

Abstract
Although a number of studies have linked body dissatisfaction to depressive symptoms, few have done so within the framework of a vulnerability-stress model. We hypothesized that women’s levels of body dissatisfaction would interact with recent experiences of vulnerability-congruent negative life events (i.e., weight-related teasing) to predict prospective changes in depressive symptoms. Consistent with these hypotheses, experiences of weight-related teasing were more strongly related to depressive symptom increases among women with high, compared to low, levels of body dissatisfaction. These results support the hypothesis that body dissatisfaction moderates the impact of weight-related teasing on depressive symptom changes.
Keywords: weight-related teasing, body dissatisfaction, depression
1.1 Introduction
A growing body of research has suggested that body dissatisfaction may contribute risk for depression (e.g., Allgood-Merten, Lewinsohn, & Hops, 1990; Fabian & Thompson, 1989; Laessle, Kittl, Fichter, & Pirke, 1988; Rierdan, Koff, & Stubbs, 1989; Stice, Killen, Hayward & Taylor, 1998; Thompson, Coovert, Richards, Johnson, & Cattarin, 1995). Beginning in adolescence, rates of depression are approximately twice as high for women than for men (Hankin, Abramson, Moffit, Silva, McGee, & Angell, 1998), and research suggests that body dissatisfaction contributes to elevated depression levels above and beyond other risk factors, such as body mass (Stice & Bearman, 2001). The 30-day prevalence of depression among 15 to 24 year old women is 8% and the lifetime prevalence is 20.8% (Blazer, Kessler, McGonagle, & Swartz, 1994). Given this, young-adult women may be an especially important group upon which to focus when examining risk for depression.
Starting as early as adolescence, girls have significantly higher levels of body dissatisfaction than do boys (Barker & Galambos, 2003; McCabe & Ricciardelli, 2001). Further, girls who are depressed also have significantly higher levels of body dissatisfaction than boys who are depressed (Bennett, Ambrosini, Kudes, Metz, & Rabinovich, 2005). It has been suggested that the gender differences in depression that first emerge during adolescence are in part a function of the developmental transition that occurs mid-puberty (Angold, 1998), as well as increased developmental challenges for girls, such as dissatisfaction with weight (Wichstrøm, 1999). The discrepancy between real and ideal physical appearance is more marked for females than males, and this increased discrepancy may contribute to depressed mood (Higgins, 1987; Straumann, Vookles, Berenstein, Chaiken, & Higgins, 1991; Wichstrøm, 1999). Further, gender differences in depressed mood are substantially reduced when the difference in body dissatisfaction is accounted for (for a review, see Wichstrøm, 1999).
Among college students, women have higher levels of body dissatisfaction, disordered eating habits, and dieting behaviors than men, despite having similar body mass indices (Edman, Yates, Aruguete, & DeBord, 2005). One study found that undergraduate women had higher levels of body dissatisfaction than undergraduate men even when matched on levels of body focus, or the tendency to focus on aspects of the body that are most often associated with reasons for dieting or social acceptance (Lokken, Ferraro, Kirchner, & Bowling, 2003). As such, this may be evidence for why women are at significantly increased risk for depression and eating disorders (Hankin et al., 1998; Hudson et al., 2007; Nolen-Hoeksema & Girgus, 1994).
Despite the established link between body dissatisfaction and depression (e.g., Johnson, & Wardle, 2005; Paxton, Eisenberg, & Neumark-Sztainer, 2006; Paxton, Neumark-Sztainer, Hannan, & Eisenberg, 2006), the potential risk conveyed by body dissatisfaction is rarely considered within the context of environmental stressors that the individual may also be experiencing. Indeed, most cognitive theories of depression present vulnerability-stress models of risk in which certain cognitions are hypothesized to increase risk for depression in the presence, but not absence, of negative life events (e.g., Abramson, Metalsky, & Alloy, 1989; Clark, Beck, & Alford, 1999). Further, according to Beck’s event-congruency hypothesis (Beck, 1983, 1987; Clark et al., 1999), depressive reactions should be more likely when there is a match between the specific type of event experienced and the vulnerability exhibited. Building upon Beck’s theory, cognitive-interpersonal models of depression (e.g., Hammen, 1992) have emphasized the interaction between specific types of negative cognitive styles and individuals’ interpersonal relations in contributing vulnerability to depression. Specifically, negative interpersonal events are hypothesized to activate pre-existing negative schema, which then contribute to depression. Further, it has been suggested that the gender differences seen in depression are, in part, a function of the increasing influence of negative interpersonal life events on emotional maladjustment throughout adolescence (Hankin, Mermelstein, & Roesch, 2007). Not only are females more likely to experience negative interpersonal events than males, but females are also more likely than males to become depressed following these events (Hankin et al., 2007). This said, however, relatively little is known about which specific types of negative interpersonal events may increase risk for depression.
One type of negative interpersonal event that may be particularly salient to individuals with high levels of body dissatisfaction is teasing about one’s weight. Research has suggested that perceptions of body dissatisfaction are heavily influenced by social events such as peer, parent, and media influences (Keery, van den Berg, & Thompson, 2004; Schutz, & Paxton, 2007; van den Berg, Thompson, Obremski-Brandon& Coovert, 2002) and that peer influences among college women affect dysfunctional eating behaviors (van den Berg et al., 2002). Consistent with Beck’s (1983, 1987; Clark et al., 1999) cognitive vulnerability-event congruency hypothesis, one would predict that weight-related teasing, which includes messages directly targeted toward a person’s body weight and shape, may be more likely than other types of events to “activate” pre-existing thoughts of body dissatisfaction.
The primary goal of the current study was to prospectively examine a specific vulnerability-stress model of depression in women. Building from Beck’s cognitive vulnerability-event congruency hypothesis, we hypothesized that women’s levels of body dissatisfaction would moderate the link between weight-related teasing and depressive symptoms. Specifically, we predicted that experiences of weight-related teasing would be more likely to predict depressive symptom increases among women with high, compared to low, levels of body dissatisfaction, and that this relation would persist irrespective of actual weight status. Further, we predicted that this moderation would not exist when examining the link between other types of teasing (e.g., general appearance teasing) and depressive symptoms, thus providing a stronger test of Beck’s cognitive vulnerability-event congruency hypothesis.
2.1 Material and Methods
2.1.1 Participants
Participants in this study were 116 undergraduate women recruited from their introductory psychology classes who participated in exchange for receiving course credit. The mean age was 18.64 years (SD = 0.97). The racial/ethnic background of the participants was as follows: 53% Caucasian, 15% African American, 15% Asian, 9% Hispanic, and 8% other. Of the Time 1 participants, 73.3% (n = 85) completed the follow-up assessment. There were no significant differences between completers and attritors on any of the Time 1 variables.
Based on self-reported height and weight, the mean body mass index (as measured by weight in kilograms divided by height in meters squared) was 23.19 (SD = 3.39). Therefore, on average, participants in our sample fell within the normal range of body mass.
2.1.2 Measures
Body Dissatisfaction
The Body Shape Questionnaire (BSQ; Cooper, Taylor, Cooper & Fairburn, 1987) is a 34-item self-report questionnaire used to assess concerns about weight and body shape, specifically how the individual has been feeling about her/his appearance over the past four weeks (e.g., “Have you felt ashamed of your body?”, “Have you felt so bad about your shape that you have cried?”). Responses are on a 6-point Likert scale ranging from “never” to “always” with higher total scores indicating more body dissatisfaction. The BSQ has demonstrated high retest reliability and strong concurrent validity with measures of self-evaluation and body checking (Rosen, Jones, Ramirez, & Waxman, 1995). The BSQ demonstrated excellent internal consistency in the current study (α = .98).
Weight-related Teasing
The Physical Appearance Related Teasing Scale (PARTS; Thompson, Fabian, Moulton, Dunn, & Altabe, 1991) is an 18-item scale used to assess appearance related teasing and is composed of two factors: general appearance teasing (GAT) and weight/size teasing (W/ST). Subjects respond on a 5-point Likert-type scale, with responses ranging from “never” to “frequently.” Items on the W/ST subscale focus on experiences of teasing in relation to weight and size, such as, “Did others call you derogatory names that related to your size or weight?” and “Did you ever feel like people were pointing at you because of your size or weight?” Items on the GAT subscale focus on experiences of teasing in relation to general appearance, such as, “Did people say you had funny teeth?” and “Did other kids ever make jokes about your hair?” For the current study, the PARTS subscales were modified to assess current teasing that occurred during the follow-up interval. Previous studies have suggested that the subscales exhibit good internal consistency and retest reliability (e.g., Thompson et al., 1991). In this study, the modified W/ST and GAT subscales exhibited excellent internal consistency (αs = .96 and .96, respectively).
Depressive symptoms
The Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996) is a 21-item self-report measure that was used to assess the severity of depressive symptoms in the subjects. The BDI-II exhibits good reliability and validity (Beck et al., 1996) and had good internal consistency in this study at both the first and second assessments (αs = .92 and .95, respectively).
2.1.3 Procedure
Participants completed the questionnaires in large groups. At the initial assessment, participants completed the Body Shape Questionnaire and the Beck Depression Inventory-II. At the second assessment, which occurred approximately one month later, participants completed the Physical Appearance Related Teasing Scale (modified as described above to assess experiences of teasing between the two assessment points) and the Beck Depression Inventory-II.
3.1 Results
Preliminary analyses were conducted to determine if there was significant skew among any of the variables. Variables that exhibited skew were transformed (e.g., square root, log 10, inverse) to satisfy assumptions of normality prior to any further analysis. Due to the low levels of reported experiences of current weight-related teasing (i.e., 68% denied any experiences of weight-related teasing during the follow-up), scores on the PARTS W/ST were dichotomized to indicate presence versus absence of teasing during the follow-up. This was also done for the GAT subscale (i.e., 91% denied any experiences of current general appearance teasing). In addition, given the presence of missing data (T1 BSQ = 2%; T1 BDI-II = 0%; T2 BDI-II = 27%; T2 W/ST = 34%), the pattern of missingness was examined to determine if the use of data imputation methods for estimating missing values was warranted (cf. Shafer & Graham, 2002). Maximum likelihood estimation of missing values is preferable over listwise deletion of missing cases because it provides more accurate parameter estimates (Shafer & Graham, 2002). Thus, as a first step, a series of t-tests was conducted to determine if attriting individuals differed from nonattriting individuals on any of the study variables. As noted above, none of these analyses was significant. Next, we examined Little’s Missing Completely at Random test (MCAR; Little & Rubin, 1987), for which the null hypothesis is that the data are missing at random. This, too, was nonsignificant, χ2 (17) = 16.52, p = .49, supporting the estimation of missing values. Therefore, maximum likelihood estimates of missing data were created and used in all subsequent analyses (see Shafer & Graham, 2002). We note, however, that results were virtually identical even when the sample was limited to participants with complete data, and the pattern of significant effects was identical to that reported below. Correlations among the study variables, as well as their means and standard deviations, are presented in Table 1. To facilitate comparison with other studies, the means and standard deviations presented are based on the untransformed variables.
Table 1.
Correlations and Descriptive Statistics for Study Variables
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| 1. BSQ | - | ||||
| 2. PARTS W/ST | .59** | - | |||
| 3. T1 BDI-II | .51** | .40** | - | ||
| 4. T2 BDI-II | .44** | .43** | .82** | - | |
| 5. BMI | .47** | .25** | .24* | .16 | - |
|
| |||||
| Mean | 87.14 | 13.87 | 9.12 | 7.07 | 23.19 |
| SD | 38.07 | 4.57 | 8.50 | 9.14 | 3.39 |
Note. BSQ = Body Shape Questionnaire; PARTS: W/ST = Physical Appearance Related Teasing Scale: Weight/Size Teasing Subscale; T1 BDI-II = Beck Depression Inventory- II at Time 1; T2 BDI-II = Beck Depression Inventory- II at Time 2. BMI = Body Mass Index.
p < .05.
p < .01.
Next, a hierarchical multiple regression analysis was used to test the hypothesis that women’s levels of body dissatisfaction would moderate the link between experiences of weight-related teasing and prospective changes in depressive symptoms (see Table 2). Using Time 2 depressive symptoms as the criterion variable, Time 1 depressive symptoms were entered in the first step of the regression, which allowed us to examine residual change in depressive symptoms across the follow-up. In this first step, Time 1 depressive symptoms were significantly related to Time 2 depressive symptoms, t(114) = 15.21, p < .001, β = .82. Body dissatisfaction and weight-related teasing were entered in the second step of the hierarchical regression, and only weight-related teasing was significant, t(112) = 2.11, p = .04, β = .14. In the third step of the regression, we entered the body dissatisfaction × weight-related teasing interaction, and it was significant, t(111) = 3.73, p < .001, β = 1.28. Following Aiken and West (1991), we examined the simple slopes of weight-related teasing on depressive symptom change among women with high (+1 SD) versus low (−1 SD) levels of body dissatisfaction. Consistent with our hypothesis, experiences of weight-related teasing were associated with residual increases in depressive symptoms among women with high, t(111) = 3.70, p < .001, β = .26, but not low, t(111) = −1.86, p = .07, β = −.21, levels of body dissatisfaction (see Figure 1).1
Table 2.
Summary of Prospective Analyses
| Variable | B | SE B | β | pr | R Square | R Square Change |
|---|---|---|---|---|---|---|
| Step 1 | ||||||
| BDI-II | .24 | .02 | .82*** | .82 | .67 | .67 |
| Step 2 | ||||||
| BSQ | −.01 | .01 | −.04 | −.05 | .68 | .01 |
| W/ST | .14 | .07 | .14* | .20 | ||
| Step 3 | ||||||
| BSQ × W/ST | .12 | .03 | 1.28*** | .33 | .72 | .04 |
Note. BSQ = Body Shape Questionnaire; W/ST = Physical Appearance Related Teasing Scale: Weight/Size Teasing Subscale; BDI-II = Beck Depression Inventory- II at Time 1.
p < .05.
p < .001.
Figure 1.
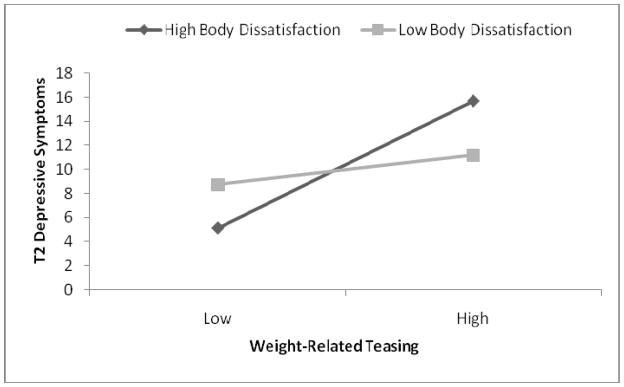
Interaction of weight-related teasing and body dissatisfaction to predict Time 2 depressive symptom levels.
To evaluate the robustness of this effect, we examined whether it would be maintained even after statistically controlling for the influence of participants’ BMI. Specifically, we reconducted the regression analysis, adding BMI score as a covariate. In this analysis, the body dissatisfaction × weight-related teasing interaction remained significant, t(110) = 3.70, p < .001, β = 1.28, and experiences of weight-related teasing continued to predict residual change in depressive symptoms among women with high (+1 SD) levels of body dissatisfaction, t(110) = 3.67, p < .001, β = .26. We should also note that women’s BMI did not significantly moderate the relation between weight-related teasing and change in depressive symptoms, t(111) = 0.87, p = .38, β = 0.71.
Finally, to provide a stronger test of Beck’s cognitive vulnerability-event congruency hypothesis, we examined whether body dissatisfaction would also moderate the link between general appearance teasing and depressive symptom changes. As before, a hierarchical multiple regression analysis was used with Time 2 depressive symptoms as the criterion variable and Time 1 depressive symptoms were entered in the first step of the regression. As before, Time 1 depressive symptoms were significantly related to Time 2 depressive symptoms, t(114) = 15.21, p < .001, β = .82, in this first step. Body dissatisfaction and general appearance teasing were then entered in the second step of the hierarchical regression, and neither was significant (ps = .57 and .71, respectively). In the third step of the regression, we entered the body dissatisfaction × general appearance teasing interaction, and it was also nonsignificant, t(114) = 1.60, p = .11, β = .48.
4.1 Discussion
The primary goal of this study was to provide a prospective test of a cognitive vulnerability-stress model of depression in young women. Specifically, we tested the hypothesis that higher levels of body dissatisfaction would contribute to prospective depressive symptom changes in the presence, but not absence, of a vulnerability-congruent stressor – weight-related teasing. As hypothesized, we found that levels of body dissatisfaction moderated the link between weight-related teasing and depressive symptom increases in women. Specifically, higher levels of body dissatisfaction were positively related to residual increases in depressive symptoms among women experiencing weight-related teasing during the follow-up. This relationship was maintained after statistically controlling for BMI, suggesting that the results were not due simply to the effects of women’s body mass. Supporting Beck’s (Beck, 1983, 1987; Clark et al., 1999) cognitive vulnerability-event congruency hypothesis, body dissatisfaction did not moderate the effects of a different form of teasing – general appearance teasing – on prospective depressive symptom changes.
Despite the established link between body dissatisfaction and depression, the potential risk conveyed by body dissatisfaction is rarely considered within the context of environmental stressors that the individual may also be experiencing. Although the results obtained in this study are from a nonclinical sample, the results suggest some potential clinical implications. Knowledge of additional vulnerability factors that may precipitate depression could aide in further refinements of prevention programs and early identification of at-risk individuals, particularly children. Understanding the cognitive mechanisms involved could aid in tailoring specific prevention strategies to the specific content of teasing children are experiencing.
The results may also speak to the treatment of eating disorders among women. It is known that depression and eating disorders are highly comorbid (Kessle, Berglund, Demler, Jin, Merikangas, & Walters, 2005). Elucidating specific biases would be useful, given that research has suggested, for example, that less than half of individuals with bulimia seek treatment for their eating disorder, although the majority of these individuals do seek treatment for an emotional problem (Hudson et al., 2005). Therefore, it may be important to assess for these interpersonal vulnerabilities at the outset of treatment. Understanding the psychological sequelae that may develop in reaction to teasing may aid in the refinement of treatment interventions for these individuals.
We specifically chose to focus on undergraduate women in this sample given evidence that body dissatisfaction increases throughout adolescence (McCabe & Ricciardelli, 2001; Wichstrøm, 1999) and weight-related concerns are particularly salient in this group (Lokken et al., 2003). The current sample focused primarily on undergraduate freshman, who may be susceptible to the weight gain typically seen upon matriculation to university (Butler, Black, Blue, & Gretebeck, 2004; Levitsky, Halbmaier, & Mrdjenovic, 2004). This weight gain might prime women for increased body dissatisfaction as females’ body dissatisfaction is almost always associated with being overweight (for a review, see Bearman et al., 2006). Future research should, however, include men in their sample to examine whether these results are maintained for both genders. In addition, while our sample was relatively diverse, it was still a primarily Caucasian sample. Future studies are needed to determine whether teasing in other samples (e.g., African American or Asian American women) provide similar effects. For example, research has demonstrated that African American adolescents tend to have lower levels of body dissatisfaction then Caucasian adolescents (Paxton et al., 2006).
The limitations of the current study should be acknowledged. First, the study measures relied on individuals’ self-report, which may have been subject to response or recall biases. That is, depressed individuals may be more likely to report higher rates of weight-related teasing as well as higher levels of body dissatisfaction. It is also possible that an unknown third variable might have caused increases in body dissatisfaction and depression (e.g., other interpersonal problems experienced in romantic or friendship relationships). Future research would benefit from including interviewer-administered instruments or an experimental manipulation to assess levels of depressive symptoms, body dissatisfaction, and current experiences of weight-related teasing, which may be less subject to the potential effects of response biases. Additionally, it might be prudent to incorporate other quality of life and interpersonal relationship measures to assess the potential confounding of other variables, as mentioned above. A second limitation is that only one follow-up assessment was included in the study, and it that it was only one month after the initial assessment, which may have limited our ability to observe experiences of teasing and changes in depressive symptoms. This said, however, the follow-up interval was sufficiently long for the hypothesized vulnerability-stress relations to be observed. Further, previous research has found support for the vulnerability-stress hypothesis with follow-up intervals as short as one week (Gibb, Beevers, Andover, & Holleran, 2006). A final limitation is that our focus on undergraduate students may limit the generalizability of the current findings to younger adolescent samples or individuals with more severe levels of psychopathology. That said, previous research that has utilized nationally representative samples of adolescents to examine vulnerability factors predicting depression onset have included individuals up to 18 years of age (e.g., Van Voorhees et al., 2008). The mean age of our sample was 18.64 years, therefore establishing comparison with other studies by conceptualizing our sample as in the stages of late adolescence or young adulthood. Future research is still needed, however, to determine whether current results will extend to younger samples and the prediction of diagnosable episodes of depression.
In summary, the current prospective study provides preliminary support for a specific cognitive vulnerability-stress model of depressive symptoms among young women. Specifically, women’s levels of body dissatisfaction were related to prospective depressive symptom increases in the presence, but not absence of, weight-related teasing. Although women tend to have higher rates of body dissatisfaction than men, future research is needed to assess whether different types of body dissatisfaction among the sexes (i.e., women’s desire to be small versus men’s desire to be muscular) contribute to sex-specific moderation effects.
Footnotes
Post-hoc analyses revealed that individuals who reported current experiences of weight-related teasing had significantly higher body dissatisfaction (mean BSQ = 107.00) than those who did not reported current experiences of weight-related teasing (mean BSQ = 59.46), t(114) = 7.75, p < .001.
References
- Abramson LY, Metalsky GI, Alloy LB. Hopelessness depression: A theory-based subtype of depression. Psychological Review. 1989;96:358–372. [Google Scholar]
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage; 1991. [Google Scholar]
- Allgood-Merten B, Lewinsohn PM, Hops H. Sex differences and adolescent depression. Journal of Abnormal Psychology. 1990;99:55–63. doi: 10.1037//0021-843x.99.1.55. [DOI] [PubMed] [Google Scholar]
- Angold A, Costello EJ, Worthman CM. Puberty and depression: The roles of age, pubertal status and pubertal timing. Psychological Medicine: A Journal of Research in Psychiatry and the Allied Sciences. 1998;28:51–61. doi: 10.1017/s003329179700593x. [DOI] [PubMed] [Google Scholar]
- Barker ET, Galambos NL. Body dissatisfaction of adolescent girls and boys: Risk and resource factors. Journal of Early Adolescence. 2003;23:141–165. [Google Scholar]
- Bearman SK, Presnell K, Martinez E, Stice E. The skinny on body dissatisfaction: A longitudinal study of adolescent girls and boys. Journal of Youth and Adolescence. 2006;35:229–241. doi: 10.1007/s10964-005-9010-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT. Cognitive therapy of depression: New Perspectives. In: Clayton P, editor. Treatment of depression: Old controversies and new approaches. New York: Raven Press; 1983. pp. 265–290. [Google Scholar]
- Beck AT. Cognitive models of depression. Journal of Cognitive Psychotherapy. 1987;1:5–37. [Google Scholar]
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory Manual. 2. San Antonio: The Psychological Corporation; 1996. [Google Scholar]
- Bennett DS, Ambrosini PJ, Kudes D, Metz C, Rabinovich H. Gender differences in adolescent depression: Do symptoms differ for boys and girls? Journal of Affective Disorders. 2005;89:35–44. doi: 10.1016/j.jad.2005.05.020. [DOI] [PubMed] [Google Scholar]
- Blazer DG, Kessler RC, McGonagle KA, Swartz MS. The prevalence and distribution of major depression in a national community sample: The national comorbidity survey. American Journal of Psychiatry. 1994;151:979–986. doi: 10.1176/ajp.151.7.979. [DOI] [PubMed] [Google Scholar]
- Butler SM, Black DR, Blue CL, Gretebeck RJ. Change in diet, physical activity, and body weight in female college freshman. American Journal of Health Behavior. 2004;28:24–32. doi: 10.5993/ajhb.28.1.3. [DOI] [PubMed] [Google Scholar]
- Clark DA, Beck AT, Alford BA. Scientific foundations of cognitive theory and therapy of depression. New York: Wiley; 1999. [Google Scholar]
- Cooper PJ, Taylor MJ, Cooper Z, Fairburn CG. The development and validation of the body shape questionnaire. International Journal of Eating Disorders. 1987;6:485–494. [Google Scholar]
- Edman JL, Yates A, Aruguete MS, DeBord KA. Negative emotion and disordered eating among obese college students. Eating Behaviors. 2005;6:308–317. doi: 10.1016/j.eatbeh.2005.05.004. [DOI] [PubMed] [Google Scholar]
- Fabian LJ, Thompson JK. Body image and eating disturbance in young females. International Journal of Eating Disorders. 1989;8:63–74. [Google Scholar]
- Gibb BE, Beevers CG, Andover MS, Holleran K. The hopelessness theory of depression: A prospective multi-wave test of the vulnerability-stress hypothesis. Cognitive Therapy and Research. 2006;30:763–772. [Google Scholar]
- Hammen C. Cognitive, life stress, and interpersonal approaches to a developmental psychopathology model of depression. Development and Psychopathology. 1992;4:189–206. [Google Scholar]
- Hankin BL, Abramson LY, Moffit TE, Silva PA, McGee R, Angell KE. Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology. 1998;107:128–140. doi: 10.1037//0021-843x.107.1.128. [DOI] [PubMed] [Google Scholar]
- Hankin BL, Mermelstein R, Roesch L. Sex differences in adolescent depression: Stress exposure and reactivity models. Child Development. 2007;78:279–295. doi: 10.1111/j.1467-8624.2007.00997.x. [DOI] [PubMed] [Google Scholar]
- Higgins ET. Self-discrepancy: A theory relating to self and affect. Psychological Review. 1987;94:319–340. [PubMed] [Google Scholar]
- Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry. 2007;61:348–358. doi: 10.1016/j.biopsych.2006.03.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson F, Wardle J. Dietary restraint, body dissatisfaction, and psychological distress: A prospective analysis. Journal of Abnormal Psychology. 2005;114:119–125. doi: 10.1037/0021-843X.114.1.119. [DOI] [PubMed] [Google Scholar]
- Keery H, van den Berg P, Thompson JK. An evaluation of the Tripartite Influence Model of body dissatisfaction and eating disturbance with adolescent girls. Body Image. 2004;1:237–254. doi: 10.1016/j.bodyim.2004.03.001. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- Levitsky DA, Halbmaier CA, Mrdjenovic G. The freshman weight gain: A model for the study of the epidemic of obesity. International Journal of Obesity. 2004;28:1435–1442. doi: 10.1038/sj.ijo.0802776. [DOI] [PubMed] [Google Scholar]
- Little RJA, Rubin DB. Statistical analysis with missing data. New York: Wiley; 1987. [Google Scholar]
- Laessle RG, Kittl S, Fichter MM, Pirke KM. Cognitive correlates of depression in patients with eating disorders. International Journal of Eating Disorders. 1988;7:681–686. [Google Scholar]
- Lokken K, Ferraro FR, Kirchner T, Bowling M. Gender differences in body size dissatisfaction among individuals with low, medium, or high levels of body focus. The Journal of General Psychology. 2003;130:305–310. doi: 10.1080/00221300309601161. [DOI] [PubMed] [Google Scholar]
- McCabe MP, Ricciardelli LA. Parent, peer, and media influences on body image and strategies to both increase and decrease body size among adolescent boys and girls. Adolescence. 2001;36:225–240. [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Girgus JS. The emergence of gender differences in depression during adolescence. Psychological Bulletin. 1994;115:424–443. doi: 10.1037/0033-2909.115.3.424. [DOI] [PubMed] [Google Scholar]
- Oates-Johnson T, Clark DA. Sociotropy, body dissatisfaction and perceived social disapproval in dieting women: A prospective diathesis-stress study of dysphoria. Cognitive Therapy and Research. 2004;28:715–731. [Google Scholar]
- Paxton SJ, Eisenberg ME, Neumark-Sztainer D. Prospective predictors of body dissatisfaction in adolescent girls and boys: A five-year longitudinal study. Developmental Psychology. 2006;42:888–899. doi: 10.1037/0012-1649.42.5.888. [DOI] [PubMed] [Google Scholar]
- Paxton SJ, Neumark-Sztainer D, Hannan PJ, Eisenberg ME. Body dissatisfaction prospectively predicts depressed mood and low self-esteem in adolescents girls and boys. Journal of Clinical Child and Adolescent Psychology. 2006;35:539–549. doi: 10.1207/s15374424jccp3504_5. [DOI] [PubMed] [Google Scholar]
- Rierdan J, Koff E, Stubbs ML. A longitudinal analysis of body image as a predictor of the onset and persistence of adolescent girls’ depression. Journal of Early Adolescence. 1989;9:454–466. [Google Scholar]
- Rosen JC, Jones A, Ramirez E, Waxman S. Body Shape Questionnaire: Studies of validity and reliability. International Journal of Eating Disorders. 1995;20:315–319. doi: 10.1002/(SICI)1098-108X(199611)20:3<315::AID-EAT11>3.0.CO;2-Z. [DOI] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Schutz HK, Paxton SJ. Friendship quality, body dissatisfaction, dieting and disordered eating in adolescent girls. British Journal of Clinical Psychology. 2007;46:67–83. doi: 10.1348/014466506x115993. [DOI] [PubMed] [Google Scholar]
- Stice E, Bearman SK. Body-image and eating disturbances prospectively predict increases in depressive symptoms in adolescent girls: A growth curve analysis. Developmental Psychology. 2001;37:597–607. doi: 10.1037//0012-1649.37.5.597. [DOI] [PubMed] [Google Scholar]
- Stice E, Killen JD, Hayward C, Taylor CB. Support for the continuity hypothesis of bulimic pathology. Journal of Consulting and Clinical Psychology. 1998;66:784–790. [PubMed] [Google Scholar]
- Strauman TJ, Vookles J, Berenstein V, Chaiken S, Higgins ET. Self-discrepancies and vulnerability to body dissatisfaction and disordered eating. Journal of Personality and Social Psychology. 1991;61:946–956. doi: 10.1037//0022-3514.61.6.946. [DOI] [PubMed] [Google Scholar]
- Thompson JK, Coovert MD, Richards KJ, Johnson S, Cattarin J. Development of body image, eating disturbance, and general psychological functioning in female adolescents: Covariance structure modeling and longitudinal investigations. International Journal of Eating Disorders. 1995;18:221–236. doi: 10.1002/1098-108x(199511)18:3<221::aid-eat2260180304>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- Thompson JK, Fabian LJ, Moulton DO, Dunn ME, Altabe MN. Development and validation of the physical appearance related teasing scale. Journal of Personality Assessment. 1991;56:513–521. doi: 10.1207/s15327752jpa5603_12. [DOI] [PubMed] [Google Scholar]
- van den Berg P, Thompson JK, Obremski-Brandon K, Coovert M. The Tripartite Influence model of body image and eating disturbance: A covariance structure modeling investigation testing the mediational role of appearance comparison. Journal of Psychosomatic Research. 2002;53:1007–1020. doi: 10.1016/s0022-3999(02)00499-3. [DOI] [PubMed] [Google Scholar]
- Van Voorhees BW, Paunesku D, Kuwabara SA, Basu A, Gollan J, Hankin BL, Melkonian S, Reinecke M. Protective and vulnerability factors predicting new-onset depressive episode in a representative of U.S. adolescents. Journal of Adolescent Health. 2008;42:605–616. doi: 10.1016/j.jadohealth.2007.11.135. [DOI] [PubMed] [Google Scholar]
- Wichstrøm L. The emergence of gender difference in depressed mood during adolescence: The role of intensified gender socialization. Developmental Psychology. 1999;35:232–245. [PubMed] [Google Scholar]