

Sir,
A 36-year-old woman presented to emergency department with 1 hour history of dysarthria and left hemiplegia. She did not have diabetes mellitus, hypertension, valvular heart disease or atrial fibrillation. National Institutes of Health Stroke Scale (NIHSS) was 12 on admission. Non-contrast computed tomography (CT) brain on admission was normal. CT angiogram showed occlusion of M1 segment of right middle cerebral artery [Figure 1]. She was on the second day of her menstruation. She did not have any other absolute or relative contraindication for thrombolysis. Intravenous thrombolysis with tissue plasminogen activator (tpA) 0.9 mg/kg was initiated 2 hours from the onset of stroke. MRI brain done 12 hours after thrombolysis showed evidence of ischemic infarct in the territory of anterior division of right middle cerebral artery [Figures 2 and 3]. However, MR angiogram showed complete recanalization of right middle cerebral artery [Figure 4]. There was no increase in her menstrual bleeding or drop in hemoglobin and packed cell volume. Two-dimensional echo, vasculitic and hypercoagulable work-up were unremarkable. She improved and was discharged after 6 days of hospitalization. NIHSS was 4 on discharge from the hospital.
Figure 1.
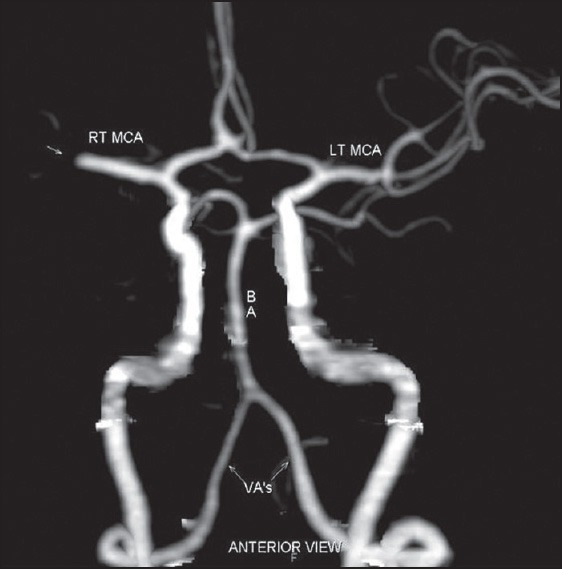
CT angiogram showing occlusion of right M1 segment
Figures 2 and 3.
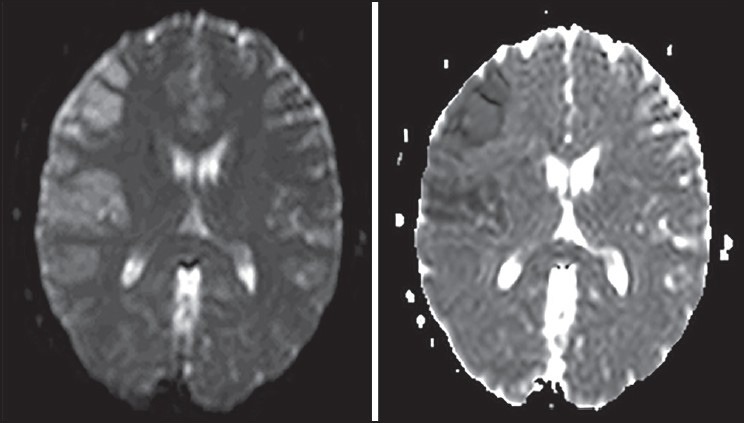
DWI and ADC images showing acute right middle cerebral artery infarct
Figure 4.
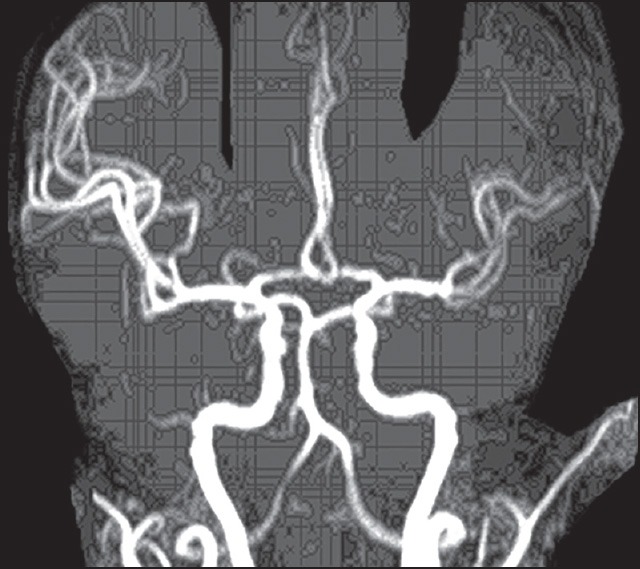
Post-thrombolysis MR angiogram showing complete recanalization of right middle cerebral artery
Menstruation is a relative contraindication for intravenous thrombolysis in stroke. During the first 20 hours of menstruation, hemostasis is maintained predominantly by platelet plugs and fibrin. Hemostasis after the initial 20 hours of menstruation is maintained by constriction of the spiral arterioles in the basal layers of the endometrium, myometrial contraction and tissue regeneration, and is not dependent on clot formation. Clot formation does not occur as the endometrium releases plasminogen activators.[1]
There is very limited data regarding safety of thrombolysis for stroke in menstruating women. Nine subjects were coded as actively menstruating in the NINDS trial (4 placebo and 5 in the treatment). Of the 5 patients who received tpA, 2 had adverse events. One subject in the treatment group who had a 1-year history of dysfunctional uterine bleeding required emergent uterine artery ligation.[2] Wein et al. have reported successful thrombolysis with intravenous tpA in a 46-year-old woman with left middle cerebral artery occlusion. She had presented within 20 hours of menstruation and required 2 packed cell transfusions due to increased menstrual bleeding.[3]
With the available limited data and understanding the physiology of menstrual bleed, intravenous thrombolysis may be administered safely in menstruating females, presenting with stroke, after first day of menstruation. Intravenous thrombolysis should be done cautiously in the first 20 hours of menstruation. Patients should be counseled regarding increased menstrual bleeding and possible requirement of transfusion in such situations. In individuals with dysfunctional uterine bleeding, intravenous thrombolysis may be avoided as hemostatic control normally present during menstruation is not applicable in this circumstance. Mechanical thrombolysis will be a safer alternative, especially during first day of menstruation and in pathological states like dysfunctional uterine bleeding. To the best of our knowledge, this is the first Indian report of safe and successful intravenous thrombolysis for acute ischemic stroke in a menstruating woman.
References
- 1.Christiaens GC, Sixma JJ, Haspels AA. Hemostasis in menstrual endometrium: A review. Obstet Gynecol Surv. 1982;37:281–303. doi: 10.1097/00006254-198205000-00001. [DOI] [PubMed] [Google Scholar]
- 2.The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–7. doi: 10.1056/NEJM199512143332401. [DOI] [PubMed] [Google Scholar]
- 3.Wein TH, Hickenbottom SL, Morgenstern LB, Demchuk AM, Grotta JC. Safety of tissue plasminogen activator for acute stroke in menstruating women. Stroke. 2002;33:2506–8. doi: 10.1161/01.str.0000030108.47462.4f. [DOI] [PubMed] [Google Scholar]