

Abstract
The incidence of pulp canal obliteration following dental trauma has been reported to be approximately 4 – 24% and its management can be quite challenging for the practitioner. Locating the canal and negotiating it to full working length may lead to iatrogenic errors such as fractured instrument and perforation. This case report deals with such a case using the modified tip instrument technique to gain access and negotiate the canal to the apex followed by conventional root canal preparation and obturation.
Keywords: Pulp canal obliteration, Calcific metamorphosis, Management, Root Canal
Introduction
Dental trauma to the permanent dentition can lead to clinical complications such as Pulp Canal Obliteration and its management may considerably challenge a practitioner. This condition is also known as Calcific Metamorphosis (1) and is defined by the American Association of Endodontists (2) as “A pulpal response to trauma characterized by rapid deposition of hard tissue within the canal space.” This is more often observed in patients who have suffered concussion or subluxation injuries. (3) PCO is generally asymptomatic and clinically the patients present to the practitioner with yellow discoloration of the affected tooth crown. This discoloration is due to a greater thickness of dentine deposition. (4) The incidence of pulp canal obliteration following dental trauma has been reported to be approximately 4–24%. (5)
Case Report
A 46 year old Egyptian male came to the out-patient clinic at Qassim University with a desire to have his missing front tooth restored. The patient gave a history of trauma to the face a few years back which leads to fracture of tooth number 21 which was extracted. On examination, tooth number 11 was found to have a discolored crown. A radiograph of tooth number 11 (Figure 1) was taken which revealed that the canal could not be traced from the pulp chamber region until the middle third of the root where after the canal was visible.
Figure 1.
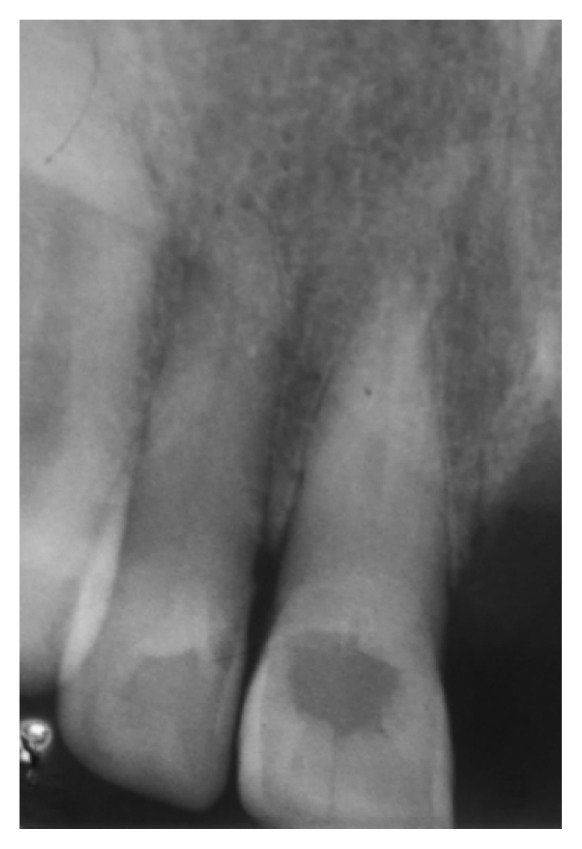
Upper right central incisor showing radiolucency in the crown region with absence of a chamber. The canal is visible from mid-root to the apical region
Since the missing tooth number 21 required replacement with a bridge, tooth number 11 was advised to undergo elective treatment endodontically for post placement. Tooth number 11 was diagnosed as Partial Pulp Canal Obliteration with no periapical involvement of bone radiographically. The floor of the cavity was initially cleared of caries and prepared using a low-speed tungsten carbide bur. On examination, a dark spot was seen on the floor which could have suggested the position of the canal orifice previously. Using this pigmented spot as a guideline, the tooth was entered using high-speed round No. 2 bur. The orientation of the access using high speed diamond bur was confirmed using radiographs to avoid perforation.
Due to unavailability of long shanked burs in our newly developed clinics, we were unable to go deeper and the radiograph showed around 3 – 4 mm of calcified dentine remaining till the canal could be negotiated. On clinical examination and trials, it was difficult to locate an orifice with an endodontic explorer. As an alternate method to gain further penetration in to the canal a 25 mm length #25 K-file was used by cutting 3 – 4 mm of its tip with the help of an orthodontic wire cutter. The file was used with reaming motion and apical pressure. Care was taken to keep the file aligned to the long axis of the tooth to avoid perforation. When a “drop” into a space was felt, a #8 K-file was introduced and a radiograph taken to confirm entry. After confirmation, rubber dam was applied and working length was determined using an apex locator and confirmed with a radiograph (Figure 2).
Figure 2.
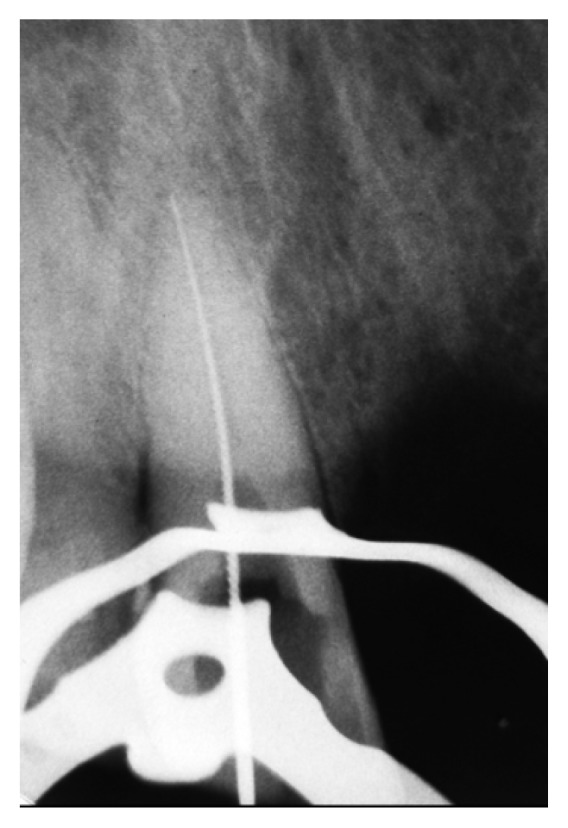
Radiograph confirming the working length
The canal was prepared using hand files with constant irrigation using 5.25% NaOCl. The canals were dried with paper points and finally obturated using the cold lateral condensation technique. The coronal access was restored with GIC [Ketac-Fil Plus Aplicap, 3M ESPE] (Figure 3). The patient was referred to the Department of Prosthdontics for treatment completion.
Figure 3.

Final obturation and GIC restoration of the coronal 3rd of root and crown portion
Discussion
The use of the modified file tip technique served purposeful in the management of this case. Numerous case reports and reviews mention a set protocol for the management of PCO. Root perforation, fractured instruments and root fracture due to excessive preparation to locate the canal are possible complications. (5)
Fachin et al. (6) described the “Modified-Tip Instrument” technique for removal of hard pastes from the root canal during retreatment and suggested its use to gain length in extremely calcified canals. The tip of a K-type file (quadrangular section), #30 and #35, is cut by 4 mm using an orthodontic wire cutter producing a sharp edge at the new working end. Used with an apical pressure and reaming motion this file now becomes an efficient and potent cutting instrument. However, a K-type file #25 was used here to avoid a larger defect such as a perforation or ledge in the event of a mishap, whilst maintaining stiffness to avoid bending of the file.
Conclusion
The modified file, in conjunction with good magnification, light and detailed knowledge of dental anatomy, can prove to be an effective, fast and easy alternative in gaining access and achieving full working length in an otherwise obliterated canal. The technique is potentially much less destructive of tooth tissue than the currently recommended alternatives.
References
- 1.Reis LC, Nascimento VDMA, Lenzi AR. Operative microscopy – indispensable resource for the treatment of pulp canal obliteration: a case report. Braz J Dent Traumatol. 2009;1(1):23–26. [Google Scholar]
- 2.Glossary of Endodontic Terms. 8th Ed. American Association of Endodontics; 2012. [Google Scholar]
- 3.Oginni AO, Adekoya-Sofowora CA. Pulpal sequelae after trauma to anterior teeth among adult Nigerian dental patients. BMC Oral Health. 2007;7:11. doi: 10.1186/1472-6831-7-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Munley PJ, Goodell GG. Calcific metamorphosis. Clinical Update for Naval Postgraduate Dental School. 2005;27(4) [Google Scholar]
- 5.McCabe PS, Dummer PMH. Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J. 2011;45:177–197. doi: 10.1111/j.1365-2591.2011.01963.x. [DOI] [PubMed] [Google Scholar]
- 6.Fachin EV, Wenckus CS, Aun CE. Retreatment using a modified-tip instrument. J Endod. 1995;21(8):425–8. doi: 10.1016/S0099-2399(06)80830-7. [DOI] [PubMed] [Google Scholar]