

Abstract
Neuro radiological findings in Dengue encephalitis are non specific. Here we report a case of Dengue encephalitis with transient splenial hyperintensity appearing as dot sign on magnetic resonance imaging of brain.
Keywords: Dengue encephalitis, dot sign, transient splenial hyperintensity
Introduction
Dengue viral infections represent a significant burden of disease in the Tropics. Neurological manifestations such as encephalitis and meningitis can be associated with dengue infection. We report a case of dengue encephalitis in a young woman having transient signal change in the splenium of corpus callosum (“Dot sign”) on magnetic resonance imaging (MRI).
Case Report
An apparently normal young female of 18 years of age had moderate grade fever with generalized lassitude and myalgia for 5 days. She developed headache and vomiting after 1 day, followed by altered sensorium in form of progressive drowsiness. On general physical examination, she had petechial rashes all over the body. Neurological examination revealed a drowsy patient without lateralizing signs. Laboratory investigations showed thrombocytopenia and reactive lymphocytosis. Renal function parameters and electrolytes were normal. She had mild elevation of liver enzymes with normal bilirubin. Blood tests were negative for malaria, enteric fever, leptospirosis, and rickettsial fever. Blood and urine cultures were sterile. Enzyme-linked immunosorbent assay (ELISA) for IgM Dengue was positive. MRI Brain (Flair/T2W) showed hyperintensity in the splenium of corpus callosum, having the appearance of a dot [“Dot sign”; Figure 1]. The lesion was hypointense on T1w image [Figure 2]. and showed restricted diffusion on MRI brain diffusion-weighted image [Figure 3]. On ADC mapping, the lesion had low apparent diffusion coefficient [Figure 4]. The hyperintensity was more prominent on DWI when compared to FLAIR and T2W sequences. Patient improved with symptomatic medical management.
Figure 1.
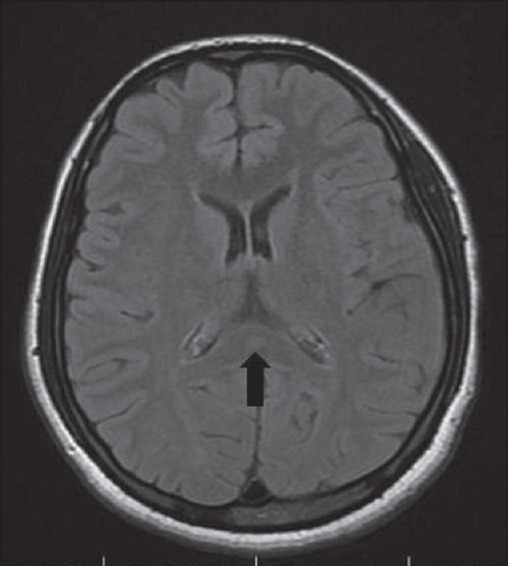
MRI brain FLAIR sequence showing hyperintensity in the splenium of corpus callosum (black arrow)
Figure 2.
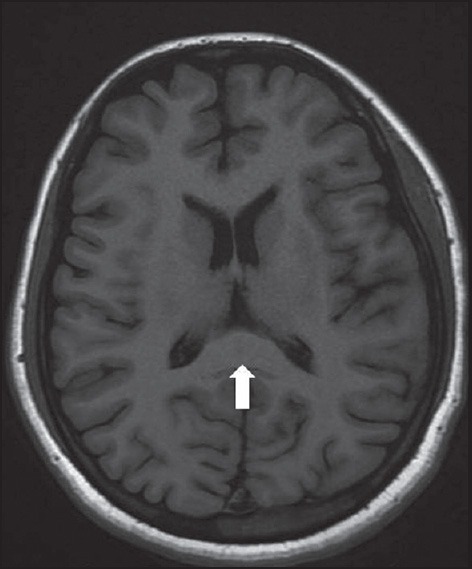
MRI brain T1W image showing hypointensity in the splenium of corpus callosum (white arrow)
Figure 3.
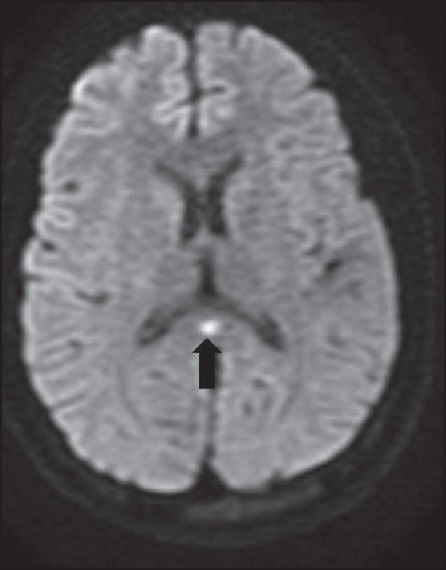
MRI brain Diffusion sequence showing hyperintensity in the splenium of corpus callosum (black arrow)
Figure 4.
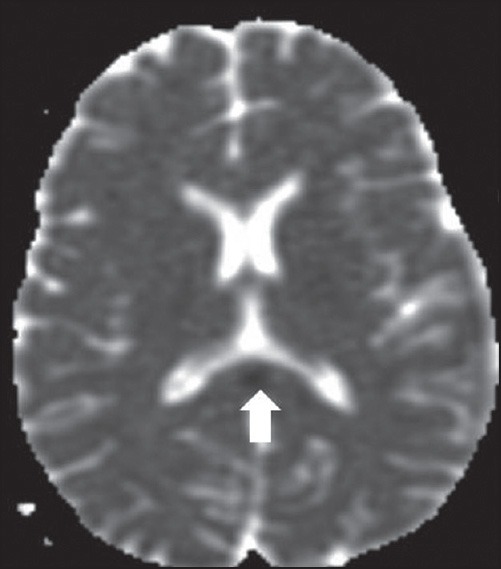
ADC mapping showing decreased apparent diffusion co-efficient (white arrow)
Discussion
Neurological involvement occurs in 4-5% of dengue infections. Most common neurologic manifestation of dengue fever is encephalitis. MRI is superior to computed tomography (CT) scan in demonstrating brain lesions in viral encephalitis. A retrospective study of 225 confirmed cases of dengue showed findings such as generalized cerebral edema, focal involvement of globus pallidus and internal capsule, pontine hemorrhage, acute disseminated encephalomyelitis, and involvement of cervical and thoracic spinal cord.[1] In Misra's 11 patients, MRI was performed on nine; all were normal bar one patient with hyperintense areas in the globus pallidus.[2] Kamble et al. have described a case featuring Japanese Encephalitis-like thalamic involvement visualized on CT (Japanese Encephalitis was excluded by serological tests).[3] MRI lesions in the hippocampi is also described.[4] Transient signal alteration in the splenium of corpus callosum on MRI Brain manifesting as “dot sign” in dengue encephalitis has not been described in literature to date.
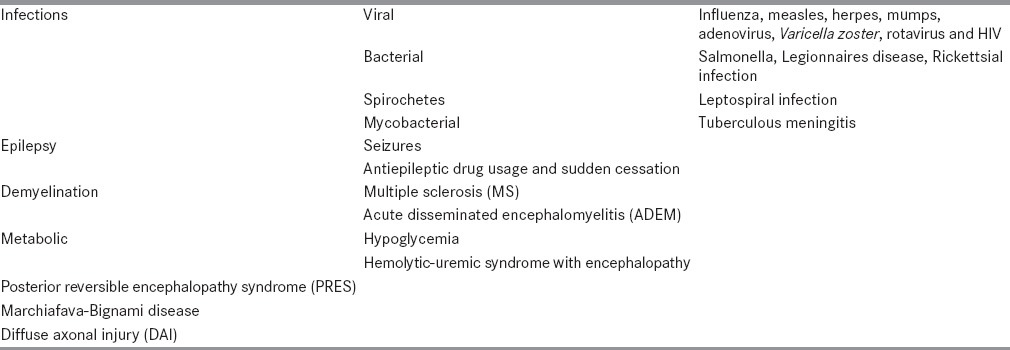
Transient splenial hyperintensity (TSH) has been reported in a variety of conditions, including infections, demyelination, ischemia, and metabolic abnormalities [Table 1].[5] TSH can be seen in two distinct patterns, either as a well-circumscribed, small, oval lesion in the midline within the substance of the corpus callosum (dot sign) or as a more extensive ill-defined, irregular lesion extending throughout the splenium and into the adjacent hemispheres (boomerang sign). The proposed mechanisms implicated include a transient breakdown of the blood-brain barrier, extrapontine osmotic myelinolysis due to sodium and glucose imbalance, intramyelinic edema due to inflammation and migration of inflammatory cells, cytokine-mediated immunologic reaction leading to microvascular endothelial injury, direct viral invasion of neurons, and toxicity or hypersensitivity to antiepileptic drugs (AEDs).[6] The clinical significance of this sign is not certain and may indicate a non-specific brain injury. TSH is an isolated, silent, reversible lesion and it should not be mistaken for something more sinister. These are usually asymptomatic and do not produce features of disconnection syndromes such as apraxia. They are fully reversible and disappear after few weeks.
Table 1.
Causes of transient splenial hyperintensity
Conclusion
Much of the neuroimaging data in dengue infection is diverse, and a decisive characterization of the MRI features of dengue encephalitis is not yet possible, although the focal nature of imaging abnormalities such “dot sign” may add weight to the theory of viral neurotropism.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Wasay M, Channa R, Jumani M, Shabbir G, Azeemuddin M, Zafar A. Encephalitis and myelitis associated with dengue viral infection clinical and neuroimaging features. Clin Neurol Neurosurg. 2008;110:635–40. doi: 10.1016/j.clineuro.2008.03.011. [DOI] [PubMed] [Google Scholar]
- 2.Misra UK, Kalita J, Syam UK, Dhole TN. Neurological manifestations of dengue virus infection. J Neurol Sci. 2006;244:117–22. doi: 10.1016/j.jns.2006.01.011. [DOI] [PubMed] [Google Scholar]
- 3.Kamble R, Peruvamba JN, Kovoor J, Ravishankar S, Kolar BS. Bilateral thalamic involvement in dengue infection. Neurol India. 2007;55:418–9. doi: 10.4103/0028-3886.37103. [DOI] [PubMed] [Google Scholar]
- 4.Yeo PS, Pinheiro L, Tong P, Lim PL, Sitoh YY. Hippocampal involvement in dengue fever. Singapore Med J. 2005;46:647–50. [PubMed] [Google Scholar]
- 5.Mathew T, Badachi S, Sarma GR, Nadig R. “Boomerang sign in rickettsial encephalitis. Neurol India. 2014;62:336–8. doi: 10.4103/0028-3886.137030. [DOI] [PubMed] [Google Scholar]
- 6.Tada H, Takanashi J, Barkovich AJ, Oba H, Maeda M, Tsukahara H, et al. Clinically mild encephalitis/encephalopathy with a reversible splenial lesion. Neurology. 2004;63:1854–8. doi: 10.1212/01.wnl.0000144274.12174.cb. [DOI] [PubMed] [Google Scholar]