

Abstract
Rapid eye movement (REM) sleep behavior disorder (RBD) is characterized by dream enactment behavior resulting from a loss of REM skeletal muscle atonia. The neurobiology of REM sleep and the characteristic features of REM atonia have an important basis for understanding the aggravating etiologies the proposed pharmacological interventions in its management. This review outlines the evidence for behavioral and therapeutic measures along with evidence-based guidelines for their implementation, impact on falls, and effect on polysomnography (PSG) while highlighting the non-motor, autonomic, and cognitive impact of this entity. PubMed databases were reviewed upto May 2013 in peer-reviewed scientific literature regarding the pathophysiology and management of RBD in adults. The literature was graded according to the Oxford centre of evidence-based Medicine Levels. An early intervention that helps prevent consequences such as falls and provides a base for intervention with neuroprotective mechanisms and allocates a unique platform that RBD portrays with its high risk of disease conversion with a sufficiently long latency. RBD provides a unique platform with its high risk of disease conversion with a sufficiently long latency, providing an opportunity for early intervention both to prevent consequences such as falls and provide a base for intervention with neuroprotective mechanisms.
Keywords: Behavioral modification, drug therapy including key pharmacological names, medication, RBD OR, REM Sleep behavior disorder and treatment
Materials and Methods
PubMed databases were reviewed upto May 2013 in peer reviewed scientific literature regarding the pathophysiology and management of RBD in adults. The search was limited to articles published in English
Associations with neurological disorders such as Parkinson's disease (PD), narcolepsy, and multisystem atrophy were investigated along with non-motor manifestations such as cognitive, autonomic and cardiac, and sleep apnea.
In reviewing the literature in management of RBD, evidence was graded according to the Oxford centre of evidence- based Medicine Levels. Grade 1: High-quality randomized clinical trials, Grade 2: Low-quality randomized clinical trials or high quality cohort studies, Grade 3: Case-control studies, and Grade 4: Case Series/case reports.[4]
The level of recommendations was as follows:
Level A — Recommended-Evidence level 1.
Level B — Suggested-Evidence level 1-4 fewer studies or expert consensus.
Level C — Considered-Evidence level 3-4.[2]
Introduction
The neurobiology of REM sleep and the characteristic features of REM atonia have an important basis for understanding the aggravating etiologies and the proposed pharmacological interventions in its management. Cholinergic systems activate reticular formation neurons in a positive-feedback interaction to produce the onset of REM. REM is terminated by the inhibitory activity of REM off aminergic neurons, which become active at the end of a REM period due to the recruitment by REM on activity. REM off neuronal activity decreases in SWS and becomes minimal at the onset of REM sleep due to self-inhibitory feedback and adenosinergic inhibition. REM on GABAergic input may inhibit REM off Dorsal Raphe activity during sleep. Cessation of discharge of aminergic neurons during Non-rapid eye movement (NREM)-REM sleep transitions lead to disinhibition of laterodorsal tegmentum/pedunculopontine (LDT/PPT) neurons.[1]
The PSG electroencephalogram (EEG) characteristics of REM sleep observed are a manifestation of the ascending cholinergic activation that promotes EEG desynchrony. The descending cholinergic projections produced muscle atonia via activation of neurons in the pontine reticular formation (PRF) and ventral medial medulla, which in turn project into the spinal cord.[1] Glycine is the prominent inhibitory neurotransmitter that inhibits the spinal motor neuron and thus produces the muscle atonia that is characteristic of REM sleep.
Orexin provides the stability to NREM/REM flip-flop mechanism, and loss of these hypocretin/orexin neurons can manifest as hypersomnia with REM intrusions as seen in narcolepsy.
RBD may be a precursor to synucleionopathies such as PD (15-33%) as well as other neurodegenerative disorders such as multiple system atrophy (70%), dementia with Lewy bodies (40%) and Spinocerebellar Ataxias 2 and 3 when followed longitudinally for upto 10-29 years. RBD has also been reported to have an increased incidence in one-third of patients with narcolepsy.[2]
RBD and Falls
Patients with RBD are at risk for sleep-related injury (SRI), injuring themselves or their spouses with aggressive behavior during sleep, often during attempted dream enactment. Studies show about 33-65% of RBD patients have been reported to have had SRI to self or bed partner. About 30-81% was the reported sleep clinic prevalence of SRI in diagnosed RBD patients.[5,6,7,8] In a series of 92 patients, 64% of the bed partners (53 of 83) sustained punches, kicks, attempted strangulation, and assault with objects.[5] In comparison, a community sample of 1034 elderly surveyed in Hong Kong, 0.8% reported SRI.[9]
Falls prevention: Role of behavioral intervention
Despite apparent unconsciousness, the brain is readily responsive to the environment during REM sleep. Complex auditory sound processing, similar to wakefulness, occurs during REM sleep, and there is a lower threshold for reversibility to wakefulness with auditory stimuli compared to NREM.[10] Further, it has been demonstrated that dream mentation can be altered by verbal stimulation. Anecdotal expert consensus exists on intervention measures to prevent falls in RBD including placing a mattress on the floor, padding corners of furniture, window protection, and removing potentially dangerous objects from the bedroom.
A customized bed alarm pacifying patients with a calming phrase prevented falls in 4 medically refractory RBD patients during vigorous dream enactment behavior. Pre-treatment: 5 serious events, 80 minor events, and 193 near events were observed in over 66 patient-months (4.21events/pt-mo). Post-treatment improvement was noted after a follow up period of 63 pt-months with a marked reduction in events (0.05 event/pt-mo).[11] The study has been summarized in Table 1.
Table 1.
Behavioral: Customized pacifying bed alarm

Fall prevention: Role of pharmacological intervention
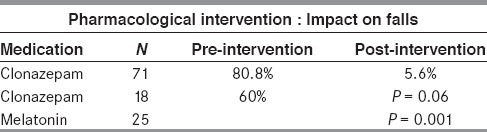
In a case study of 71 patients from Hong Kong, the rate of SRI that included ecchymoses, lacerations, fractures, and subdural hematomas following treatment with clonazepam (CNZP) decreased from 80.8% pre-treatment to 5.6% post-treatment in 62 patients.[7]
In a survey-based study (n = 45), 25 patients received melatonin, 18 were administered CNZP, and two received both as initial treatment. Before treatment, 27 patients (60%) reported an RBD-associated injury. Median dosages were 6 mg for melatonin and 0.5 mg for CNZP. RBD visual analog scale (VAS) ratings were significantly improved following both treatments. Melatonin-treated patients reported less frequent adverse effects than those treated with CNZP[12] [Table 2].
Table 2.
Falls prevention safety: Level of evidence a
Pharmacotherapy of REM Behavior Disorder
CNZP
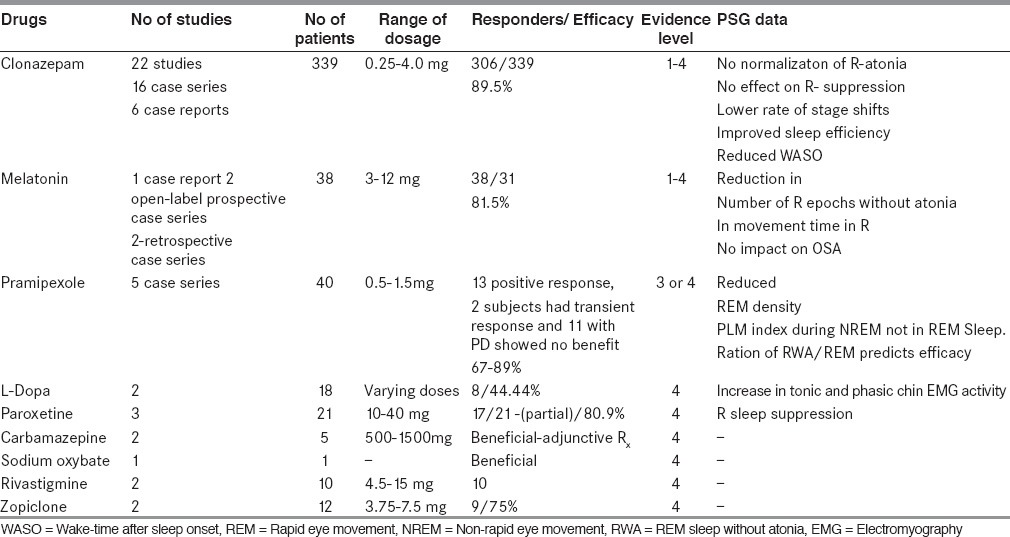
Meta-analysis of 22 studies included 16 case series,[5,6,7,9,13,14,15,16,17,18,19,20,21,22,23,24] six case reports,[25,26,27,28,29,30] and one community[9] sample with a total of 339 subjects, of whom 306 were noted to have complete (249) or partial (57) treatment response to CNZP. The clinical efficacy noted was 80% at Minnesota Regional Sleep Disorders Center.[33] The dosage ranged 0.25-4.0 mg administered 30 minutes prior to bedtime.[8] Women tended to require higher dosage than men.[8] Sustained CNZP efficacy in 89.5% of 57 treated patients. No dose escalation was reported.[7] CNZP also decreased the occurrence of SRI caused by RBD.
CNZP: Video-polysomnographic study
Polysomnography (PSG) variables on patients that were drug-free RBD patients and on CNZP treatment n = 57 patients with 42 untreated iRBD patients, 15 iRBD patients on CNZP (0.5-1 mg) at bedtime. iRBD+Clo patients showed a lower rate of sleep stage shifts, improved sleep efficiency, and lower percentage of wakefulness after sleep onset observed. The CGI scale improved after treatment. No evident common trend was observed for RBD severity scale (RBDSS) or Atonia Index.
Side effects of CNZP included: Sedation, impotence, morning motor incoordination, confusion, memory dysfunction, no reported instance of drug abuse, risk of confusion, or falls.
Pharmacological Intervention with CNZP: Level of Evidence B
Melatonin
The mechanism of melatonin is unclear; it is suggested that it restores RBD-related desychronization of the circadian rhythms. One case report,[33] two open-label prospective case series,[34,35] two retrospective case series[36] (n = 38). Dose: 3-12 mg at bedtime. PSG showed statistically significant decrease in number of R epochs without atonia[36,37] and in movement time in R.[36] Successfully treated patients included those with synucleinopathies including DLB, PD, and MSA memory problems and sleep-disordered breathing.[34,36] Side effects include morning headache, sleepiness, and delusions/hallucinations.
Pharmacological Intervention with Melatonin: Level of Evidence B
Pramipexole
Pramipexole has been studied in the management of RBD in three case studies, two retrospective cohorts with PSG variables including 113 subjects[37,38,39,40,41] with and without synucleinopathies. In a study of eight patients with idiopathic RBD, five patients reported a sustained reduction in the frequency or intensity of sleep motor behaviors, which was confirmed by video recording, although no change was observed for the percentage of phasic electromyographic (EMG) activity during REM sleep.[37] In another study, 10 consecutive patients, 89% of patients experienced either a moderate reduction or complete resolution in the frequency of RBD symptoms throughout the duration of the study. Moreover, 67% reported at least a moderate reduction in the severity of remaining symptoms.[38] In another study, 11 subjects with untreated RBD on levodopa (L-dopa) monotherapy improved PD but did not modify RBD-related symptoms and objective video PSG abnormalities.[39]
In 98 patients with RBD (pramipexole or CNZP), pramipexole was efficacious in 61.7% (50 of 81). The ratio of REM sleep without atonia (RWA)/REM was associated with pramipexole effectiveness. The cut-off rate of RWA/REM for predicting pramipexole effectiveness was estimated as 16.8%. Pramipexole + CNZP showed higher RWA/REM and frequency of vocalization, concluding that pramipexole may play a role in mild iRBD cases with a lower rate of RWA.[40]
Fourteen patients with RBD (80.0%) achieved symptomatic improvement of RBD with pramipexole treatment, which reduced REM density and PLM index during non-REM sleep despite the unchanged amount of RWA. The rate of change in RBD symptoms correlated positively with the rate of REM density reduction. Significant reduction of the PLM index was observed in NREM sleep but not in REM sleep. Pramipexole can improve RBD symptoms, possibly because of changes in dream contents or its amount manifested as the reduction of REM density.[41]
Pharmacological Intervention with Pramipexole: Level of Evidence C
L-Dopa
Limited and Conflicting level 4 Data
PSG showed a statistically significant increase in tonic and phasic chin EMG activity in the group as a whole. The data overall suggest a limited role for L-DOPA in the treatment of RBD at this time.[2]
Acetylcholinesterase Inhibitors
RBD may be due to disruption in R-related cholinergic systems[42] associated with sleep disruption, vivid dreams, and sleep-related disruptive behaviors.[20,43]
Reviewed two papers, six cases, four were associated with neurodegenerative disorders.
Result: Four patients responded at doses between 10 mg and 15 mg,[20,44] and two patients failed to respond to donepezil.
Pharmacological Intervention with Acetylcholinesterase Inhibitors: Level of Evidence C
Rivastigmine
A double-blind, crossover pilot trial was conducted on 12 patients with PD. Dose of 4.6 mg/24 hours for 3 weeks was administered. Side effects: Peripheral cholinergic action.[45]
Other medications
The following medications were considered for treatment of RBD with limited evidence: Zopiclone, benzodiazepines other than CNZP, Yi-Gan San, desipramine, clozapine, carbamazepine, and sodium oxybate[2] [Table 3].
Table 3.
Pharmacological intervention with other medications: Level of evidence C/D
REM-related cardiorespiratory activation is altered in subjects with RBD
Normally observed NREM-to-REM-sleep cardiac excitatory response and parasympathetic withdrawal are absent in patients with idiopathic RBD and symptoms of clinical dysautonomia were more frequent in subjects with idiopathic RBD as compared with age-matched controls. Reduced cardiac uptake of 123I-MIBG (a noradrenaline analog) was observed in subjects with idiopathic RBD.[46]
Relationship between RBD, OSA and medication
RBD might protect against obstructive sleep apnea. Loss of atonia in skeletal muscle in RBD patients could lead to lower severity of OSA with shorter apneas and hypopneas; serotonergic enhancers such as paroxetine, mirtazapine, and glycinergic antagonists could alleviate the severity of OSA by increasing EMG activity.
Cognitive function in REM sleep behavior disorder
Significant worsening in visuospatial learning over time in RBD compared to controls (P = 0.0001). Cognitive decline may coincide or precede the onset of RBD. Cognitive decline occurred in 94% of a sample of patients with RBD. The risk for dementia is limited to those who develop abnormal neurological findings or includes all patients presenting with cryptogenic RBD. Role of intervention in this regard is unclear.[47]
Modulation of EEG with Long-term use of CNZP
With 46 participants, 15 had siRBD, 13 had narcolepsy/RBD, and 18 were normal controls. RBDSS was obtained, and atonia index was computed. NREM sleep instability was evaluated using an automatic quantitative analysis. Patients with iRBD were re-evaluated after 2.75 ± 1.62 years. CNZP modifies NREM sleep in iRBD participants with a decrease in its instability. Wakefulness after sleep onset was decreased together with an increase in both slow-wave sleep (SWS) and sleep stage 2; chin tone was not modified by CNZP. REM atonia index reduced in iRBD participants and reduced in narcolepsy/RBD participants.[48]
Medications aggravating RBD
A recent study, (n = 48)[49] showed an increased risk ratio of being on antidepressants for patients with early-onset RBD effect of SSRI medications on motor tone in R[50] demonstrated that SSRI medications can induce RSWA. β-blockers have also been noted to cause RBD.[51] RBD may be observed in association with R rebound states such as alcohol and barbiturate withdrawal.[52]
Summary
RBD allows an unprecedented opportunity for early and preclinical symptomatic evaluation of patients, as a majority may transition into clinically neurodegenerative disease. Evidence for behavioral and therapeutic measures along with evidence-based guidelines for their implementation has been discussed as well as the clinical impact of autonomic and cognitive impact of this entity. RBD provides a unique platform with its high risk of disease conversion with a sufficiently long latency providing an opportunity for early intervention both to prevent consequences such as falls and provide a base for intervention with neuroprotective mechanisms.[53]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.España RA, Scammell TE. Sleep neurobiology for the clinician. Sleep. 2004;27:811–20. [PubMed] [Google Scholar]
- 2.Aurora RN, Zak RS, Maganti RK, Auerbach SH, Casey KR, Chowdhuri S, et al. Standards of Practice Committee, American Academy of Sleep Medicine. Best practice guide for the treatment of REM Sleep Behavior Disorder (RBD) J Clin Sleep Med. 2010;6:85–95. [PMC free article] [PubMed] [Google Scholar]
- 3.Boeve BF, Silber MH, Saper CB, Ferman TJ, Dickson DW, Parisi JE, et al. Pathophysiology of REM sleep behavior disorder and relevance to neurodegenerative disease. Brain. 2007;130:2770–88. doi: 10.1093/brain/awm056. [DOI] [PubMed] [Google Scholar]
- 4.Phillips B, Ball C, Sackett D, et al. Oxford Centre for Evidence-Based Medicine — Levels of Evidence. 2009. www.cebm.net/levels_of_evidence.asp .
- 5.Olson EJ, Boeve BF, Silber MH. Rapid eye movement sleep behavior disorder: Demographic, clinical and laboratory findings in 93 cases. Brain. 2000;123:331–9. doi: 10.1093/brain/123.2.331. [DOI] [PubMed] [Google Scholar]
- 6.Boeve BF, Silber MH, Ferman TJ, Kokmen E, Smith GE, Ivnik RJ, et al. REM sleep behavior disorder and degenerative dementia: An association likely reflecting Lewy body disease. Neurology. 1998;51:363–70. doi: 10.1212/wnl.51.2.363. [DOI] [PubMed] [Google Scholar]
- 7.Wing YK, Lam SP, Li SX, Yu MW, Fong SY, Tsoh JM, et al. REM sleep behaviour disorder in Hong Kong Chinese: Clinical outcome and gender comparison. J Neurol Neurosurg Psychiatry. 2008;79:1415–6. doi: 10.1136/jnnp.2008.155374. [DOI] [PubMed] [Google Scholar]
- 8.Schenck CH, Mahowald MW. A polysomnographic, neurologic, psychiatric, and clinical outcome report on 70 consecutive cases with REM sleep behavior disorder (RBD): Sustained clonazepam efficacy in 89.5% of 57 treated patients. Clev Clin J Med. 1990;57:9–S23. [Google Scholar]
- 9.Chiu HF, Wing YK, Lam LC, Li SW, Lum CM, Leung T, et al. Sleep-related injury in the elderly — An epidemiological study in Hong Kong. Sleep. 2000;23:513–7. [PubMed] [Google Scholar]
- 10.Takahara M, Nittono H, Hori T. Effect of voluntary attention on auditory processing during REM sleep. Sleep. 2006;29:975–82. doi: 10.1093/sleep/29.7.975. [DOI] [PubMed] [Google Scholar]
- 11.Howell MJ, Arneson PA, Schenck CH. A novel therapy for REM sleep behavior disorder (RBD) J Clin Sleep Med. 2011;7:639–44A. doi: 10.5664/jcsm.1470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McCarter SJ, Boswell CL, St Louis EK, Dueffert LG, Slocumb N, Boeve BF, et al. Treatment outcomes in REM sleep behavior disorder. Sleep Med. 2013;14:237–42. doi: 10.1016/j.sleep.2012.09.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chiu HF, Wing YK, Chung DW, Ho CK. REM sleep behavior disorder in the elderly. Int J Geriat Psychiatry. 1997;12:888–91. [PubMed] [Google Scholar]
- 14.Iranzo A, Molinuevo JL, Santamaria J, Serradell M, Martí MJ, Valldeoriola F, et al. Rapid-eye movement sleep behaviour disorder as an early marker for a neurodegenerative disorder: A descriptive study. Lancet Neurol. 2006;5:572–7. doi: 10.1016/S1474-4422(06)70476-8. [DOI] [PubMed] [Google Scholar]
- 15.Culebras A, Moore JT. Magnetic resonance findings in REM sleep behavior disorder. Neurology. 1989;39:1519–23. doi: 10.1212/wnl.39.11.1519. [DOI] [PubMed] [Google Scholar]
- 16.Husain A, Miller PP, Carwile ST. REM sleep behavior disorder: Potential relationship to post-traumatic stress disorder. J Clin Neurophysiol. 2001;18:148–57. doi: 10.1097/00004691-200103000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Lapierre O, Montplaisir J. Polysomnographic features of REM sleep behavior disorder: Development of a scoring method. Neurology. 1992;42:1371–4. doi: 10.1212/wnl.42.7.1371. [DOI] [PubMed] [Google Scholar]
- 18.Mahowald MW, Schenck CH. Status dissociates — a perspective on states of being. Sleep. 1991:69–79. doi: 10.1093/sleep/14.1.69. [DOI] [PubMed] [Google Scholar]
- 19.Manni R, Terzaghi M. REM behavior disorder associated with epileptic seizures. Neurology. 2005;64:883–4. doi: 10.1212/01.WNL.0000152894.47873.53. [DOI] [PubMed] [Google Scholar]
- 20.Massironi G, Galluzzi S, Frisoni GB. Drug treatment of REM sleep behavior disorders in dementia with Lewy bodies. Int Psychogeriatr. 2003;15:377–83. doi: 10.1017/s1041610203009621. [DOI] [PubMed] [Google Scholar]
- 21.Schenck CH, Boyd JL, Mahowald MW. A parasomnia overlap disorder involving sleepwalking, sleep terrors, and REM sleep behavior disorder in 33 polysomnographically confirmed cases. Sleep. 1997;20:972–81. doi: 10.1093/sleep/20.11.972. [DOI] [PubMed] [Google Scholar]
- 22.Schenck CH, Hurwitz TD, Mahowald MW. REM sleep behaviour disorder: An update on a series of 96 patients and a review of the world literature. J Sleep Res. 1993;2:224–31. doi: 10.1111/j.1365-2869.1993.tb00093.x. [DOI] [PubMed] [Google Scholar]
- 23.Schenck CH, Mahowald MW. Injurious sleep behavior disorders (parasomnias) affecting patients on intensive care units. Intensive Care Med. 1991;17:219–24. doi: 10.1007/BF01709881. [DOI] [PubMed] [Google Scholar]
- 24.Sforza E, Krieger J, Petiau C. REM sleep behavior disorder: Clinical and physiopathological findings. Sleep Med Rev. 1997;1:57–69. doi: 10.1016/s1087-0792(97)90006-x. [DOI] [PubMed] [Google Scholar]
- 25.Bokey K. Conversion disorder revisited: Severe parasomnia discovered. Aust N Z J Psychiatry. 1993;27:694–8. doi: 10.3109/00048679309075833. [DOI] [PubMed] [Google Scholar]
- 26.Kimura K, Tachibana N, Kohyama J, Otsuka Y, Fukazawa S, Waki R. A discrete pontine ischemic lesion could cause REM sleep behavior disorder. Neurology. 2000;55:894–5. doi: 10.1212/wnl.55.6.894. [DOI] [PubMed] [Google Scholar]
- 27.Kumru H, Santamaria J, Tolosa E, Valldeoriola F, Muñoz E, Marti MJ, et al. Rapid eye movement sleep behavior disorder in parkinsonism with parkin mutations. Ann Neurol. 2004;56:599–603. doi: 10.1002/ana.20272. [DOI] [PubMed] [Google Scholar]
- 28.Morfis L, Schwartz RS, Cistulli PA. REM sleep behaviour disorder: A treatable cause of falls in elderly people. Age Ageing. 1997;26:43–44. doi: 10.1093/ageing/26.1.43. [DOI] [PubMed] [Google Scholar]
- 29.Provini F, Vetrugno R, Pastorelli F, Lombardi C, Plazzi G, Marliani AF, et al. Status dissociatus after surgery for tegmental ponto-mesencephalic cavernoma: A state-dependent disorder of motor control during sleep. Mov Disord. 2004;19:719–23. doi: 10.1002/mds.20027. [DOI] [PubMed] [Google Scholar]
- 30.Thomas M, Moore K. Falling asleep. Age Ageing. 2004;33:636–7. doi: 10.1093/ageing/afh180. [DOI] [PubMed] [Google Scholar]
- 31.Personal communication from Schenck CH [Google Scholar]
- 32.Mahowald MW, Schenck CH, Bornemann MA. Pathophysiologic mechanisms in REM sleep behavior disorder. Curr Neurol Neurosci Rep. 2007;7:167–72. doi: 10.1007/s11910-007-0013-7. [DOI] [PubMed] [Google Scholar]
- 33.Kunz D, Bes F. Melatonin effects in a patient with severe REM sleep behavior disorder: Case report and theoretical considerations. Neuropsychobiology. 1997;36:211–4. doi: 10.1159/000119383. [DOI] [PubMed] [Google Scholar]
- 34.Kunz D, Bes F. Melatonin as a therapy in REM sleep behavior disorder patients: An open-labeled pilot study on the possible influence of melatonin on REM-sleep regulation. Mov Disord. 1999;14:507–11. doi: 10.1002/1531-8257(199905)14:3<507::aid-mds1021>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 35.Takeuchi N, Uchimura N, Hashizume Y, Mukai M, Etoh Y, Yamamoto K, et al. Melatonin therapy for REM sleep behavior disorder. Psychiatry Clin Neurosci. 2001;55:267–9. doi: 10.1046/j.1440-1819.2001.00854.x. [DOI] [PubMed] [Google Scholar]
- 36.Boeve BF, Silber MH, Ferman TJ. Melatonin for treatment of REM sleep behavior disorder in neurologic disorders: Results in 14 patients. Sleep Med. 2003;4:281–4. doi: 10.1016/s1389-9457(03)00072-8. [DOI] [PubMed] [Google Scholar]
- 37.Fantini ML, Gagnon JF, Filipini D, Montplaisir J. The effects of pramipexole in REM sleep behavior disorder. Neurology. 2003;61:1418–20. doi: 10.1212/wnl.61.10.1418. [DOI] [PubMed] [Google Scholar]
- 38.Schmidt MH, Koshal VB, Schmidt HS. Use of pramipexole in REM sleep behavior disorder: Results from a case series. Sleep Med. 2006;7:418–23. doi: 10.1016/j.sleep.2006.03.018. [DOI] [PubMed] [Google Scholar]
- 39.Kumru H, Iranzo A, Carrasco E, Valldeoriola F, Marti MJ, Santamaria J, et al. Lack of effects of pramipexole on REM sleep behavior disorder in Parkinson disease. Sleep. 2008;31:1418–21. [PMC free article] [PubMed] [Google Scholar]
- 40.Sasai T, Matsuura M, Inoue Y. Factors associated with the effect of pramipexole on symptoms of idiopathic REM sleep behavior disorder. Parkinsonism Relat Disord. 2013;19:153–7. doi: 10.1016/j.parkreldis.2012.08.010. [DOI] [PubMed] [Google Scholar]
- 41.Sasai T, Inoue Y, Matsuura M. Effectiveness of pramipexole, a dopamine agonist, on rapid eye movement sleep behavior disorder. Tohoku J Exp Med. 2012;226:177–81. doi: 10.1620/tjem.226.177. [DOI] [PubMed] [Google Scholar]
- 42.Rye DB. Contributions of the pedunculopontine region to normal and altered REM sleep. Sleep. 1997;20:757–88. doi: 10.1093/sleep/20.9.757. [DOI] [PubMed] [Google Scholar]
- 43.Moraes WA, Poyares DR, Guilleminault C, Ramos LR, Bertolucci PH, Tufik S. The effect of donepezil on sleep and REM sleep EEG in patients with Alzheimer disease: A double-blind placebo-controlled study. Sleep. 2006;29:199–205. doi: 10.1093/sleep/29.2.199. [DOI] [PubMed] [Google Scholar]
- 44.Ringman JM, Simmons JH. Treatment of REM sleep behavior disorder with donepezil: A report of three cases. Neurology. 2000;55:870–1. doi: 10.1212/wnl.55.6.870. [DOI] [PubMed] [Google Scholar]
- 45.Di Giacopo R, Fasano A, Quaranta D, Della Marca G, Bove F, Bentivoglio AR. Rivastigmine as alternative treatment for refractory REM behavior disorder in Parkinson's disease. Mov Disord. 2012;27:559–61. doi: 10.1002/mds.24909. [DOI] [PubMed] [Google Scholar]
- 46.Treglia G, Cocciolillo F, Stefanelli A, Cason E, Giordano A. Usefulness of MIBG scintigraphy in idiopathic REM sleep behavior disorder: A systematic review. Res Rep Nucl Med. 2011;2011:1–7. [Google Scholar]
- 47.Huang J, Zhang J, Lam SP, Li SX, Ho CK, Lam V, et al. Amelioration of obstructive sleep apnea in REM sleep behavior disorder: Implications for the neuromuscular control of OSA. Sleep. 2011;34:909–15. doi: 10.5665/SLEEP.1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ferri R, Zucconi M, Marelli S, Plazzi G, Schenck CH, Ferini-Strambi L. Effects of long-term use of clonazepam on nonrapid eye movement sleep patterns in rapid eye movement sleep behavior disorder. Sleep Med. 2013;14:399–406. doi: 10.1016/j.sleep.2013.01.007. [DOI] [PubMed] [Google Scholar]
- 49.Teman P, Tippman-Peikert M, Silber MH, Slocumb NL, Robert Auger R. Idiopathic rapid-eye movement sleep disorder: Associations with antidepressants, psychiatric diagnoses, and other factors, in relation to age of onset. Sleep Med. 2009;10:60–5. doi: 10.1016/j.sleep.2007.11.019. [DOI] [PubMed] [Google Scholar]
- 50.Winkelman JW, James L. Serotonergic antidepressants are associated with REM sleep without atonia. Sleep. 2004;27:317–21. doi: 10.1093/sleep/27.2.317. [DOI] [PubMed] [Google Scholar]
- 51.Iranzo A, Santamaria J. Bisoprolol-induced rapid eye movement sleep behavior disorder. Am J Med. 1999;107:390–2. doi: 10.1016/s0002-9343(99)00245-4. [DOI] [PubMed] [Google Scholar]
- 52.Silber MH. REM sleep behavior disorder associated with barbiturate withdrawal. Sleep Res. 1996;25:371. [Google Scholar]
- 53.Postuma RB, Gagnon JF, Montplaisir JY. REM Sleep Behavior Disorder and Prodromal Neurodegeneration — Where Are We Headed? Tremor Other Hyperkinet Mov (N Y) 2013:3. doi: 10.7916/D8N879HS. [DOI] [PMC free article] [PubMed] [Google Scholar]