

Highlights
-
•
Lower socioeconomic position associated with higher cumulative physiological burden.
-
•
Material factors (home ownership and income) completely attenuated the association.
-
•
Psychological factors (as measured using GHQ-12) did not attenuate the association.
-
•
Smoking attenuated the association by approximately one third.
-
•
Alcohol, physical activity and diet had no attenuation impact.
Keywords: Alcohol, Allostatic load, Diet, Health, Humans, Physiology, Physical activity, Socioeconomic status, Smoking
Abstract
Lower socioeconomic position (SEP), both accumulated across the life course and at different life-stages, has been found to be associated with higher cumulative physiological burden, as measured by allostatic load. This study aimed to identify what factors mediate the association between SEP and allostatic load, as measured through combining cardiovascular, metabolic and inflammatory markers. We explored the role of material, psychological and behavioral factors, accumulated across two periods in time, in mediating the association between SEP and allostatic load. Data are from the West of Scotland Twenty-07 Study, with respondents followed over five waves of data collection from ages 35 to 55 (n = 999). Allostatic load was measured by summing nine binary biomarker scores (‘1’ = in the highest-risk quartile) measured when respondents were 55 years old (wave 5). SEP was measured by a person’s accumulated social class over two periods All mediators and SEP were measured at baseline in 1987 and 20 years later and combined to form accumulated measures of risk. Material mediators included car and home ownership, and having low income. The General Health Questionnaire (GHQ-12) was used as the psychosocial mediator. Behavioral mediators included smoking, alcohol consumption, physical activity and diet. Path analysis using linear regressions adjusting for sex were performed for each of the potential mediators to assess evidence of attenuation in the association between lower SEP and higher allostatic load. Analyses by mediator type revealed that renting one’s home (approximately 78% attenuation) and having low income (approx. 62% attenuation) largely attenuated the SEP–allostatic load association. GHQ did not attenuate the association. Smoking had the strongest attenuating effect of all health behaviors (by 33%) with no other health behaviors attenuating the association substantially. Material factors, namely home tenure and income status, and smoking have important roles in explaining socioeconomic disparities in allostatic load, particularly when accumulated over time.
1. Background
Our bodies are often being challenged by changing and sometimes stressful environmental conditions that can alter the stability of our physiological systems. Allostasis is an active process where, given these challenges, our bodies attempt to maintain optimal physiological function by altering the operating set points or range (‘moving the goalposts’) of the physiological systems involved in adapting and reacting to these conditions (Sterling and Eyer, 1988). The wear and tear, or cumulative physiological burden, that occurs following the repeated activation of the allostatic response is known as allostatic load. Allostatic load is measured by combining several biomarker measures across an array of systems including the cardiovascular, metabolic and inflammatory systems, and has been shown to predict the risk of major health outcomes including heart disease and all-cause mortality (Seeman et al., 1997, 2004; Gruenewald et al., 2009; Karlamangla et al., 2006; Sabbah et al., 2008). Importantly, many of the individual components of allostatic load are not risk predictors for these same health outcomes, suggesting that the allostatic load construct could provide additional predictive power of disease risk over individual biomarkers. Assessing these biomarkers together as allostatic load helps us to understand the synergistic nature of the physiological burden on the body imposed by exposure to damaging environmental stressors. This could make allostatic load an important, early predictor of disease risk and improve our understanding of how physiological damage develops across the body.
There is growing evidence that allostatic load is socially patterned, with higher allostatic load associated with lower socioeconomic position (SEP), including SEP measured contemporaneously with allostatic load, as well as over time and during developmentally-important life stages such as childhood (measured distally to allostatic load) (Gruenewald et al., 2012; Gustafsson et al., 2011, 2012; Hawkley et al., 2011; Robertson et al., 2014). However, less is known about the potential pathways that link SEP and allostatic load. Three major mediating pathways have been suggested between SEP and health, namely material factors (e.g. income, employment status, ownership of material goods such as a car or home), psychosocial (e.g. stress)/psychological (e.g. distress) factors and health behaviors (e.g. smoking, alcohol consumption) (Fig. 1) Adler and Ostrove, 1999; Adler and Stewart, 2010. Given the evidence for links between SEP and health, SEP and allostatic load, and allostatic load and health, we propose that these same potential mediators could be involved in mediating the relationship between SEP and allostatic load. Given the theoretical links between the allostatic load concept and the stress response, and lower SEP and increased stressful environment (Baum et al., 1999; Brunner, 1997; Cohen et al., 2006), it would be expected that psychosocial/psychological factors would be important explanatory factors for the relationship between SEP and allostatic load (McEwen, 2001, 2006; Stewart, 2006). The socially patterned material factors linking SEP and allostatic load could relate to increased exposure to harmful conditions in the workplace, home and neighborhood, including toxins, damp, overcrowding, etc., as well as being interlinked to psychosocial factors (such as low control and high stress) that lead to psychological distress, which may play a role in both damaging and preventing repair to multiple physiological systems in the body. The carcinogens and health-damaging components in tobacco, alcohol, and some foods (and the lack of restorative efforts brought about by low physical activity) have the potential to impact on allostatic load, and are typically socially patterned. While these three pathways have distinct components, they are not mutually exclusive and are likely to combine in mediating the SEP–allostatic load association (Bartley, 2003). There has been evidence that some health behaviors, as well as a mix of psychosocial and psychological factors, explain some part of the SEP–allostatic load association (Gruenewald et al., 2012; Gustafsson et al., 2011, 2012; Hawkley et al., 2011). However, the number of studies are limited, the results inconsistent and material factors have had limited attention. The aim of this study was to examine the degree to which these material, psychological and behavioral factors explain the association between SEP and allostatic load, as measured through combining cardiovascular, metabolic and inflammatory markers. Given the strong links between stress and allostatic load, one would predict that psychosocial factors would play a major role in attenuating the SEP–allostatic load association. In this study we have used a measure of psychological distress, one mechanism linking psychosocial circumstances and health, and predicted that this psychological mediator would have the greatest attenuating effect, followed by material factors and then behavioral mediators.
Fig. 1.

Theoretical pathways linking SEP and health.
2. Methods
2.1. Study sample
Data were from the West of Scotland Twenty-07 Study, a community-based, prospective study, with respondents aged approximately 35 in 1987 (wave 1/W1) and followed up in a further four waves over the next 20 years. This is an important stage in the life course for the early development of disease and therefore a key life stage to investigate allostatic load. A more detailed description of the study is available elsewhere Benzeval et al. (2009). Data, including blood samples at wave 5 (W5) (2007/8), were collected by trained nurses in the homes of the study participants when respondents were aged approximately 55. Ethical approval for the baseline study was granted in 1986 by the GP Sub-Committee of Greater Glasgow Health Board and the ethics sub-committee of the West of Scotland Area Medical Committees. Wave 5 was approved by the Tayside Committee on Medical Research Ethics.
2.2. Biomarkers and allostatic load
Allostatic load was operationalized based on methods described by Seeman et al. (2008) and Bird et al. (2010), although this operationalization does not include any stress markers. The strengths and weaknesses of this operationalization are discussed later. The selected biomarkers represent three physiological systems: cardiovascular [systolic and diastolic blood pressure, and pulse rate]; metabolic [glycated hemoglobin (HbA1c), total cholesterol, high density lipoprotein (HDL) cholesterol and waist-hip ratio (WHR)]; and inflammatory [C-reactive protein (CRP) and serum albumin]. Adjustments were made to the biomarkers to account for the effect of medications. For those on anti-hypertensive medication, systolic and diastolic blood pressures were adjusted by adding 10 mmHG and 5 mmHG, respectively (Law et al., 2003). Respondents taking diabetes medication had 1% added to their HbA1c values (Kinshuck et al., 2013). Where respondents were taking statins, total cholesterol values had 21.24 mg/dL (1.18 mmol/l) added Law et al., 2003. Where respondents were taking diuretic medication, total cholesterol values were reduced by 4% (Weir and Moser, 2000). HDL values were increased by 10% where respondents were taking beta-blockers (Weir and Moser, 2000).
Allostatic load was constructed by first dichotomizing, separately for each sex, each of the nine biomarkers based on respondents in the highest quartile of risk (‘1’) versus the rest (‘0’). These binary measures were then summed to create the overall allostatic load score (ranging from 0 to 9) (Seeman et al., 2004; Bird et al., 2010).
2.3. Socioeconomic position
SEP was based on head of household occupational social class (Registrar General’s 1980 Social Class (RGSC) OPCS, 1980) and operationalized as the accumulated SEP over two time periods spanning 20 years. SEP was measured at baseline in 1987 and again at wave 5, with current or most recent social class data used. The six-category variable at each wave was dichotomized into manual (VI, V and III-M) and non-manual SEP (III-NM, II, I), thereby giving a possible score of 0, 1 or 2 (waves defined as being in a non-manual social class, i.e. higher SEP). The RGSC measure has been described as being “…(theoretically) a measure of prestige or social standing, (thus) it could be argued that the relation of this classification to health should be interpreted as due to the advantages bestowed by elevated social standing and increased prestige. In practice it is often interpreted as an indicator of both social standing and material reward and resources” (Galobardes et al., 2006b).
2.4. Material mediators
Data on car ownership, home ownership and income were based on self-report. Car ownership and home ownership, amongst other measures of household assets, have been hypothesized to be more direct indicators of material circumstances within the SEP construct (Davey-Smith and Egger, 1992). Both measures reflect income, but also access to resources and power (Carr-Hill et al., 1992). There may also be direct causal mechanisms between car/home ownership and health through for example, safer transport, changes in exposure to pollutants (positive and negative) or damp or overcrowded housing. It must also be noted that these measures have overlaps with behavioral, as well as psychological and psychosocial, factors, for example, owning a car resulting in decreased physical activity (behavioral), but increased pride/self-esteem (psychosocial) (Macintyre et al., 1998). Income is linked to health through multiple pathways including behavioral and psychological/psychosocial, (Benzeval et al., 2014) although the material pathway may be considered the primary driver through access to resources.
Car ownership was based on a simple yes/no question. Respondents were classed as home renters if they rented their home either from social housing stock or from a private landlord (‘1’) or were classed as homeowners (‘0’). Income was based on monthly net household income, equivalised for household size and used as a continuous measure of British Pounds (£) per week. The top and bottom 1% of values on the income distribution were excluded (trimmed) to limit the effect of outliers, a common method when measuring income inequality (Cowell and Victoria-Feser, 1996). Respondents were considered to have a low income (‘1’) if their income fell within the lowest 60% of those earning less than the median trimmed income of the cohort (a common measure of poverty in the United Kingdom).
2.5. Psychosocial and psychological mediators
Ideally, we would employ a psychosocial mediator such as stress, defined as “the interaction between people and their social environment involving psychological processes” (Egan et al., 2008), but unfortunately such variables were not available in the study. We therefore used the General Health Questionnaire (GHQ-12) to derive a psychological factor for this study. The GHQ-12 comprises 12 self-complete questions describing mood states used to assess psychiatric morbidity, with six of the questions being positively phrased and six negatively phrased (Goldberg and Williams, 1988). Each item of the GHQ-12 has four possible response options and these were scored dichotomously using the GHQ method (all items coded 0-0-1-1). Missing items were scored zero. The 12 scores were then summed and a cut-off for mental ill health derived from the mean score. For both waves 1 and 5, mean GHQ scores were approximately 2, setting a cut-off of 3 or more as a case (‘1’) compared to not being considered a case (‘0’).
2.6. Behavioral mediators
Data on smoking, alcohol consumption, diet and physical activity were based on self-report. Behavioral variables created for these analyses were based, where possible, on contemporary guidelines, as well as making variables homogeneous between waves. Smoking status at both waves 1 and 5 was defined as current (1) versus ex- or non-smoker (0). Weekly alcohol consumption was used to define respondents as below (‘0’) versus above (‘1’) gender-specific recommended weekly limits (⩽21 versus 22+ units for males; ⩽14 versus 15+ units for females) (Changing Scotland’s Relationship with Alcohol, 2009) Alcohol strength changed for some drinks during follow-up (Bromley et al., 2003) and we recalculated this variable in wave 5, although this change had no impact on our results. Physical activity was based on the number of occasions per week that respondents took part in an activity “lasting more than 20 min” that made them “sweat or (be) out of breath”, reflecting guidelines at the time. Respondents were dichotomized into high physical activity (at least 20 min once a week; ‘0’) versus low physical activity (less than once a week; ‘1’). Diet, from food-frequency questionnaires, was based on the number of days per week on which participants reported eating fruit and vegetables. Respondents were classified as having a poor diet (‘1’) if they had at least one day per week with no fruit or vegetables consumed versus not having a poor diet if they consumed fruit and vegetables every day of the week (‘0’) (See Table 1).
Table 1.
Material, psychological and behavioral mediator descriptives.⁎
| Material mediators |
Psychological mediators |
Behavioral mediators |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Number of waves classed as non-manual (higher) SEP |
Total | Number of waves classed as non-manual (higher) SEP |
Total | Number of waves classed as non-manual (higher) SEP |
|||||||||
| 0 | 1 | 2 | 0 | 1 | 2 | 0 | 1 | 2 | ||||||
| Accumulated car ownership | Accumulated GHQ-12 | Accumulated smoker | ||||||||||||
| Never | 38 (4%) | 15 (9%) | 10 (5%) | 13 (2%) | Case at both measurement waves | 73 (8%) | 32 (21%) | 12 (7%) | 27 (5%) | Both measurement waves | 206 (21%) | 82 (46%) | 50 (24%) | 72 (12%) |
| One measurement wave | 776 (79%) | 114 (65%) | 139 (67%) | 519 (87%) | Case at one measurement wave | 242 (28%) | 40 (27%) | 46 (26%) | 156 (29%) | One measurement wave | 157 (16%) | 28 (16%) | 37 (18%) | 92 (15%) |
| Both measurement waves | 172 (17%) | 46 (27%) | 59 (28%) | 65 (11%) | Never a case | 553 (64%) | 79 (52%) | 117 (67%) | 350 (66%) | Never | 206 (21%) | 67 (38%) | 122 (58%) | 433 (73%) |
| Missing | 6 | 0 | 4 | 2 | Missing | 9 | 7 | 0 | 2 | Missing | 6 | 4 | 0 | 2 |
| Accumulated home ownership | Accumulated low physical activity | |||||||||||||
| Never | 149 (15%) | 83 (47%) | 37 (18%) | 26 (4%) | Both measurement waves | 295 (31%) | 57 (35%) | 87 (34%) | 168 (29%) | |||||
| One measurement wave | 253 (26%) | 70 (40%) | 85 (41%) | 97 (16%) | One measurement wave | 406 (43%) | 79 (48%) | 86 (44%) | 237 (42%) | |||||
| Both measurement waves | 580 (59% | 22 (13%) | 86 (41%) | 470 (80%) | Never | 237 (25%) | 28 (17%) | 44 (22%) | 163 (29%) | |||||
| Missing | 6 | 3 | 1 | 2 | Missing | 9 | 2 | 4 | 3 | |||||
| Accumulated low income | Accumulated heavy drinker | |||||||||||||
| Low income for both measurement waves | 78 (9%) | 43 (29%) | 26 (15%) | 7 (1%) | Both measurement waves | 98 (10%) | 22 (12%) | 15 (7%) | 59 (10%) | |||||
| Low income at one measurement wave | 174 (21%) | 40 (27%) | 50 (28%) | 64 (13%) | One measurement wave | 262 (26%) | 30 (17%) | 46 (22%) | 185 (31%) | |||||
| Never low income | 586 (70%) | 32 (21%) | 101 (57%) | 438 (86%) | Never | 631 (64%) | 125 (71%) | 148 (71%) | 355 (59%) | |||||
| Missing | 2 | 2 | 2 | Missing | 6 | 3 | 1 | 2 | ||||||
| Accumulated poor diet | ||||||||||||||
| Both measurement waves | 411 (45%) | 99 (62%) | 88 (47%) | 219 (39%) | ||||||||||
| One measurement wave | 393 (43%) | 56 (35%) | 77 (41%) | 258 (46%) | ||||||||||
| Never | 113 (12%) | 5 (3%) | 22 (12%) | 84 (15%) | ||||||||||
| Missing | 9 | 2 | 2 | 5 | ||||||||||
Of respondents who took part in waves 1 and 5.
2.7. Cumulative mediators
For each individual measure (e.g. smoking, income, etc.), and for the combined factors, a cumulative measure was generated using data from both waves of survey data such that each mediator could take a value of 0, 1 or 2, with higher scores representing more negative material, psychological or behavioral exposures.
2.8. Statistical analyses
Although 999 respondents took part in W5 of the study, not all respondents had complete data available. The amount of missing data across all measures was 3.6% for those taking part in wave 5, although if complete-case analyses were carried out 42% of respondents would show some missing data. Multiple Imputation (MI) was therefore used to address potential biases arising from missing values. Complete-case sensitivity analysis was also carried out, but the results mirrored the substantive findings of the MI analyses (presented here). Thirty-five imputed datasets were created, and analyses were performed using the ‘ice’ and ‘mibeta’ packages in Stata (ver.11, Stata Corp., Texas, USA). Auxiliary variables (those not included in the analysis, but which help predict missingness) were included in the imputation model and included self-rated health (W1 & W5), years spent in full-time education (W5), self-assessed disability (W1), self-assessed fitness (W1) and religion (W1). All analyses were adjusted for clustered sampling at baseline and were weighted to the living baseline sample at the time of the W5 interviews using inverse probability weights to correct for bias due to drop out (Seaman and Benzeval, 2011). These weights were also included in the imputation model. Linear regression was used for the statistical analyses using a path analysis approach. First, a basic model, including sex, was used to determine the association between SEP and allostatic load, with a negative regression coefficient representing lower allostatic load being associated with higher SEP. This basic model was built on by performing further regression analyses including each individual mediator grouped by mediator type (material, psychological or behavioral) to consider the individual degree of attenuation of each potential pathway on the association. The standardized beta coefficients generated were then used to determine the direct and indirect effects between SEP and allostatic load (as seen in Figs. 2–6) Stata’s ‘mibeta’ command does not allow for the calculation of confidence intervals with standardized coefficients, therefore unstandardized coefficients are also presented, with confidence intervals and p-values in Table 2. These p-values are applicable to both standardized and unstandardized coefficients. Percentage attenuation was used as an additional inspection tool to assess the impact of each potential mediator on the SEP–allostatic load association and was calculated as:
Fig. 2.
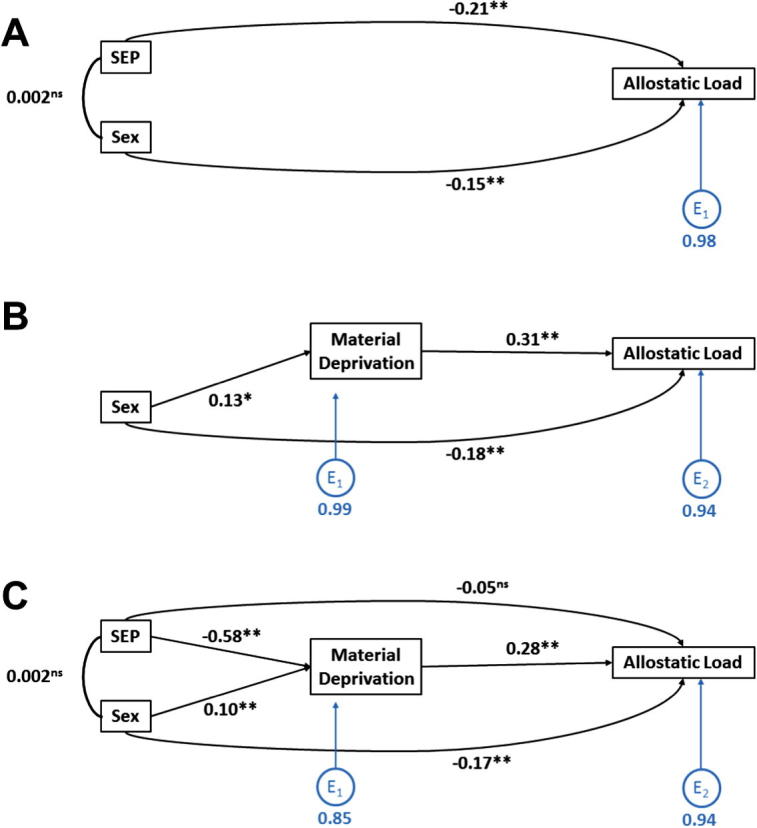
Path analysis for the association between SEP and Allostatic Load accounting for accumulated material deprivation. (A) Basic model examining the direct path between SEP and allostatic load, adjusted for sex. (B) Direct path between material deprivation (all low material possessions) and allostatic load, adjusted for sex. (C) Full path analysis of the association between SEP and allostatic load (direct path) accounting for accumulated material deprivation (indirect path) and adjusting for sex. NB all coefficients are standardized.
Fig. 3.

Path analysis for the association between SEP and Allostatic Load accounting for each of the potential Material Mediators. (A) Basic model examining the direct path between SEP and allostatic load, adjusted for sex. (B) Full path analysis of the association between SEP and allostatic load (direct path) accounting for lack of car ownership (indirect path) and adjusting for sex. (C) Full path analysis of the association between SEP and allostatic load (direct path) accounting for renting (versus owning) one’s own home (indirect path) and adjusting for sex. (D) Full path analysis of the association between SEP and allostatic load (direct path) accounting for low income (indirect path) and adjusting for sex. NB all coefficients are standardized.
Fig. 4.
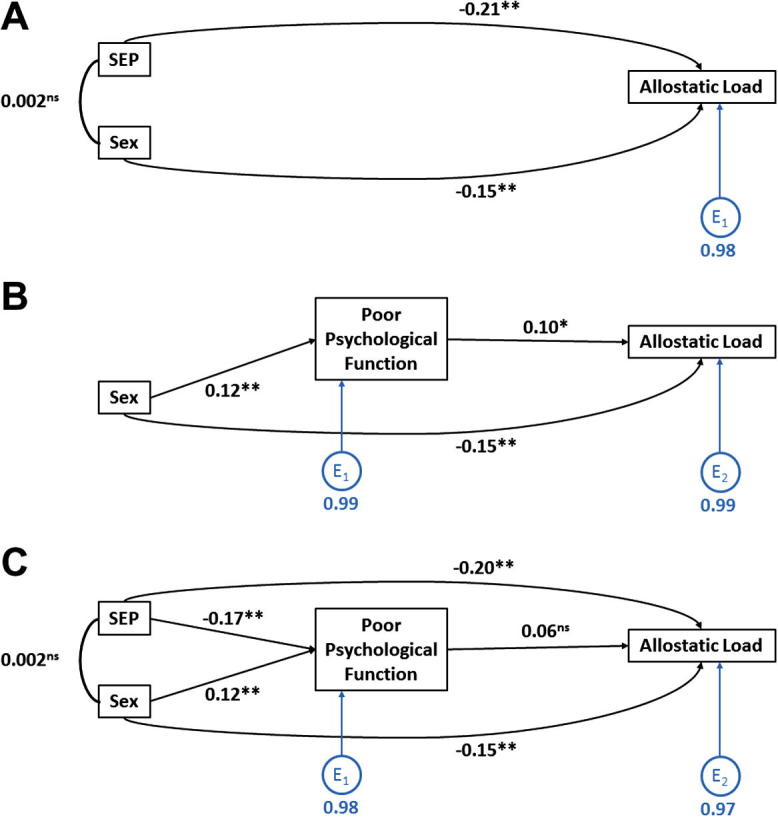
Path analysis for the association between SEP and Allostatic Load accounting for Accumulated Poor Psychological Function. (A) Basic model examining the direct path between SEP and allostatic load, adjusted for sex. (B) Direct path between accumulated poor psychological function and allostatic load, adjusted for sex. (C) Full path analysis of the association between SEP and allostatic load (direct path) accounting for poor psychological function (indirect path) and adjusting for sex. NB all coefficients are standardized.
Fig. 5.
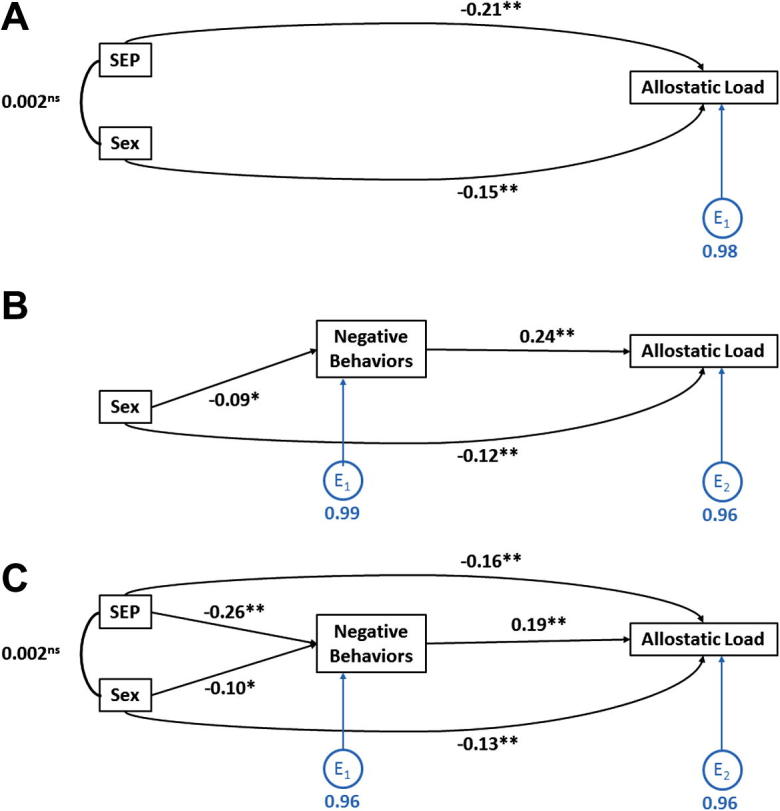
Path analysis for the association between SEP and allostatic Load accounting for Accumulated Negative Behaviors. (A) Basic model examining the direct path between SEP and allostatic load, adjusted for sex. (B) Direct path between accumulated negative behaviors and allostatic load, adjusted for sex. (C) Full path analysis of the association between SEP and allostatic load (direct path) accounting for negative behaviors (indirect path) and adjusting for sex. NB all coefficients are standardized.
Fig. 6.
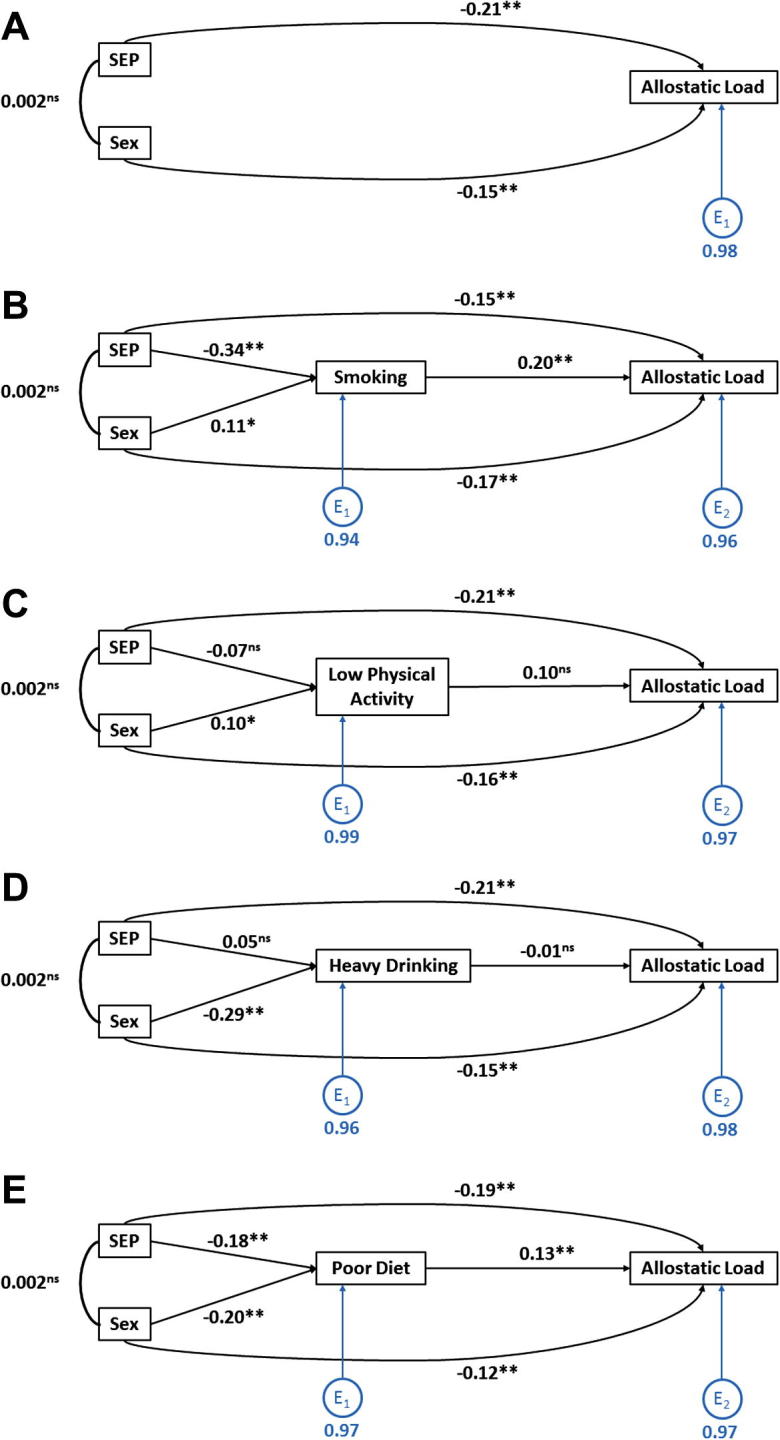
Path Analysis for the association between SEP and allostatic load accounting for each of the potential behavioral mediators. (A) Basic model examining the direct path between SEP and allostatic load, adjusted for sex. (B) Full path analysis of the association between SEP and allostatic load (direct path) accounting for smoking status (indirect path) and adjusting for sex. (C and B) Full path analysis of the association between SEP and allostatic load (direct path) accounting for low physical activity (indirect path) and adjusting for sex. (D) Full path analysis of the association between SEP and allostatic load (direct path) accounting for heavy alcohol consumption (indirect path) and adjusting for sex. (E) Full path analysis of the association between SEP and allostatic load (direct path) accounting for poor diet (indirect path) and adjusting for sex. NB all coefficients are standardized.
Table 2.
Beta coefficient (B) for the association between allostatic load and socioeconomic position, adjusted for potential mediators.
| Unstandardized B for increasing SEPa | 95% CI | P | % Reduction in Effect Size | |
|---|---|---|---|---|
| Basic modelb | −0.45 | −0.65, −0.24 | <0.001 | |
| Cumulative material mediators | ||||
| No carc | −0.44 | −0.65, −0.23 | <0.001 | 2 |
| Renting homed | −0.10 | −0.31, 0.11 | 0.352 | 78 |
| Low incomee | −0.17 | −0.36, 0.23 | 0.083 | 62 |
| All low material possessions | 0.11 | −0.31, 0.10 | 0.315 | 124 |
| Cumulative psychological mediators | ||||
| All GHQ-12 case | −0.43 | −0.63, −0.22 | <0.001 | 4 |
| Cumulative behavioral mediators | ||||
| Smokingi | −0.30 | −0.52, −0.09 | 0.007 | 33 |
| Low physical activityf | −0.43 | −0.63, −0.23 | <0.001 | 4 |
| Heavy drinkingg | −0.44 | −0.65, −0.24 | <0.001 | 2 |
| Poor dieth | −0.40 | −0.60, −0.19 | <0.001 | 11 |
| All behaviors | −0.34 | −0.55, −0.14 | 0.002 | 24 |
Negative B represents lower allostatic load with increasing SEP.
Adjusted for sex.
No car: yes vs. No.
Renting home: private/social renter vs. owner.
Low income: bottom 60% of those below median income.
Low physical activity: no vigorous activity per week (20+ mins of hot and sweaty activity).
Heavy drinking: More than 14 (women) or 21 (men) units per week.
Poor diet: At least one day per week with no fruit or vegetables consumed.
Smoking: current smoker (at least 7 cigarettes per week) vs. ex-/non-smoker.
3. Results
1444 respondents were included in the baseline sample in 1987/88, with 999 taking part in W5 (542 women). Those who remained in the sample by W5 had higher SEP, lower prevalence of health-damaging behaviors and better health than those in the baseline sample. Based on non-imputed data, mean allostatic load for men and women was 2.5 (SD = 1.6) and 2.0 (SD = 1.6), respectively. This difference was statistically significant (Fig. 2A). Eighteen percent of respondents were classed as being in the manual social class grouping across both measurement waves, with 62% classed as non-manual across both waves. Renting one’s own home and having low income were typically lower in those with lower SEP, as expected (Table 2). The pattern was more mixed for car ownership, highlighting the changing nature of car ownership since 1987. Poor psychological function showed the social patterning one might expect, with higher prevalence in those experiencing lower SEP. Smoking and poor diet showed similar social patterning, although the patterns for heavy drinking and low physical activity were more evenly spread across the socioeconomic spectrum (Table 2).
Increasing SEP was associated with lower allostatic load (unstandardized coefficient, B = −0.45; 95% CI = −0.65, −0.24, p < 0.001) (Table 2). Material deprivation fully attenuated the association between SEP and allostatic load (>100%) (Table 2). Path analysis confirmed that as well as attenuating this association, material deprivation was significantly associated with both SEP (higher SEP with greater material deprivation) and allostatic load (greater material deprivation with higher allostatic load) (Fig. 2), matching Baron and Kenny’s classical criteria for mediation (Baron and Kenny, 1986). Two of the three material mediators had a strong attenuating effect on this relationship between SEP and allostatic load so that it was no longer statistically significant at p ⩽ 0.05. Renting one’s own home had the largest impact, reducing the regression coefficient by 78% (B = −0.10; 95% CI: −0.31, 0.11; p = 0.35), while accounting for low income attenuation by 62% (B = −0.17; 95% CI: −0.36, 0.23; p = 0.08). Renting one’s own home (Fig. 3C) and low income (Fig. 3D) both met the criteria for mediation, as confirmed by path analysis. Car ownership showed no attenuation effect (Table 2), nor was it associated either with SEP or allostatic load (Fig. 3A).
GHQ-12 was used to represent psychological factors, but only minimally attenuated the association between SEP and allostatic load (by 4%, with the association remaining statistically significant: B = −0.43; 95% CI = −0.63, −0.22, p < 0.001) (Table 2). Although poor psychological function was associated with lower SEP in the path analysis, it was not associated with allostatic load (Fig. 4C).
Health-damaging behaviors attenuated the SEP–allostatic load association by only 24%, with the association remaining statistically significant (B = −0.34; 95% CI = −0.55, −0.14, p = 0.002) (Table 2). Path analysis confirmed that more negative behaviors did meet the other criteria for mediation, with higher levels being social patterned (higher prevalence with lower SEP) and being associated with higher allostatic load (Fig. 5). Of the four behavioral mediators, only smoking had any marked attenuating effect, reducing the association by 33% (B = −0.30; 95% CI = −0.52, −0.09, p = 0.007), but again the association between SEP and allostatic load remained statistically significant (Table 2). As with overall negative behaviors, smoking was significantly higher in those with lower SEP and was associated with higher allostatic load scores (Fig. 6B).
4. Discussion
This study has found evidence that negative behavioral and poorer material factors account for much of the association between higher SEP and lower allostatic load in middle-aged men and women from a community-based UK cohort. Home ownership and low income, but not car ownership, attenuated the SEP–allostatic load association by between approximately 60% and 80%. Smoking, but not alcohol consumption, poor diet or low physical activity, attenuated the SEP–allostatic load association by a third. Adjustment for GHQ-12, a measure of psychological circumstances, had next to no attenuating effect.
There is growing evidence for a link between higher SEP and lower allostatic load, which is supported here. However, consistent evidence linking material, psychosocial and/or psychological and behavioral factors as mediators of the association is still lacking. In a study of over 800 US men aged 21–80, Kubzansky et al. (1999) found that higher levels of perceived hostility attenuated the association between lower education and higher allostatic load (Kubzansky et al., 1999). Hawkley et al. (2011) also found that hostility (and poor sleep) attenuated the association between SEP and allostatic load in approximately 200 US men and women aged 51–69 (Hawkley et al., 2011). However, a range of other psychological and behavioral measures (smoking, alcohol consumption, physical activity and diet) had no impact. Similarly, Schulz et al. (2012) found that measures of stress and negative life events helped explain the (neighborhood-level) social gradient in allostatic load in nearly 1000 US middle-aged men and women, whereas health behaviors did not. Finally, Gruenewald et al. (2012) found that smoking, alcohol consumption, fast food consumption and reduced contact with friends helped explain approximately 35–40% of the SEP–allostatic load association in 1000 US men and women, aged 35–85 (Gruenewald et al., 2012). However, life events, stress and coping-skills had only a minimal effect.
Material factors have been largely ignored as possible mediators between SEP and allostatic load in previous literature. However, recent work by Gustafsson et al. (2014) has explored the links between neighborhood SEP and allostatic load, including the contribution of personal material disadvantage (using a summative score of 14 different material measures) Gustafsson et al. (2014) found that material disadvantage only slightly attenuated the association between lower neighborhood SEP and higher allostatic load, with the SEP–allostatic load association still remaining statistically significant after adjustment. Our analysis has shown a more significant role for material disadvantage in explaining the link between individual SEP and allostatic load, with factors such as renting one’s own home and having low income strongly attenuating the association between SEP and allostatic load. Occupation-based measures of SEP (e.g. working age social class used here) are strongly tied to income and material goods/opportunities, as measured by car ownership, home ownership and income status (Galobardes et al., 2006a), hence the stronger attenuating effect. The material and psychosocial/psychological pathways that help explain socioeconomic inequalities in allostatic load and health are not mutually exclusive and may be difficult to separate (Bartley, 2003). These material factors may be related to increased exposure to harmful conditions in the workplace, home and neighborhood (toxins, carcinogens, crime, injury, etc.), but also increased prevalence of negative psychosocial factors (e.g. stressors, lack of coping skills, etc.) (Adler and Ostrove, 1999) and consequent psychological distress. Therefore, it is difficult to be certain that there is no psychosocial or psychological mediation between lower SEP and higher allostatic load. Our results provide evidence that interventions targeted further upstream to health outcomes, especially material deprivation, could be important if we are to try and reduce inequalities in allostatic load and possibly health.
In terms of behavioral pathways, only smoking had any marked attenuating effect. Smoking has been linked with detrimental effects (direct and indirect) on many of the individual components of the allostatic load construct (Omvik, 1996; Moffatt, 1988; Tonstad and Cowan, 2009; Will et al., 2001) and has been extensively linked with lower SEP (Hiscock et al., 2012). If smoking prevalence can be significantly reduced in Scotland (and other countries) it could wield significant power in reducing inequalities in allostatic load and health. However, it must be noted that there may be long-lasting impacts of negative behaviors (as well as material circumstances) on allostatic load not captured here.
We have found little evidence to support psychological factors, as measured with GHQ, mediating the SEP–allostatic load association. This may be the result of GHQ being a measure of mental health and less effective at capturing broader psychosocial factors such as stress, one of the major pathways hypothesized to link SEP and allostatic load. No alternative direct measures of stress were consistently available in this study.
This is the first study to focus on the three possible pathways that may link SEP and allostatic load, utilizing a relatively large general population sample of men and women. In addition, we have used a measure of SEP and mediators accumulated over time, most likely to show the strongest relationship with long-term cumulative physiological damage, as measured by allostatic load. We have further strengthened this study by using multiple imputation to address issues of potential bias through item missingness and probability weights to minimize the effects of bias through attrition.
The measures selected to encapsulate the three theoretical pathways may not be all encompassing, but we have selected a relatively large number and broad-range of measures, essential in better understanding and considering the complex interactions and effects of these mediators when considering interventions.
One potential limitation is only using respondents at one age. This lack of a continuous age range limits the conclusions that can be made about the ages not sampled here, although it gives a good indication of the association at middle age. Our allostatic load construct did not contain any markers from the hypothalamic pituitary adrenal (HPA) axis that forms part of the neuroendocrine system (stress response). The stress response is believed to play a key role in allostasis and subsequent allostatic load, with a cascade of events that starts with primary stress mediators, such as cortisol, before initial stress responses (‘primary effects’ such as rapid increases in blood pressure, and sugars and fats that supply the body with extra energy) and then to secondary and tertiary outcomes (measured in our allostatic load model). These stress markers are difficult to measure in large surveys where direct examination of the stress response (e.g. measuring cortisol) is problematic due to the circadian rhythms shown in these stress hormones and the rapid sampling required in order to measure baseline versus activated levels. Inclusion of measures such as cortisol could improve the power of allostatic load as an earlier risk predictor for disease, but their exclusion does not invalidate this allostatic load construct as the subsequent outcomes of cortisol release are still included. It is also important to consider limitations in the measurement and meaning of the mediators. The data for all the mediators is self-report. This can lead to under- or over-estimates of some health behaviors such as alcohol or physical activity (Boniface and Shelton, 2013; Prince et al., 2008). The measures selected for this analysis were based on a priori knowledge of their relevance for their specific mediator groupings, but availability (and lack thereof) also influences which individual components can be included in the analysis. In terms of SEP, we used occupational-based social class as it is a well-validated measure of SEP in the UK, as well as being measured consistently over time and rarely affected by non-response. Finally, we dichotomized our SEP measure to manual/non-manual categories to ease construction of a long-term SEP measure. While dichotomizing the RGSC measure is a common and validated procedure, the meaning of social class (and the binary distinction) has become less relevant over time in the UK (with the increase in non-manual service sector jobs such as call centers, for example).
In summary, we have found evidence that material conditions, as well as smoking, are important mediators in the pathway between lower SEP and higher allostatic load. This is an important step in better understanding the pathways and mechanisms linking SEP, physiology and health.
Conflict of interest
All authors declare that there are no conflicts of interest.
References
- Adler N.E., Ostrove J.M. Socioeconomic status and health: what we know and what we don’t. Ann. N. Y. Acad. Sci. 1999;896(1):3–15. doi: 10.1111/j.1749-6632.1999.tb08101.x. [DOI] [PubMed] [Google Scholar]
- Adler N.E., Stewart J. Health disparities across the lifespan: meaning, methods, and mechanisms. Ann. N. Y. Acad. Sci. 2010;1186(1):5–23. doi: 10.1111/j.1749-6632.2009.05337.x. [DOI] [PubMed] [Google Scholar]
- Baron R.M., Kenny D.A. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bartley M. Polity Press; Cambridge, UK: 2003. Health Inequality: An Introduction to Theories, Concepts and Methods. [Google Scholar]
- Baum A., Garofalo J.P., Yali A.M. Socioeconomic status and chronic stress: does stress account for SES effects on health? Ann. N. Y. Acad. Sci. 1999;896(1):131–144. doi: 10.1111/j.1749-6632.1999.tb08111.x. [DOI] [PubMed] [Google Scholar]
- Benzeval M., Der G., Ellaway A., Hunt K., Sweeting H., West P., Macintyre S. Cohort profile: west of Scotland twenty-07 study: health in the community. Int. J. Epidemiol. 2009;38(5):1215–1223. doi: 10.1093/ije/dyn213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benzeval M., Bond L., Campbell M., Egan M., Lorenc T., Petticrew M., Popham F. Joseph Roundtree Foundation; York, UK: 2014. How does Money Influence Health? [Google Scholar]
- Bird C.E., Seeman T., Escarce J.J., Basurto-Davila R., Finch B.K., Dubowitz T., Heron M., Hale L., Merkin S.S., Weden M. Neighbourhood socioeconomic status and biological ‘wear and tear’ in a nationally representative sample of US adults. J. Epidemiol. Community Health. 2010;64(10):860–865. doi: 10.1136/jech.2008.084814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boniface S., Shelton N. How is alcohol consumption affected if we account for under-reporting? a hypothetical scenario. Eur. J. Public Health. 2013;23(6):1076–1081. doi: 10.1093/eurpub/ckt016. [DOI] [PubMed] [Google Scholar]
- Bromley, C., Corbett, J., Erens, B., Moody A., 2003. Scottish Health Survey: Revised Alcohol Consumption Estimates. In: Edinburgh, UK: Scottish Government.
- Brunner E. Socioeconomic determinants of health: stress and the biology of inequality. BMJ. 1997;314:1472. doi: 10.1136/bmj.314.7092.1472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr-Hill R., Sheldon T., Thunhurst C. The politics of deprivation indices and health. In: S N., Warwick H.J., editors. Uses and Abuses of Deprivation Indices. University of Warwick; UK: 1992. [Google Scholar]
- Changing Scotland’s Relationship with Alcohol: A Framework for Action. In: Government S. Edinburgh (Ed.), UK: Scottish Government; 2009.
- Cohen S., Doyle W.J., Baum A. Socioeconomic status is associated with stress hormones. Psychosom. Med. 2006;68(3):414–420. doi: 10.1097/01.psy.0000221236.37158.b9. [DOI] [PubMed] [Google Scholar]
- Cowell F.A., Victoria-Feser M.P. Robustness properties of inequality measures. Econometrica. 1996;64(1):77–101. [Google Scholar]
- Davey-Smith G., Egger M. Socioeconomic differences in mortality in Britain and the United States. Am. J. Public Health. 1992;82(8):1079–1081. doi: 10.2105/ajph.82.8.1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Egan M., Tannahill C., Petticrew M., Thomas S. Psychosocial risk factors in home and community settings and their associations with population health and health inequalities: a systematic meta-review. BMC Public Health. 2008;8:239. doi: 10.1186/1471-2458-8-239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galobardes B., Shaw M., Lawlor D.A., Lynch J.W., Davey Smith G. Indicators of socioeconomic position (part 1) J. Epidemiol. Community Health. 2006;60:7–12. doi: 10.1136/jech.2004.023531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galobardes B., Shaw M., Lawlor D.A., Lynch J.W., Davey Smith G. Indicators of socioeconomic position (part 2) J. Epidemiol. Community Health. 2006;60 doi: 10.1136/jech.2004.028092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg D., Williams P. NFER-Neson; Windsor, UK: 1988. A User’s Guide to the General Health Questionnaire. [Google Scholar]
- Gruenewald T.L., Seeman T.E., Karlamangla A.S., Sarkisian C.A. Allostatic load and frailty in older adults. J. Am. Geriatr. Soc. 2009;57(9):1525–1531. doi: 10.1111/j.1532-5415.2009.02389.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gruenewald T.L., Karlamangla A.S., Hu P., Stein-Merkin S., Crandall C., Koretz B., Seeman T.E. History of socioeconomic disadvantage and allostatic load in later life. Soc. Sci. Med. 2012;74(1):75–83. doi: 10.1016/j.socscimed.2011.09.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gustafsson P.E., San Sebastian M., Janlert U., Theorell T., Westerlund H., Hammarstrom A. Life-course accumulation of neighborhood disadvantage and allostatic load: empirical integration of three social determinants of health frameworks. Am. J. Public Health. 2014;104(5):904–910. doi: 10.2105/AJPH.2013.301707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gustafsson P.E., Janlert U., Theorell T., Westerlund H., Hammarstrom A. Socioeconomic status over the life course and allostatic load in adulthood: results from the Northern Swedish Cohort. J. Epidemiol. Community Health. 2011;65(11):986–992. doi: 10.1136/jech.2010.108332. [DOI] [PubMed] [Google Scholar]
- Gustafsson P.E., Janlert U., Theorell T., Westerlund H., Hammarstrom A. Social and material adversity from adolescence to adulthood and allostatic load in middle-aged women and men: results from the Northern Swedish Cohort. Ann. Behav. Med. 2012;43(1):117–128. doi: 10.1007/s12160-011-9309-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkley L.C., Lavelle L.A., Berntson G.G., Cacioppo J.T. Mediators of the relationship between socioeconomic status and allostatic load in the Chicago Health, Aging, and Social Relations Study (CHASRS) Psychophysiology. 2011;48(8):1134–1145. doi: 10.1111/j.1469-8986.2011.01185.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hiscock R., Bauld L., Amos A., Fidler J.A., Munafo M. Socioeconomic status and smoking: a review. Ann. N. Y. Acad. Sci. 2012;1248:107–123. doi: 10.1111/j.1749-6632.2011.06202.x. [DOI] [PubMed] [Google Scholar]
- Karlamangla A.S., Singer B.H., Seeman T.E. Reduction in allostatic load in older adults is associated with lower all-cause mortality risk: MacArthur studies of successful aging. Psychosom. Med. 2006;68(3):500–507. doi: 10.1097/01.psy.0000221270.93985.82. [DOI] [PubMed] [Google Scholar]
- Kinshuck, D., Lamb, P., Griffiths, U., 2013. Control of Type 2 diabetes. <http://www.diabeticretinopathy.org.uk/HBA1c%20&%20type%202%20diabetes.htm/> (accessed 14.08.13).
- Kubzansky L.D., Kawachi I., Sparrow D. Socioeconomic status, hostility, and risk factor clustering in the Normative Aging Study: any help from the concept of allostatic load? Ann. Behav. Med. 1999;21(4):330–338. doi: 10.1007/BF02895966. [DOI] [PubMed] [Google Scholar]
- Law M.R., Wald N.J., Morris J.K., Jordan R.E. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427. doi: 10.1136/bmj.326.7404.1427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Law M.R., Wald N.J., Rudnicka A.R. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ. 2003;326(7404):1423. doi: 10.1136/bmj.326.7404.1423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macintyre S., Ellaway A., Der G., Ford G., Hunt K. Do housing tenure and car access predict health because they are simply markers of income or self esteem? a Scottish study. J. Epidemiol. Community Health. 1998;52(10):657–664. doi: 10.1136/jech.52.10.657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen B.S. From molecules to mind. Stress, individual differences, and the social environment. Ann. N. Y. Acad. Sci. 2001;935:42–49. [PubMed] [Google Scholar]
- McEwen B.S. Protective and damaging effects of stress mediators: central role of the brain. Dialogues Clin. Neurosci. 2006;8(4):367–381. doi: 10.31887/DCNS.2006.8.4/bmcewen. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moffatt R.J. Effects of cessation of smoking on serum lipids and high density lipoprotein-cholesterol. Atherosclerosis. 1988;74(1–2):85–89. doi: 10.1016/0021-9150(88)90194-3. [DOI] [PubMed] [Google Scholar]
- Omvik P. How smoking affects blood pressure. Blood Press. 1996;5(2):71–77. doi: 10.3109/08037059609062111. [DOI] [PubMed] [Google Scholar]
- Opcs A. HMSO; London: 1980. Classification of Occupations. [Google Scholar]
- Prince S., Adamo K., Hamel M., Hardt J., Gorber S., Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int. J. Behav. Nutr. Phys. Act. 2008;5(1):56. doi: 10.1186/1479-5868-5-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robertson T., Popham F., Benzeval M. Socioeconomic position across the lifecourse & allostatic load: data from the West of Scotland Twenty-07 cohort study. BMC Public Health. 2014;14(1):184. doi: 10.1186/1471-2458-14-184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabbah W., Watt R.G., Sheiham A., Tsakos G. Effects of allostatic load on the social gradient in ischaemic heart disease and periodontal disease: evidence from the Third National Health and Nutrition Examination Survey. J. Epidemiol. Community Health. 2008;62(5):415–420. doi: 10.1136/jech.2007.064188. [DOI] [PubMed] [Google Scholar]
- Schulz A.J., Mentz G., Lachance L., Johnson J., Gaines C., Israel B.A. Associations between socioeconomic status and allostatic load: effects of neighborhood poverty and tests of mediating pathways. Am. J. Public Health. 2012;102(9):1706–1714. doi: 10.2105/AJPH.2011.300412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seaman, S., Benzeval, M., 2011. The West of Scotland Twenty-07 Study: Inverse probability weights for Wave 5: MRC/CSO Social and Public Health Sciences Unit Working Paper 27, Glasgow.
- Seeman T.E., Singer B.H., Rowe J.W., Horwitz R.I., McEwen B.S. Price of adaptation–allostatic load and its health consequences. MacArthur studies of successful aging. Arch. Intern. Med. 1997;157(19):2259–2268. [PubMed] [Google Scholar]
- Seeman T.E., Crimmins E., Huang M.H., Singer B., Bucur A., Gruenewald T., Berkman L.F., Reuben D.B. Cumulative biological risk and socio-economic differences in mortality: MacArthur studies of successful aging. Soc. Sci. Med. 2004;58(10):1985–1997. doi: 10.1016/S0277-9536(03)00402-7. [DOI] [PubMed] [Google Scholar]
- Seeman T., Merkin S.S., Crimmins E., Koretz B., Charette S., Karlamangla A. Education, income and ethnic differences in cumulative biological risk profiles in a national sample of US adults: NHANES III (1988–1994) Soc. Sci. Med. 2008;66(1):72–87. doi: 10.1016/j.socscimed.2007.08.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sterling P., Eyer J. Allostasis: a new paradigm to explain arousal pathology. In: Fisher S., Reason J., editors. Handbook of Life Stress, Cognition, and Health. Wiley; New York: 1988. pp. 629–649. [Google Scholar]
- Stewart J.A. The detrimental effects of allostasis: allostatic load as a measure of cumulative stress. J. Physiol. Anthropol. 2006;25(1):133–145. doi: 10.2114/jpa2.25.133. [DOI] [PubMed] [Google Scholar]
- Tonstad S., Cowan J.L. C-reactive protein as a predictor of disease in smokers and former smokers: a review. Int. J. Clin. Pract. 2009;63(11):1634–1641. doi: 10.1111/j.1742-1241.2009.02179.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weir M.R., Moser M. Diuretics and beta-blockers: is there a risk for dyslipidemia? Am. Heart J. 2000;139(1):174–183. doi: 10.1016/s0002-8703(00)90325-9. [DOI] [PubMed] [Google Scholar]
- Will J.C., Galuska D.A., Ford E.S., Mokdad A., Calle E.E. Cigarette smoking and diabetes mellitus: evidence of a positive association from a large prospective cohort study. Int. J. Epidemiol. 2001;30(3):540–546. doi: 10.1093/ije/30.3.540. [DOI] [PubMed] [Google Scholar]