irrespective of FMS-like tyrosine kinase 3-internal tandem duplication status. J Clin Oncol. 2013;31(29):3681–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cortes J, Perl A, Dombret H, et al. Final results of a Phase 2 open-label, monotherapy efficacy and safety study of Quizartinib (AC220) in patients 60 years of age with FLT3 ITD positive or negative relapsed/refractory acute myeloid leukemia. Blood. 2012;120:48a. [Google Scholar]
- 14.Sato T, Yang X, Knapper S, et al. FLT3 ligand impedes the efficacy of FLT3 inhibitors in vitro and in vivo. Blood. 2011;117(12):3286–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Burton E, Wong B, Zhang J, et al. The Novel Inhibitor PLX3397 Effectively Inhibits FLT3-Mutant AML. Blood. 2011;118:3632a. [Google Scholar]