

Abstract
Background:
Stroke in the young is particularly tragic because of its potential to create a long-term burden on the victims, their families, and the community. There had been relatively few studies on young stroke in Kerala's socio-economic setup, that too encapsulating the mentioned apparently relevant dimensions of stroke in the young.
Objective:
To study the prevalence, patterns and risk factors of young stroke.
Settings and Design:
A cross-sectional study with case control comparison at Government Medical College Hospital, Thiruvananthapuram, Kerala, India.
Materials and and Methods:
Total 100 stroke patients were identified over a period of 2 months, and data were collected on the basis of questionnaire developed for the purpose.
Results:
Of 100 stroke patients, 15 had stroke in the young, among which 9 (60%) had ishaemic stroke. Hypertension was the most common risk factor. Smoking, alcohol, atrial fibrillation, and hyperlipidemia were found to be more common in cases (young stroke) when compared with controls. Alcohol use and atrial fibrillation were significantly higher among young stroke patients. Physical inactivity was significantly lesser in those with stroke in the young than elderly. Atrial fibrillation emerged as an independent risk factor of stroke in the young with adjusted odds ratio of 6.18 (1.31-29.21).
Conclusion:
In all, 15% of total stroke occurred in young adults <50 years. The proportion of hemorrhagic stroke in young adults is higher than in elderly. Atrial fibrillation is identified as an independent risk factor of stroke in the young. Compared with stroke in elderly alcohol use, smoking, hyperlipidemia, and cardiac diseases, which are known risk factors, are higher in young stroke.
Keywords: Atrial fibrillation, Thiruvananthapuram, young stroke
Introduction
Stroke is a global health problem and a leading cause of adult disability.[1] Stroke is the second major cause of death worldwide[2] and the fourth major cause of death in India, the death rate being 0.6/1000 in India.[3] Of 35 million deaths attributable to chronic non-communicable diseases that occurred worldwide in 2005, stroke was responsible for 5.7 million (16.6%) deaths, and 87% of these deaths occurred in low- and middle-income countries.[2] According to WHO, by 2020, stroke will become the leading cause of both death and disability worldwide, with the number of fatalities projected to over 20 million and by 2030 to over 24 million a year.
Although stroke is predominantly a disease of the middle age and the elderly, its occurrence in younger age groups is not rare. It has emerged as an important cause of morbidity and mortality in young adults, especially in developing countries. Stroke in the young is particularly tragic because of its potential to create a long-term burden on the victims, their families, and the community. Also, it results in mortality[4] and a great loss of potential years of their lives. Studies show that in India, 10-15% of the total stroke cases are young stroke, and in Kerala, the proportion is 3.8% under the age of 40 and 9.5% under the age of 50.[5] Moreover, there had been relatively few studies on young stroke in Kerala's socio-economic setup, that too encapsulating the mentioned apparently relevant dimensions of stroke in the young. It is against this background that we tried to find the prevalence, pattern, and risk factors of stroke in the young adults.
Materials and Methods
This is a cross-sectional study with case control comparison to identify the risk factors of stroke in the young conducted during August-September 2013 in the department of Medicine at the Government Medical College Hospital, Thiruvananthapuram, Kerala — a tertiary referral center in South India. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all participants. All patients admitted with definite diagnosis of stroke during the study period, were prospectively enrolled.
The diagnosis of stroke was established clinically and confirmed by neuroimaging (non-contrast CT head). Those who were unwilling to give informed written consent were excluded from the study. The study subjects were grouped into cases and controls as per the following demarcation based on age:
Case
Patients having stroke acquired at less than or equal to 50 years of age with a definite diagnosis of stroke.
Control
Patients having stroke acquired above 50 years of age with a definite diagnosis of stroke.
Information regarding the relevant variables in the study was collected by interviewer-administered questionnaire from patients admitted to the medical wards, their bystanders, and case sheets. Ward register was used to identify the eligible study subjects. The risk factors of young stroke were assessed with the help of a structured questionnaire. Non-modifiable risk factors like age, gender, and genetic predisposition and the common modifiable risk factors like hypertension, diabetes mellitus, smoking, dyslipidemia, alcohol, obesity, coronary artery disease (CAD), transient ischemic attack (TIA), and lack of exercise were inquired into.[6]
Patients admitted to the medical wards were visited on the post admission day. The patient was interviewed on the basis of the questionnaire prepared for the purpose. In case, if the patient was not able to give answers to the questions, necessary information was obtained from the bystander and other available sources.
Data obtained in the study were subjected to statistical analysis with Statistical Package for Social Sciences (SPSS) version 11. Bivariate analysis was done to find the risk factors of young stroke using chi-square test. Multivariate analysis was done using logistic regression.
Definition of Important Study Variables
Stroke is defined according to WHO criteria as “rapidly developing clinical symptoms and/or signs of focal, and at times global, loss of cerebral function, with symptoms lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.”[7]
Hypertension
Patient is taking either antihypertensive drugs or if the blood pressure is >140 mm of Hg systolic and >90 mmHg diastolic in two measurements.[8]
Diabetes mellitus
Patient is already diagnosed as diabetic or has fasting plasma glucose ≥126 mg/dl (7.0 mmol/l) or 2-h plasma glucose ≥200 mg/dl (11.1 mmol/l).[9]
Current smoker/smokeless tobacco user
Someone who at the time of the study, smokes/uses tobacco in any form either daily or occasionally.[10]
Current drinker
Those who consumed one or more than one drink of any alcohol in the year preceding the study.[10]
Hypercholesterolemia
Patient with total serum cholesterol ≥6.2 (mmol/l) or 240 mg/dl).[11]
Transient ischemic attacks
Focal, reversible, neurological deficit of sudden onset and <24-hour duration.[12]
Young stroke is considered as stroke in patients less than or equal to 50 years of age.[13,14,15]
Results
Socio-demographic characteristics
During the 2-month study period, 100 stroke patients were identified. The age of incidence ranged from 37 years to 88 years having a mean age of 65.30 ± 12.80. The median age of stroke patients was 66.5 years (interquartile range 20); 85% of patients were aged >50 years, and 66.7% of young adults were having more than primary education, which is much higher when compared with patients >50 years.
Young stroke
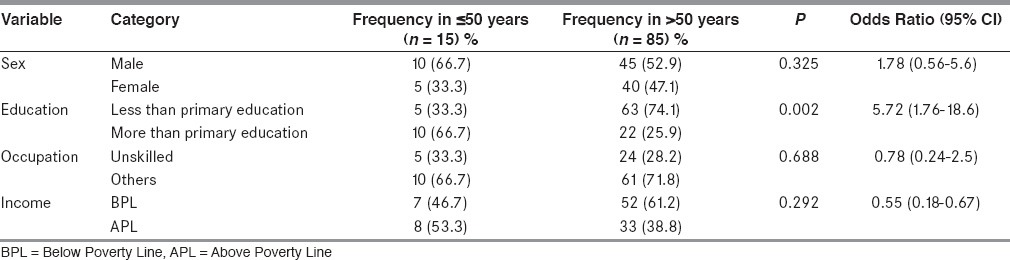
Out of the total, 15% were identified as stroke in the young, out of which 60% were ischemic and 40% were hemorrhagic. In young stroke, males have more preponderance compared to stroke in elderly (66.7% versus 52.9%). Table 1 shows the relation between socio-demographic characteristics of stroke in the young and that of elderly.
Table 1.
Relation between socio-demographic characteristics of stroke in ≤50 and >50 years
Risk factors
Hypertension was the most common risk factor in young stroke (80%). Smoking, alcohol, atrial fibrillation, and hyperlipidemia were found to be more common in cases (young stroke) when compared with control [Tables 2–4]. However, only alcohol use and atrial fibrillation were significantly higher among young stroke patients. Physical inactivity was significantly lesser in young adults.
Table 2.
Comparison of frequencies of stroke risk factors in ≤50 years and >50 years
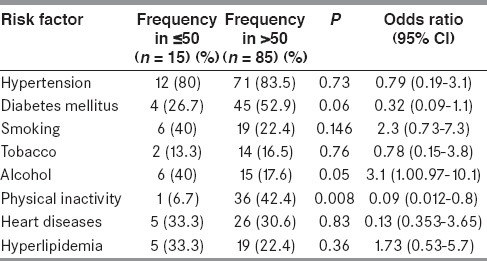
Table 4.
Other risk factors in stroke patients ≤50 years and >50 years compared
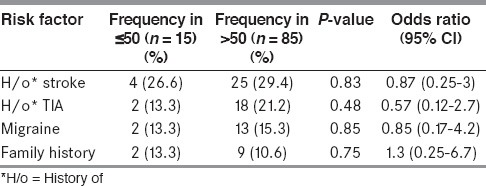
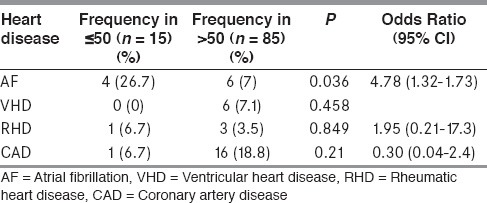
Table 3.
Comparison of frequency of heart diseases in stroke patients ≤50 years and >50 years
Multivariable analysis was done using logistic regression. All those variables with significance level of 0.5, namely, alcohol use, atrial fibrillation, smoking, and hyperlipidemia were included in the analysis. After this, only atrial fibrillation emerged as an independent risk factor of young stroke with adjusted odds ratio of 6.18 (1.31-29.21).
Pattern of young stroke
On analyzing the pattern of young stroke, it was found that only 60% were of ischemic type compared to 72.9% in >50-year-old patients. Young adults showed a more tendency for hemorrhagic stroke than elderly. On analyzing the severity of stroke in ≤50 and >50, it was found that stroke in the young were less severe.
Clinical features
On comparing the clinical features of presentation of young adults with that of elderly, it was found that facial palsy, vomiting, and headache are more common in young adults, whereas altered sensorium, seizures, and vertigo are less common [Figure 1].
Figure 1.
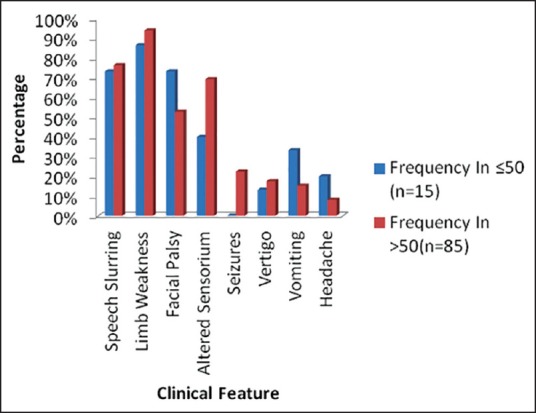
Clinical features of young stroke in comparison with elderly
Discussion
The study gathered information from 100 respondents admitted in the medicine wards of Trivandrum Medical College.
In this study, 4% were ≤40 years and 15% aged ≤50 years, which is substantiated by the data from Trivandrum Stroke Registry[4] in which 3.8% of incident strokes occurred in people aged ≤40 years, 9.5% occurred in people aged ≤50 years. This implies that a slightly higher percentage have developed stroke between 40 and 50 years, pointing toward the increasing incidence of stroke in young within past 4 years.
Sex ratio usually shows a slight male preponderance in the ischemic stroke in young adults (55-71% males).[16,17,18] In the present study also, this trend was observed with males constituting 66.7% of the young adults with stroke. However, in a retrospective study of stroke in young adults,[19] there was a slight female preponderance (52.4%).
When the educational status of the respondents was analyzed, it was found that frequency of patients with more than primary education was significantly higher. At the same time, the percentage of sedentary workers among young stroke patients was lesser when compared with older stroke patients. Also the percentage having low physical activity was significantly less in patients with stroke in the young compared to elderly. This may be because of the obvious reason that younger population tends to involve in more physical activity than elderly population. Increased frequency of higher education in young adults when compared with elderly may be due to the change in outlook of people regarding education, increase in the options, and chances for seeking higher education.
Hemorrhagic stroke was found to be more common in young adults when compared with elderly. Another study[20] supports this result. The leading risk factors of young stroke were hypertension (80%), smoking (40%), hyperlipidemia (33.3%), and cardiac diseases (33.3%). A study on the characteristics of young stroke[20] came up with the leading risk factors as smoking (56%) and hypertension (45%), which supports the study done.
In this study, cardiac risk factors were identified in 33.3% of cases. This higher frequency may be attributed to higher prevalence of atrial fibrillation and rheumatic heart disease in the population referred to the study setting compared with developed countries. Atrial fibrillation was the leading cardiac cause of ischemic stroke in young adults (26.7%). This statistics is similar to that in a study of stroke etiology in European young adults[15] where the most frequent high-risk sources were atrial fibrillation/flutter (15.1%) and cardiomyopathy (11.5%).
Conclusion
The study was helpful in analyzing the prevalence, pattern, and risk factors of young stroke patients admitted in the medical wards of Medical College, Thiruvananthapuram.
In all, 15% of the total stroke occurs in young adults <50 years. The proportion of hemorrhagic stroke in young adults is higher than that of the same in elderly. Atrial fibrillation is identified as an independent risk factor of stroke in the young. Compared to stroke in elderly alcohol use, smoking, hyperlipidemia, and cardiac diseases, which are known risk factors, are higher in patients with young stroke. The higher proportion of stroke in young age group and the higher prevalence of risk factors of stroke in young, point toward the need for more active interventions in the community for prevention of young stroke.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008;371:1612–23. doi: 10.1016/S0140-6736(08)60694-7. [DOI] [PubMed] [Google Scholar]
- 2.Strong K, Mathers C, Bonita R. Preventing stroke: Saving lives around the world. Lancet Neurol. 2007;6:182–7. doi: 10.1016/S1474-4422(07)70031-5. [DOI] [PubMed] [Google Scholar]
- 3.Park K. 22th ed. Jabalpur: Bhanot; 2013. Park's Textbook of Preventive and Social Medicine; pp. 348–9. [Google Scholar]
- 4.Rathore JA, Kango ZA, Mehraj A. Predictors of mortality after acute stroke a prospective hospital based study. J Ayub Med Coll Abbottabad. 2011;23:144–6. [PubMed] [Google Scholar]
- 5.Sridharan SE, Unnikrishnan JP, Sukumaran S, Sylaja PN, Nayak SD, Sarma PS, et al. Incidence, types, risk factors, and outcome of stroke in developing country: The Trivandrum Stroke Registry. Stroke. 2009;40:1212–8. doi: 10.1161/STROKEAHA.108.531293. [DOI] [PubMed] [Google Scholar]
- 6.Lipska K, Sylaja PN, Sarma PS, Thankappan KR, Kutty VR, Vasan RS, et al. Risk factors for acute ischaemic stroke in young adults in South India. J Neurol Neurosurg Psychiatry. 2007;78:959–63. doi: 10.1136/jnnp.2006.106831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yao XY, Lin Y, Geng JL, Sun YM, Chen Y, Shi GW, et al. Age- and gender-specific prevalence of risk factors in patients with first-ever ischemic stroke in china. Stroke Res Treat 2012. 2012 doi: 10.1155/2012/136398. 136398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hatano S. Experience from a multicenter stroke register: A preliminary report. Bull World Health Organ. 1976;54:541–53. [PMC free article] [PubMed] [Google Scholar]
- 9.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National High Blood Pressure Education Program Coordinating Committee. The seventh report of the joint committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA. 2003;289:2560–72. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 10.Government of India ministry of health and family welfare. Integrated Disease Surveillance Project. [Last accessed on 2013 January 10]. Available from: http://www.idsp.nic.in .
- 11.Roth GA, Fihn SD, Mokdad AH, Aekplakorn W, Hasegawa T, Lim SS. High total serum cholesterol, medication coverage and therapeutic control: An analysis of national health examination survey data from eight countries. Bull World Health Organ. 2011;89:92–101. doi: 10.2471/BLT.10.079947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Davenport R, Dennis M. Neurological emergencies: Acute stroke. J Neurol Neurosurg Psychiatry. 2000;68:277–88. doi: 10.1136/jnnp.68.3.277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guo R, Liu H, Li M, Liu L, Yang F, Yin Q, et al. Cerebral arteriostenosis associated with elevated serum-immunoglobulin E level in young adults without risk factors for ischemic stroke: A possible manifestation of cerebral vasculitis? J Clin Neurosci. 2014;21:95–9. doi: 10.1016/j.jocn.2013.03.028. [DOI] [PubMed] [Google Scholar]
- 14.Naess H, Nyland HI, Thomassen L, Aarseth J, Nyland G, Myhr KM. Incidence and short-term outcome of cerebral infarction in young adults in western Norway. Stroke. 2002;33:2105–8. doi: 10.1161/01.str.0000023888.43488.10. [DOI] [PubMed] [Google Scholar]
- 15.Yesilot Barlas N, Putaala J, Waje-Andreassen U, Vassilopoulou S, Nardi K, Odier C, et al. Etiology of first-ever ischaemic stroke in European young adults: The 15 cities young stroke study. Eur J Neurol. 2013;20:1431–9. doi: 10.1111/ene.12228. [DOI] [PubMed] [Google Scholar]
- 16.Kristensen B, Malm J, Carlberg B, Stegmayr B, Backman C, Fagerlund M, et al. Epidemiology and etiology of ischemic stroke in young adults aged 18 to 44 years in northern Sweden. Stroke. 1997;28:1702–9. doi: 10.1161/01.str.28.9.1702. [DOI] [PubMed] [Google Scholar]
- 17.Adams HP, Jr, Kappelle LJ, Biller J, Gordon DL, Love BB, Gomez F, et al. Ischemic stroke in young adults: Experience in 329 patients enrolled in the Iowa Registry of stroke in young adults. Arch Neurol. 1995;52:491–5. doi: 10.1001/archneur.1995.00540290081021. [DOI] [PubMed] [Google Scholar]
- 18.Bogousslavsky J, Pierre P. Ischemic stroke in patients under age 45. Neurol Clin. 1992;10:113–24. [PubMed] [Google Scholar]
- 19.Harirchian MH, Ghaffarpour M, Doratotaj D, Akhavirad MB. Stroke in young adults: A retrospective study of 68 cases. Acta Med Iran. 2006;44:119–24. [Google Scholar]
- 20.Smajlović D, Salihović D, Ibrahimagić OC, Sinanović O. Characteristics of stroke in young adults in Tuzla Canton, Bosnia and Herzegovina. Coll Antropol. 2013;37:515–9. [PubMed] [Google Scholar]