

Abstract
Objective
To examine the longitudinal association between sedentary behaviors and risk of developing depressive symptoms.
Patients and Methods
1012 women and 3790 men (18–80 yr) not reporting depressive moods completed a health survey during 1982 when they reported their time spent watching television (TV) and riding in a car each week. All participants completed a follow-up health survey when they responded to the 10-item Center for Epidemiologic Studies Depression Scale (CES-D 10). Those who scored 8 or more on the CES-D 10 were considered to have depressive symptoms.
Results
568 participants reported depressive symptoms during an average follow-up of 9.3 years. After multivariate-adjustment including moderate- and vigorous- intensity physical activity (MVPA), time in riding in a car, watching TV and combined time spent in the two sedentary behaviors were positively (P trend <.05 for each) associated with depressive symptoms. Individuals who reported ≥9 hrs/wk riding in a car, >10 hrs/wk watching TV, or ≥19 hrs/wk of combined sedentary behavior had 28%, 52%, and 74% greater risk of developing depressive symptoms than those who reported <5 hrs/wk, <5 hrs/wk, or <12 hrs/wk, respectively after adjusting for baseline covariates and MVPA. The positive association between time in riding in a car or time in watching TV and depressive symptoms was only observed among individual who did not meet the current PA guidelines.
Conclusion
Longer time reported in these two sedentary behaviors was positively associated with depressive symptoms. The direct associations between time spent in car riding and TV viewing, with depressive symptoms, were however only significant among those who did not meet the current PA recommendation.
INTRODUCTION
During the past ten years, sedentary behavior, defined as behavior characterized by a seated or reclining posture and low energy expenditure (≤1.5 MET) during waking hours1, 2, has emerged and been recognized as an important risk factor for negative health impacts that is different and distinct from physical activity (PA)3–5. The evidence is growing from observational and experimental studies that supports a direct link between sedentary behavior and poor physical health outcomes, including mortality due to all causes, cardiovascular diseases (CVDs), and cancer, obesity, hypertension, diabetes, and metabolic health6, 7. The World Health Organization and several other countries are starting to provide recommendations in regard to limiting sedentary time, in youth and adults8–10.
However, the prospective association between sustained sedentary behavior and mental health outcomes is unclear7, 11. There are four longitudinal investigations of the associations12–15 between sedentary behaviors and depressive disorders/moods. One of the longitudinal studies13 created a sedentary index by combining television (TV) viewing and computer use, which makes the interpretation difficult because internet use per se and sitting time alone are confounded. A recent study by Hamer et al reported a beneficial effect of internet use on depressive symptoms in a group of older adults14. This recent study further supports the hypothesis that different types of sedentary behavior may influence human health differently11, 16. The other three longitudinal studies have examined TV viewing with a depression-related outcome, but focused exclusively on the one aspect of sedentary behavior. An important dimension of sedentary behavior was not considered in these analyses; none of these studies evaluated the role of time spent in car riding in the development of depressive symptoms12, 14, 15. According to the 2009 National Household Travel Survey data, the average American now spends almost one hour per day traveling by car, not including long road trips17, and thus time spent sitting in the car may be an important sedentary behavior parameter that merits consideration.
In addition, the influence or the interaction of PA on the association between sedentary behavior and depression risk is controversial. The presence of a significant interaction indicates that the mechanism through which sedentary behavior impacts depression may be different in people who are active from people who are inactive. Very few studies have investigated this issue; some studies have reported no interaction18, 19, whereas others have observed an interaction13, 20 between sedentary behavior, PA and depression risk. Therefore, careful consideration of an interaction with PA is warranted as a more detailed analysis of sedentary behaviors is evaluated in association with risk of depressive symptoms.
Considering the increased disease burden of depressive disorders worldwide21, identifying modifiable factors to prevent depression is becoming an important public health issue. Therefore, the aim of this study was to examine the association between two types of sedentary behaviors (TV viewing and car riding) and the risk of developing depressive symptoms over twenty years of follow-up among a group of men and women enrolled in the Aerobics Center Longitudinal Study (ACLS). A second aim was to explore if or how PA modified the association between sedentary behaviors and depressive symptoms.
METHODS
Aerobics Center Longitudinal Study
The ACLS is a prospective study of men and women who have been examined at the Cooper Clinic in Dallas, TX22, 23. These patients came to the clinic for periodic preventive medical examinations and for counseling regarding health and lifestyle behavior factors. Patients came from all 50 states; most were self-referred with some referred by their physicians or employers. At the time of their clinic examination, the ACLS was described to patients who then provided written informed consent for enrollment in the follow-up study. Starting in 1982, mail surveys were administered every 4–5 years until 2004 to collect additional information. The Cooper Institute Institutional Review Board annually reviewed and approved the study protocol.
Study population
For the purposes of the present analyses, data from participants who responded to the 1982 survey were used as the baseline measure because this was the first time that information on sedentary behaviors was collected. A total of 11,972 participants returned the 1982 survey with a 77% response rate22. We excluded 1,830 individuals who met the following criteria: myocardial infarction or coronary bypass operation (n=560), stroke (n=43), cancer (n=476), often depressed or generally sad (n=406), age<18 or age>100 (n=345). Among the eligible participants, 4,802 individuals completed the 10-item Center for Epidemiological Studies Depression Scale (CES-D 10) during 1990–2005, and therefore became the final analytical sample for the current study.
Sedentary behaviors
During the 1982 survey, participants were asked to recall their average time (in hours) viewing TV and riding in a car during each week. Weekly TV time, car riding time, and combined time in these two behaviors were categorized into three roughly equal groups rounded up to the nearest hour. The associated times were <5, 5–8.9, and ≥9 hours/week for TV viewing, <5, 5–10, and >10 hours/week for car riding, and <12, 12–18.9 and ≥19 hours/week for the combined behaviors, respectively. We have used a similar approach in a previous report22.
Depressive symptoms
Depressive symptoms were assessed after the baseline visit using the CES-D 10, between 1990 and 2005. Participants were asked to respond to ten items by providing a 4-point ordinal scale answer from “less than 1 day” to “5–7 days”. Eight of the ten CES-D items assessed different aspects of depressed mood, while the remaining two (reverse scored) items assessed a more hopeful, happy mood state. The CES-D 10 has been validated with good reliability in general populations24–26. Although the CES-D is a screening measure rather than a diagnostic tool, a score of ≥8 on the CES-D 10 (which corresponds to a cutoff of 16 on the 20-item CES-D) is considered to indicate the presence of elevated depressive symptoms26.
Baseline measures
Demographic, socioeconomic status, and health-related questions included age (in years), gender (female/male), race (black, white, other), education (high school or less, some college, college graduate, master’s degree, doctoral degree), marital status (never married, married, separated, divorced, widowed), employment status (working, retired, unemployed, keeping house, student), presence of hypertension and diabetes. PA was assessed by questions asking the participant to report their total time spent doing moderate and vigorous PA (MVPA) during the last seven days. Meeting the current PA recommendation was defined as total time ≥2.5 hours and those who performed less than 2.5 hours of MVPA were classified as not meeting the current PA recommendation. MVPA was further classified into three groups: <2.5, 2.5–4.9, and ≥5 hours/wk. Other covariates included smoking (current smoker or not), alcohol intake, and body mass index (BMI). Heavy drinkers were defined as drinks per week >14 in men or >7 in women. One drink of alcohol equals 12 oz (3.41 dL) of beer, 5 oz (1.42 dL) of wine, or 1.5 oz (0.4262 dL) of hard liquor. BMI was calculated from measured height and weight in accordance with standard procedures during participants’ clinical visit. Cardiorespiratory fitness (CRF) was assessed using a maximal treadmill exercise test27.
Statistical analysis
Analyses were conducted in 2014 using SAS, version 9.3, with alpha set at P<.05. Baseline characteristics of the study population were characterized by depressive symptoms status (developed depressive symptoms/did not develop depressive symptoms). Differences in covariates were tested using Student t-tests and chi-square tests. Logistic regression models were used to examine the association between sedentary behavior and risk of developing depressive symptoms. Odds Ratios (ORs) and 95% confidence intervals (CIs) were reported as an index of the strength of association. Three models were tested: 1) age and sex-adjusted model; 2) multivariate-adjusted model including the following covariates: age (in years), gender, high school or less education (yes/no), marital status (currently married or not), employment status (currently working or not), current smokers (yes/no), BMI (in kg/m2), and diabetes (yes/no); and 3) multivariate plus MVPA (in hours/week) model. We assessed linear trends in the association of sedentary behavior with the risk of depressive symptoms. We then performed stratified analyses across MVPA groups to assess whether MVPA modified the association between sedentary behavior and depressive symptoms. Finally, we conducted additional analysis by adjusting for CRF in model 3 in a subgroup of participants with available CRF data (n=4709) because CRF is an objective indicator of habitual PA28. Because the magnitude of the associations from these analyses was very similar to the main findings reported by adjusting for self-reported MVPA, we do not report them in this manuscript. Please see the web appendix (Supplemental tables S1 and S2).
RESULTS
Characteristics of the study population are presented in Table 1. Over the average follow-up period of 9.3 years, 568/4802 individuals (12%) developed depressive symptoms. Participants who developed depressive symptoms were younger, female, not currently married, and reported longer time spending in riding in a car, watching TV, and combined sedentary behaviors.
TABLE 1.
Baseline characteristics of study participants by depressive symptoms during follow-up.
| Characteristic | All (N=4802) | Participants Who Did Not Develop Depressive Symptoms (n=4234), mean (SD) or n (%) | Participants Who Developed Depressive Symptoms (n=568), mean (SD) or n (%) | P Value |
|---|---|---|---|---|
| Age (yr) | 48.4 (9.8) | 48.5 (9.7) | 47.5 (10.1) | .02 |
| Female (%) | 1012 (21.1) | 851 (20.1) | 161 (28.4) | <.001 |
| Black (%) | 20 (0.4) | 18 (0.4) | 2 (0.4) | .99 |
| High school or less education (%) | 262 (5.5) | 226 (5.3) | 36 (6.3) | .32 |
| Currently married (%) | 4274 (89.0) | 3784 (89.4) | 490 (86.3) | .03 |
| Currently working (%) | 3947 (82.2) | 3510 (82.9) | 437 (76.9) | <.001 |
| Body mass index (kg/m2) | 24.6 (3.4) | 24.6 (3.3) | 24.9 (3.8) | .07 |
| Physical activitya (hours in the last seven days) | 6.2 (7.3) | 6.3 (7.3) | 5.7 (7.1) | .07 |
| Sedentary behaviors (h.wk−1) | ||||
| Riding in a car | 8.0 (6.0) | 7.9 (5.9) | 8.8 (6.9) | .002 |
| Watching TV | 9.0 (7.3) | 8.9 (7.2) | 9.9 (7.7) | .002 |
| Combined sedentary behaviors | 17.0 (10.0) | 16.7 (9.9) | 18.7 (10.5) | <.001 |
| Current smoker (%) | 379 (7.9) | 324 (7.7) | 55 (9.7) | .09 |
| Heavy alcohol drinkerb (%) | 717 (14.9) | 628 (14.8) | 89 (15.7) | .60 |
| Hypertension (%) | 829 (17.3) | 728 (17.2) | 101 (17.8) | .73 |
| Diabetes (%) | 93 (1.9) | 78 (1.8) | 15 (2.6) | .19 |
Abbreviation: SD=standard deviation.
Physical activity was defined as the total hours of moderate and vigorous physical activity reported during the past seven days.
Heavy alcohol drinker was defined as drinks per week >14 in male or >7 in female. One drink of alcohol is defined as 12 oz (3.41 dL) of beer, 5 oz (1.421 dL) of wine, or 1.5 oz (0.4262 dL) of hard liquor.
Table 2 presents the association between sedentary behaviors and risk of depressive symptoms. Time spent riding in a car, watching TV, and combined behaviors was each associated with developing depressive symptoms. Participants who rode in a car ≥9 hours/week had a 27% greater risk of developing depressive symptoms than those with a car riding time <5 hours/week after adjusting for age, gender, education, marital status, employment status, current smoker, BMI, and diabetes (P trend =.03). Additional adjustment for MVPA did not materially change the above observed association. Participants who watched TV >10 hours/week had a 42% higher risk of developing depressive symptoms than those who watched less than 5 hours/week after multivariate adjustment of the above factors (P trend =.003). Additional adjustment for MVPA showed a 35% higher risk of developing depressive symptoms for individuals who watched 5–10 hours/week, and a 52% higher risk for those who watched more than 10 hours/week, respectively. After combining the reported hours of car riding and TV watching, participants who reported 12–18.9 hours/week and ≥19 hours/week of sedentary behavior had a 35% and 74% greater risk of developing depressive symptoms compared with those who reported <12 hours/week, respectively, even after adjusting MVPA (P trend<.001).
TABLE 2.
Odds ratios (95% confidence intervals) of depressive symptoms according to tertiles of sedentary behaviors
| Tertiles of Sedentary Behaviors
|
||||
|---|---|---|---|---|
| 1 (Low) | 2 (Middle) | 3 (Upper) | P for linear trend | |
| Riding in a car (h/wk) | ||||
| Range | <5 | 5–8.9 | >9 | |
| Cases (N)a | 163 | 185 | 220 | |
| Total (N) | 1515 | 1648 | 1639 | |
| Age and sex- adjusted OR (95% CI) | 1 | 1.05 (0.84–1.31) | 1.30 (1.05–1.62) | .02 |
| Multivariate OR (95% CI)b | 1 | 1.05 (0.84–1.32) | 1.27 (1.02–1.59) | .03 |
| Multivariate + MVPA OR (95% CI)c | 1 | 1.02 (0.81–1.29) | 1.28 (1.02–1.61) | .03 |
| Watching TV (h/wk) | ||||
| Range | <5 | 5–10 | >10 | |
| Cases (N)a | 147 | 224 | 197 | |
| Total (N) | 1481 | 1892 | 1429 | |
| Age and sex- adjusted OR (95% CI) | 1 | 1.24 (1.00–1.55) | 1.47 (1.17–1.85) | <.001 |
| Multivariate OR (95% CI)b | 1 | 1.24 (0.99–1.54) | 1.42 (1.13–1.80) | .003 |
| Multivariate + MVPA OR (95% CI)c | 1 | 1.35 (1.07–1.71) | 1.52 (1.19–1.95) | <.001 |
| Combined sedentary behavior (h/wk) | ||||
| Range | <12 | 12–18.9 | >19 | |
| Cases (N)a | 143 | 179 | 246 | |
| Total (N) | 1563 | 1523 | 1716 | |
| Age and sex- adjusted OR (95% CI) | 1 | 1.33 (1.05–1.68) | 1.69 (1.35–2.10) | <.001 |
| Multivariate OR (95% CI)b | 1 | 1.31 (1.04–1.66) | 1.63 (1.31–2.04) | <.001 |
| Multivariate + MVPA OR (95% CI)c | 1 | 1.35 (1.06–1.72) | 1.74 (1.38–2.19) | <.001 |
Abbreviation: OR= odds ratio; CI=confidence interval; MVPA=moderate and vigorous physical activity.
Cases referred to participants who developed depressive symptoms.
Adjusted for age, gender, education, marital status, employment status, current smoker, body mass index, and diabetes.
Adjusted for age, gender, education, marital status, employment status, current smoker, body mass index, diabetes, and MVPA (hours/week).
We next examined the relationship between each sedentary behavior variable and depressive symptoms representing hours/week as a continuous exposure (Figure 1). Multivariate-adjusted OR and 95% CI associated with each 1 hour increment was 1.024 (1.01–1.039, P<.001) for car riding, 1.017 (1.005–1.029, P=.005) for TV viewing, and 1.018 (1.009–1.026, P<.001) for the combined behaviors, respectively. Additionally adjusting for MVPA did not significantly affect the above association. The associated OR and 95% CI for each 1 hour increment was 1.023 (1.01–1.037, P<.001) for car riding, 1.016 (1.004–1.027, P=.007) for TV viewing, and 1.017 (1.009–1.025, P<.001) for the combined behaviors, respectively.
FIGURE 1.
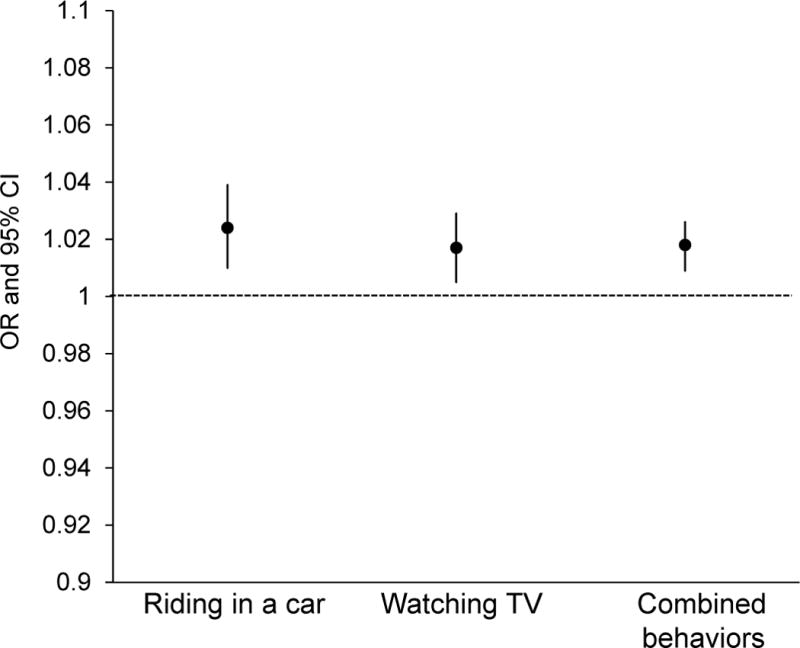
Multivariate*-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of depressive symptoms associated with 1 hour increase in time spent in sedentary behavior. *Adjusted by age, gender, education, marital status, employment status, current smoker, body mass index, and diabetes.
We then examined whether MVPA modified the association between sedentary behavior and depressive symptoms (Figure 2). Multivariate-adjusted analyses showed a positive association between time spent riding in a car (upper panel), and watching TV (middle panel) and the risk of developing depressive symptoms only among participants who did not meet the current PA recommendation. However, a positive linear trend was observed between longer hours of combined behaviors and higher risk of developing depressive symptoms not only among those who did not meet the current PA recommendation (P trend<.001), but also among individuals who met the recommendation (P trend=.01) (lower panel). Further analyses across three groups of MVPA showed similar patterns of positive associations between time spent in the combined sedentary behaviors and depressive symptoms in each MVPA category (all P trend<.05) (Figure 3).
FIGURE 2.
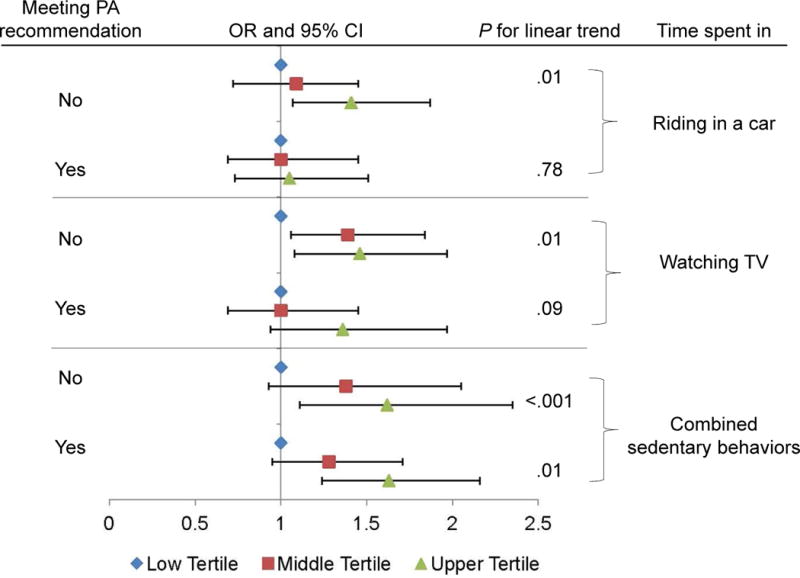
Multivariate*-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of depressive symptoms by tertiles of time spent in riding in a car, watching TV, and in combined sedentary behaviors across meeting and not meeting physical activity (PA) recommendation groups. *Adjusted by age, gender, education, marital status, employment status, current smoker, body mass index, and diabetes. Low tertile is the referent.
FIGURE 3.
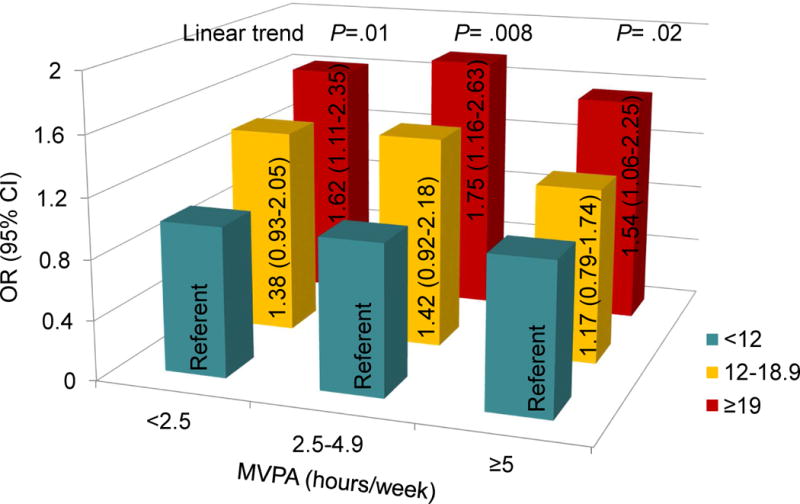
Multivariate*-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of depressive symptoms by tertiles of time spent in combined sedentary behaviors across moderate and vigorous physical activity (MVPA) groups. *Adjusted by age, gender, education, marital status, employment status, current smoker, body mass index, and diabetes.
DISCUSSION
Key study findings
Longer time spent in riding in a car, viewing TV, and the combined behaviors were associated with higher risk of developing depressive symptoms over an average period of 9.3 years, and these associations remained significant, after adjustment for other covariates, including MVPA. Participants who rode in a car ≥9 hours/week, watched TV>10 hours/week, or reported a combination of these behaviors ≥19 hours/week had a 28%, 42%, and 52% higher risk of developing depressive symptoms compared with those who reported <5 hours/week of car riding, <5 hours of TV viewing, or <12 hours of combined behaviors, respectively. Adjusting for CRF in stead of MVPA showed a clear attenuation of the associations between the two sedentary behaviors and depressive symptoms although the degree of attenuation was small (Supplemental Table S2). A clear dose-response relationship was observed for TV viewing and the combined sedentary behaviors. The longer time spent in these two sedentary behaviors, the higher the risk of depressive symptoms (Table 2). In addition, MVPA played a major role in buffering the association between car riding and TV viewing and future depressive symptoms. For participants who met the current PA recommendation, no significant association was observed between car riding and TV viewing and depressive symptoms, however, for those who did not meet the recommendation, there was a clear positive linear trend across the tertiles of time spent in car riding and TV viewing with depressive symptoms (Figure 2). However, with the prolonged combined sedentary behaviors (≥19 hours/week), MVPA did not appear to reduce the risk of developing depressive symptoms. The significant higher risk of developing depressive symptoms was observed among participants who spent 19 or more hours/week of combined sedentary behaviors regardless their MVPA levels (Figure 3). To our knowledge, this is the first longitudinal study to demonstrate a direct association between two popular sedentary behaviors, riding in a car and watching TV, and risk of developing depressive symptoms. The present data not only confirm previous work12–15, 18–20, 29–31 but also expand the existing literature by showing an adverse association of car riding with depressive symptoms.
Comparison with the existing literature
There is substantial evidence of the role of PA (e.g., MVPA) in reducing the risk of non-clinical depressive symptoms and clinical depression in adults32, 33. Additionally, PA and formal exercise training have been associated with significant reductions in depression and depression-related mortality in patients with coronary heart disease and heart failure34–36. Even with the rapidly expanding literature on sedentary behavior and health outcomes during the past decade6, much less research has been conducted on the effect of sedentary behavior on mental health outcomes11. Until now, the role of sedentary behaviors on the development of depressed mood has been evaluated in only ten studies, including 6 cross-sectional18–20, 29–31 and 4 longitudinal reports12–15. The cross-sectional studies all suggested a positive association between excessive sitting time, mostly screen-based behaviors18, 19, 30, 31 or total sedentary behaviors20, 29, and depressive moods. However, two cross-sectional studies did not demonstrate any association between TV viewing and depressive moods18, 31. On the other hand, Dittmar and colleagues reported a direct association between TV viewing and depressive symptoms among a group of college students30. The inconsistent findings from these cross-sectional studies might be due to the nature of the study design and other factors such as the different definitions and classifications of the sedentary behavior exposure, different study populations, and the various depression outcomes assessed, or a combination of these factors.
During the past several years, longitudinal studies have provided some evidence on the association between sedentary behaviors and risk of developing depression12, 13, 15 or elevated depressive symptoms14, 15. TV viewing and screen time have been shown to be positively associated with incident depression in two reports from the Nurses’ Health Study12, 15. Lucas and colleagues reported a 19% higher risk of clinical depression among women who spent 21 or more hours weekly watching TV than those with less than 2 hours12. In the English Longitudinal Study of Ageing (ELSA), longer time spent viewing TV (≥6 hours/day) was associated with higher depressive symptoms scores during a 2-year follow-up, compared with those who watched TV less than 6 hours/day14. However, the Seguimiento University of Navarra (SUN) Cohort Study did not find any association between a sedentary index (watching TV or/and using the computer) and depression incidence (OR for the highest level of the sedentary index=1.35; 95% CI=0.94,1.94; P for trend=.27)13. This nonsignificant finding is likely due to the small number of depression events because they did report a significant association between sedentary index and metal disorders overall (OR for the highest level of the sedentary index=1.31; 95% CI=1.01,1.68; P for trend=.04). We found a 2% higher risk of depressive symptoms for each additional hour spent in watching TV over a 20-year follow-up (Figure 1). In addition, participants had a 52% higher risk of depressive symptoms when they watched TV for more than 10 hours per week, compared with those who reported watching less than 5 hours, and these associations were independent of MVPA (Table 2).
Whether PA influences the association between sedentary behavior and depressive moods is controversial, as few studies have investigated this issue; some studies have indicated no interaction18, 19, while others have suggested an interaction13, 20 between sedentary behavior and PA with depressive moods. The SUN Cohort Study found a reduced sedentary index to be an important correlate of reduced risk of mental disorder (depression was part of the outcome measure, along with stress and anxiety) when PA levels were low, however, it was not associated with the outcome when PA levels were high13. A recent study from the Australian Longitudinal Study on Women’s Health (ALSWH) reported a three-fold higher likelihood of depressive symptoms in mid-aged women who sat >7 hours/day and did no PA, compared with those who sat ≤4 hours/day and met PA guidelines20. As in the current study, the higher risk associated with longer time spent in car riding (Figure 2, upper panel), and TV viewing (Figure 2, middle panel) was only observed in participants who did not meet the current PA recommendation. It is noteworthy that when combined sedentary behavior was analyzed as the exposure, the positive linear trend across tertiles of this exposure persisted, regardless of MVPA level (Figures 2, lower panel and 3). This unique finding may indicate that the deleterious effect of very high levels of sedentary behaviors might not be offset by meeting PA guidelines. However, our results showed that levels of PA consistent with the upper range of current guidelines (≥5 hours each week), seemed to attenuate the sitting/depression relationship (Figure 3). Future studies are warranted to identify intervention strategies to reduce high levels of sedentary behaviors while continuing to promote PA.
Few studies have examined the association between car riding and depressive symptoms. In some studies, participants are asked to report time in several sitting contexts, such as visiting friends, driving, reading, watching TV or working at a desk or computer, but only generic estimates of sitting time are included in this analysis20. Therefore, we believe that our study is the first to establish a link between time spent riding in a car and depressive symptoms. We found that each additional hour spent in the car was associated with a 2% higher risk of depressive symptoms (Figure 1) and participant who reported riding in a car ≥9 hours per week had a 28% higher risk of developing depressive symptoms, compared with those who spent less than 5 hours per week riding in a car (Table 2). Future studies will need to confirm or reject our findings.
Potential mechanisms linking sedentary behavior and depression
The underlying mechanisms explaining the associations between sedentary behavior and risk of depression are still not clear. Several hypotheses have been proposed, such as withdrawal, social isolation, or displacement hypotheses. The withdrawal hypothesis suggests that the excessive sedentary behaviors such as TV viewing or computer/internet use take individuals away from social interaction, which can increase risk of depression37. In fact, existing studies have consistently reported a positive association between TV viewing and depression11. However, a recent study using the ELSA data demonstrated an inverse association of internet use and newspaper reading with depressive symptoms14. Another study also showed that using the internet/computer decreased the risk of depression38. Therefore, other biological or psychological mechanisms might be identified to explain the link between different types of sedentary behaviors and depression risk. The displacement hypothesis suggests that sedentary behaviors might displace PA, and therefore could lead to a higher risk of depression. The beneficial effects of PA on depression have been established32 and strengthened by biological changes from experiment studies39.
Study strengths and limitations
The strengths of the current study include a relatively large sample of adult men and women from a well-established cohort, with over 20-year follow-up, and measures of two popular sedentary behaviors of TV viewing and car riding. In fact, to our knowledge, this is the first study showing a direct link between prolonged car riding and risk of developing depressive symptoms.
Several limitations are acknowledged. Firstly, the ACLS population may not be totally representative of US population, as the majority of the participants were non-Hispanic whites, well-educated, non-overweight, and with middle-to-high socioeconomic status. A small percentage of women limited our ability to conduct gender-specific analysis. Secondly, both sedentary behaviors and MVPA were assessed by self-report. We acknowledge that such measurement has inherent weaknesses including recall bias and social desirability. Thirdly, the observed effect modification from MVPA should be interpreted cautiously due to the likelihood of insufficient statistical power. Fourthly, we are not able to assess changes in sitting time that occurred during the long follow-up period. Some participants might have changed their TV and/or car riding time. Fifthly, depressive disorders are often episodic so it is possible that elevated depressive symptoms might be missed due to the timing of the follow-up. A final consideration is the behavioral manifestations of depressive disorders (lack of energy, psychomotor retardation, insomnia, and anhedonia) may well predispose individuals to engage in longer periods of sedentary behaviors like watching TV than the same individual might engage in when not clinically depressed. Because CES-D 10 data were not available at baseline, those who reported often depressed or generally sad at baseline were excluded due to their previous mental health concerns. Thus, it is possible that some individuals with high depressive symptoms at baseline may have been inadvertently included in analyses (because they did not report being “often depressed” or “generally sad”). Therefore, reverse causation where high depressive symptoms caused an increase in TV time and car riding time cannot be entirely ruled out. In fact, Hamer and colleagues had reported that at baseline, longer time spent viewing TV was associated with higher depressive symptoms scores14. Future studies with adequate sample size are needed that incorporate changes in both exposure and covariates when studying the association between sedentary behaviors and depressive symptoms as well as examine other diverse samples, and the use of objective measurements to assess sedentary behaviors and PA.
Conclusion
The findings are consistent with and extend those of previous research which indicates that sedentary behaviors may be risk factors for depressive symptoms. However, MVPA appears to partially reduce the negative effects of prolonged sedentary behaviors on depressive symptoms. These results, therefore, suggested that sedentary behavior and MVPA are implicated in the development of depressive symptoms. This study findings support the need for interventions which will reduce these two sedentary behaviors and increase MVPA to improve this health outcome in adult populations.
Supplementary Material
Acknowledgments
Sources of Funding
This work was supported by National Institutes of Health grants AG06945, HL62508, and DK088195. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
LIST OF ABBREVIATIONS
- ACLS
Aerobics Center Longitudinal Study
- ALSWH
Australian Longitudinal Study on Women’s Health
- BMI
body mass index
- CES-D
Center for Epidemiologic Studies Depression Scale
- CI
confidence interval
- CRF
cardiorespiratory fitness
- CVD
cardiovascular disease
- ELSA
English Longitudinal Study of Ageing
- OR
odds ratio
- MET
metabolic equivalent
- MVPA
moderate and vigorous physical activity
- SUN Cohort Study
Seguimiento University of Navarra Cohort Study
- TV
television
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosures
None.
Competing interests: none.
Reference List
- 1.Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O’Brien WL, Bassett DRJ, Schmitz KH, Emplaincourt PO, Jacobs DRJ, Leon AS. Compendium of physical activities: An update of activity codes and MET intensities. Med Sci Sports Exerc. 2000 Sep;32(9 Suppl):S498–S516. doi: 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- 2.Pate RR, O’Neill JR, Lobelo F. The evolving definition of “sedentary”. Exerc Sport Sci Rev. 2008 Oct;36(4):173–8. doi: 10.1097/JES.0b013e3181877d1a. [DOI] [PubMed] [Google Scholar]
- 3.Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010 Dec;35(6):725–40. doi: 10.1139/H10-079. [DOI] [PubMed] [Google Scholar]
- 4.Hamilton MT, Hamilton DG, Zderic TW. Exercise physiology versus inactivity physiology: an essential concept for understanding lipoprotein lipase regulation. Exerc Sport Sci Rev. 2004 Oct;32(4):161–6. doi: 10.1097/00003677-200410000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dunstan DW, Kingwell BA, Larsen R, Healy GN, Cerin E, Hamilton MT, Shaw JE, Bertovic DA, Zimmet PZ, Salmon J, Owen N. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. 2012 May;35(5):976–83. doi: 10.2337/dc11-1931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Proper KI, Singh AS, van MW, Chinapaw MJ. Sedentary behaviors and health outcomes among adults: a systematic review of prospective studies. Am J Prev Med. 2011 Feb;40(2):174–82. doi: 10.1016/j.amepre.2010.10.015. [DOI] [PubMed] [Google Scholar]
- 7.Thorp AA, Owen N, Neuhaus M, Dunstan DW. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996–2011. Am J Prev Med. 2011 Aug;41(2):207–15. doi: 10.1016/j.amepre.2011.05.004. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. Global Recommendations on Physical Activity for health. 2010 [PubMed] [Google Scholar]
- 9.UK Department of Health, Physical Activity, Health Improvement and Protection. Start Active, Stay Active: a report on physical activity for health from the four home countries’ chief medical officers. London, UK: Department of Health; 2011. [Google Scholar]
- 10.Brown WJ, Bauman AE, Bull FC, Burton NW. Report prepared for the Australian Government Department of Health. Australian Government Department of Health; 2012. Development of evidence-based physical activity recommendations for adults (18–64 years) ( http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines/$File/DEB-PAR-Adults-18–64years.pdf) [Google Scholar]
- 11.Teychenne M, Ball K, Salmon J. Sedentary behavior and depression among adults: a review. Int J Behav Med. 2010 Dec;17(4):246–54. doi: 10.1007/s12529-010-9075-z. [DOI] [PubMed] [Google Scholar]
- 12.Lucas M, Mekary R, Pan A, Mirzaei F, O’Reilly EJ, Willett WC, Koenen K, Okereke OI, Ascherio A. Relation between clinical depression risk and physical activity and time spent watching television in older women: a 10-year prospective follow-up study. Am J Epidemiol. 2011 Nov 1;174(9):1017–27. doi: 10.1093/aje/kwr218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sanchez-Villegas A, Ara I, Guillen-Grima F, Bes-Rastrollo M, Varo-Cenarruzabeitia JJ, Martinez-Gonzalez MA. Physical activity, sedentary index, and mental disorders in the SUN cohort study. Med Sci Sports Exerc. 2008 May;40(5):827–34. doi: 10.1249/MSS.0b013e31816348b9. [DOI] [PubMed] [Google Scholar]
- 14.Hamer M, Stamatakis E. Prospective study of sedentary behavior, risk of depression, and cognitive impairment. Med Sci Sports Exerc. 2014;46(4):718–23. doi: 10.1249/MSS.0000000000000156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mekary RA, Lucas M, Pan A, Okereke OI, Willett WC, Hu FB, Ding EL. Isotemporal substitution analysis for physical activity, television watching, and risk of depression. Am J Epidemiol. 2013 Aug 1;178(3):474–83. doi: 10.1093/aje/kws590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Atkin AJ, Adams E, Bull FC, Biddle SJ. Non-occupational sitting and mental well-being in employed adults. Ann Behav Med. 2012 Apr;43(2):181–8. doi: 10.1007/s12160-011-9320-y. [DOI] [PubMed] [Google Scholar]
- 17.U.S. Department of Transportation. National Household Travel Survey. 2009 http://nhts.ornl.gov/2009/pub/stt.pdf. 2009.
- 18.Teychenne M, Ball K, Salmon J. Physical activity, sedentary behavior and depression among disadvantaged women. Health Educ Res. 2010 Aug;25(4):632–44. doi: 10.1093/her/cyq008. [DOI] [PubMed] [Google Scholar]
- 19.Breland JY, Fox AM, Horowitz CR. Screen time, physical activity and depression risk in minority women. Ment Health Phys Act. 2012;6(2013):10–5. doi: 10.1016/j.mhpa.2012.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.van Uffelen JG, van Gellecum YR, Burton NW, Peeters G, Heesch KC, Brown WJ. Sitting-time, physical activity, and depressive symptoms in mid-aged women. Am J Prev Med. 2013 Sep;45(3):276–81. doi: 10.1016/j.amepre.2013.04.009. [DOI] [PubMed] [Google Scholar]
- 21.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006 Nov;3(11):e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Warren TY, Barry V, Hooker SP, Sui X, Church TS, Blair SN. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010 May;42(5):879–85. doi: 10.1249/MSS.0b013e3181c3aa7e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Blair SN, Kohl HW, III, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality: a prospective study of healthy men and women. JAMA. 1989;262(17):2395–401. doi: 10.1001/jama.262.17.2395. [DOI] [PubMed] [Google Scholar]
- 24.Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psych Measurement. 1977;1:385–401. [Google Scholar]
- 25.Kohout FL, Berkman LF, Evans DA, Cornoni-Huntley J. Two shorter forms of the CES-D Depression Symptoms Index. J Aging Health. 1993;2:179–93. doi: 10.1177/089826439300500202. [DOI] [PubMed] [Google Scholar]
- 26.Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: Evaluation of a short form of the CES-D. Am J Prev Med. 1994;10(2):77–84. [PubMed] [Google Scholar]
- 27.Sui X, Laditka JN, Church TS, Hardin JW, Chase N, Davis K, Blair SN. Prospective study of cardiorespiratory fitness and depressive symptoms in women and men. J Psychiatr Res. 2009 Feb;43(5):546–52. doi: 10.1016/j.jpsychires.2008.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Haskell WL, Leon AS, Caspersen CJ, Froelicher VF, Hagberg JM, Harlan W, Holloszy JO, Regensteiner JG, Thompson PD, Washburn RA. Cardiovascular benefits and assessment of physical activity and physical fitness in adults. Med Sci Sports Exerc. 1992 Jun;24(6 Suppl):S201–S220. [PubMed] [Google Scholar]
- 29.Vallance JK, Winkler EA, Gardiner PA, Healy GN, Lynch BM, Owen N. Associations of objectively-assessed physical activity and sedentary time with depression: NHANES (2005–2006) Prev Med. 2011 Oct;53(4–5):284–8. doi: 10.1016/j.ypmed.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 30.Dittmar ML. Relations among depression, gender, and television viewing of college students. J Soc Behav Pers. 1994;9:317–28. [Google Scholar]
- 31.de WL, van SA, Lamers F, Cuijpers P, Penninx B. Are sedentary television watching and computer use behaviors associated with anxiety and depressive disorders? Psychiatry Res. 2011 Apr 30;186(2–3):239–43. doi: 10.1016/j.psychres.2010.07.003. [DOI] [PubMed] [Google Scholar]
- 32.Teychenne M, Ball K, Salmon J. Physical activity and likelihood of depression in adults: a review. Prev Med. 2008 May;46(5):397–411. doi: 10.1016/j.ypmed.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 33.Azar D, Ball K, Salmon J, Cleland V. Individual, social, and physical environmental correlates of physical activity among young women at risk of depression. J Phys Act Health. 2011 Jan;8(1):133–40. doi: 10.1123/jpah.8.1.133. [DOI] [PubMed] [Google Scholar]
- 34.Lavie CJ, Milani RV. Adverse psychological and coronary risk profiles in young patients with coronary artery disease and benefits of formal cardiac rehabilitation. Arch Intern Med. 2006 Sep 25;166(17):1878–83. doi: 10.1001/archinte.166.17.1878. [DOI] [PubMed] [Google Scholar]
- 35.Milani RV, Lavie CJ. Impact of cardiac rehabilitation on depression and its associated mortality. Am J Med. 2007 Sep;120(9):799–806. doi: 10.1016/j.amjmed.2007.03.026. [DOI] [PubMed] [Google Scholar]
- 36.Milani RV, Lavie CJ, Mehra MR, Ventura HO. Impact of exercise training and depression on survival in heart failure due to coronary heart disease. Am J Cardiol. 2011 Jan;107(1):64–8. doi: 10.1016/j.amjcard.2010.08.047. [DOI] [PubMed] [Google Scholar]
- 37.Kraut R, Patterson M, Lundmark V, Kiesler S, Mukopadhyay T, Scherlis W. Internet paradox. A social technology that reduces social involvement and psychological well-being? Am Psychol. 1998 Sep;53(9):1017–31. doi: 10.1037//0003-066x.53.9.1017. [DOI] [PubMed] [Google Scholar]
- 38.Shaw LH, Gant LM. Users divided? Exploring the gender gap in Internet use. Cyberpsychol Behav. 2002 Dec;5(6):517–27. doi: 10.1089/109493102321018150. [DOI] [PubMed] [Google Scholar]
- 39.Biddle SJH, Fox KR, Boutcher S. Physical activity and psychological well-being. London: Routledge; 2000. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.