

Abstract
Objectives.
Social expectancy theory posits that cultural values shape how individuals perceive and evaluate others, and this influences how others evaluate themselves. Based on this theory, ageism may shape older individuals’ self-evaluations. Given the cultural focus on beauty and youth, perceptions of age discrimination may be associated with lower body esteem, and this may be associated with poor psychological well-being. Because discrimination has been associated with poor health, and perceptions of health can affect body perceptions, subjective health status may also contribute to lower body esteem.
Method.
These associations are assessed in a structural equation model for 244 African American and European American women in their early 60s.
Results.
Perceptions of age discrimination and body esteem were associated with lower psychological well-being for both ethnic groups. Body esteem partially mediated the association between age discrimination and psychological well-being among European American women but not among African American women.
Discussion.
Age-related discrimination is one source of psychological distress for older adults, though ageism’s associations with body esteem, health, and psychological well-being vary significantly for European American and African American women. Examining body perceptions and health in the contexts of ageism and ethnicity is necessary when considering the psychological well-being of older women.
Key Words: Age discrimination, Ageism, Body esteem, Ethnic differences, Psychological well-being, Subjective health.
Adults who appear to be old may receive differential (i.e., ageist) treatment compared with younger looking adults. The perception or evaluation of an individual based on age may, in turn, influence how that individual evaluates his or herself. Given the omnipresent cultural focus on appearance, particularly for women (Fredrickson & Roberts, 1997), and the association between beauty and youth (Garner, 1999), it is likely that increased awareness of negative evaluations or perceptions of older adults (i.e., ageism) may lead some women to evaluate themselves negatively, particularly in the domain of body image. Both ageism and low body esteem are independently associated with poor psychological well-being (Forman & Davis, 2005; Levy, 2001), yet these have not yet been integrated into the same model. Negative self-evaluation in the domain of body image may represent one way that perceptions of ageism affect psychological well-being.
Perceptions of an individual’s age may influence evaluations and judgments of that individual in a variety of domains and have the power to shape self-evaluations. Older adults who perceive aging negatively or are subjected to ageism may experience deleterious consequences. Discrimination (e.g., racism and sexism) has a significant effect on the health and psychological well-being of members of low-status groups who report these experiences (Branscombe, Schmitt, & Harvey, 1999; Schmitt, Branscombe, Kobrynowicz, & Owen, 2002). However, few studies have considered the effects of discrimination based on age (i.e., ageism) (Butler, 1969; Nelson, 2005). The majority of research on ageism has focused on factors that contribute to stereotyping and prejudices against the aged, and less attention has been given to the effect on the targets of discrimination (Nelson, 2005; Swim & Stangor, 1998), or how ageism may affect middle-aged adults transitioning into older age.
Ageism and Body Esteem
Like other social categories and identities, age conveys social meaning both to oneself and to others (Garstka, Schmitt, Branscombe, & Hummert, 2004), and age-based social categorization affects the impressions we form about others (Celejewski & Dion, 1998; Slotterback, 1996). Although younger individuals will eventually move into the higher status category of being adults, those who have reached late middle age may be aware of the stigma associated with getting older, and the transition into a lower status group may place some adults at risk for poor psychological well-being. Women may be particularly vulnerable to age discrimination due to gendered ageism (Antonucci, Blieszner, & Denmark, 2010)—that is, women are routinely judged based upon the appearance of their bodies, and mainstream beauty standards prescribe a youthful appearance (Chrisler & Ghiz, 1993; Garner, 1999; Peat, Peyerl, & Muehlenkamp, 2008). Because visible markers of aging such as wrinkles and gray hair often assign social value to individuals, ageism is grounded in the beauty standards that value the youthful presentation of the body (Hurd Clarke, Griffin, & Maliha, 2009).
Social expectancy theory posits that cultural values shape how individuals perceive and evaluate others and that this, in turn, influences how others evaluate themselves (Jackson, 2004). Jackson (2004) explained that social expectancy theorists have developed a set of hypotheses with regard to bodily appearance and attractiveness, and these hypotheses illustrate how cultural expectations can shape an individual’s self-perceptions. Specifically, these hypotheses state that there is consensual cultural agreement about who is considered attractive or unattractive, that there are expectations about those who are considered to be attractive or unattractive (i.e., stereotypes), that people behave differently toward those who are considered attractive and unattractive, that differential behavior toward attractive and unattractive people shapes how these individuals respond, and that these behavioral differences result in differences in the self-concept of those considered attractive or unattractive (Jackson, 2004).
Older women are culturally devalued, and older women’s bodies are judged harshly for showing signs of age (Garner, 1999). Based upon the tenets of social expectancy theory, it is possible that women who experience greater age discrimination may perceive that they are treated differently from others, potentially based upon assumptions made about their appearance and/or age. This differential treatment shapes how older women respond and may be responsible for observed differences in self-concept, including both body and health perceptions. That is, older women who are subjected to greater age discrimination may experience poorer health and lower body esteem. Consequently, women’s psychological well-being may be negatively affected by both ageist discrimination and low body esteem (see Figure 1).
Figure 1.
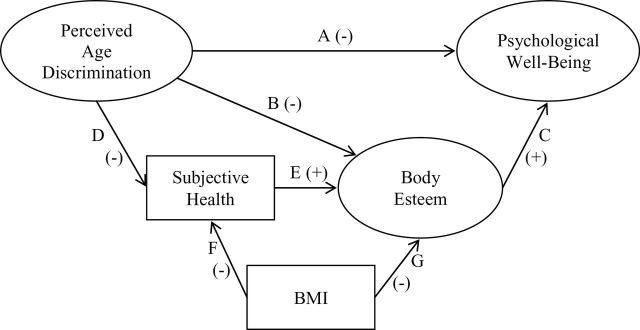
Proposed model combining perceptions of discrimination, body esteem, subjective health, and psychological well-being.
Discrimination and Psychological Well-Being
Perceptions of discrimination based on social identities, such as gender, ethnicity, and age, have been negatively associated with self-esteem and perceived locus of control and may lead individuals to hold negative expectations for the future (Schmitt & Branscombe, 2002). The association between experiencing discrimination and poor psychological well-being (i.e., depression, psychological distress, anxiety, and well-being) has been supported repeatedly (Paradies, 2006; Williams, Neighbors, & Jackson, 2003), and this pattern has been confirmed among members of low-status groups, such as women (Klonoff, Landrine, & Campbell, 2000; Schmitt et al., 2002), African Americans (Branscombe et al., 1999; Williams, Yu, Jackson, & Anderson, 1997), and lesbians and gay men (Herek, Gillis, & Cogan, 1999). Although the term ageism can refer to any discrimination based specifically on age, this most often refers to discrimination directed toward older adults (Nemmers, 2004). Little attention has been given to ageism and body image, despite that bodily signs of aging are often used as a means for determining who will be excluded (Calasanti, 2005).
Ageism has a profound effect on the psychological well-being of older adults. As predicted by social expectancy theory, exposure to ageism and negative stereotypes about aging throughout the life span may lead older adults to internalize this viewpoint and direct this prejudice inward (Levy, 2001). Internalized ageism has been associated with a plethora of negative outcomes, including lower life expectancy (Levy, Slade, Kunkel, & Kasl, 2002), impaired memory (Hess, Auman, Colcombe, & Rahhal, 2003), high blood pressure and heart rates (Levy, Hausdorff, Hencke, & Wei, 2000), and impaired motor skills, such as handwriting (Levy, 2000). Women in late middle age are transitioning into the category of older age and may be particularly aware of evaluation and judgments based on age. As a result, women who report greater age discrimination may also experience poorer psychological well-being.
Discrimination and Health
Discrimination may affect the body through its association with physical health. Perceptions of discrimination have been linked to a number of physical health problems, including hypertension and self-reported poor health, obesity, and substance abuse (Williams & Mohammed, 2009). One explanation for this association is that discrimination is a stressor that may trigger a series of physiological responses (such as high blood pressure, increased heart rate, and high levels of stress-related hormones) that, over time, affect health (Pascoe & Richman, 2009). Additionally, experiences of discrimination may affect health by lowering self-control responses, potentially increasing unhealthy behaviors and decreasing participation in healthy behaviors (Pascoe & Richman, 2009; Zucker & Landry, 2007) and impairing self-control (Inzlicht, McKay, & Aronson, 2006). Experiences of discrimination may leave fewer resources for making healthy decisions, and consequently older adults who report more ageism may be in poorer health.
Body Esteem and Mental Health
Beauty norms focus on youth, and normative aging is often associated with a loss of conventional beauty, making aging women susceptible to body image concerns (Peat et al., 2008). Because of the association between beauty and youth, women “lose their social value simply by growing old” (Garner, 1999, p. 4). The loss of perceived social value based on beauty norms is one facet of ageism and reinforces the idea that women are devalued as they age (Saucier, 2004; Sontag, 1972). As social expectancy theory posits, observing that older women are culturally devalued may cause women to view their own bodies in a negative manner.
Although some research has suggested that body dissatisfaction levels off after adolescence and remains relatively stable across the adult years (Tiggemann, 2004; Wilcox, 1997), a growing literature indicates that body dissatisfaction is prevalent among aging women (Bedford & Johnson, 2006; Lewis & Cachelin, 2001; Mangweth-Matzek et al., 2006; Szymanski & Henning, 2007). However, few studies have examined the impact of body esteem on mental health among aging women (Peat et al., 2008). Given that many midlife and older women demonstrate dissatisfaction with their bodies and with the cultural emphasis on beauty and youth, it is likely that low body esteem may be associated with poor psychological well-being for women in late middle age.
Health and Body Esteem
Feeling satisfied with one’s body may be strongly influenced by body functioning and health status; however, few researchers have considered the relationship between these constructs. Chrisler and Ghiz (1993) pointed out that medical research on aging bodies has focused primarily on the effects of chronic illness or surgery and has not considered satisfaction with or feelings about the body. The body undergoes physical changes with age, producing a changed physical reality for older adults (Rodin, Silberstein, & Striegel-Moore, 1984; Voda, Christy, & Morgan, 1991). The basal metabolic rate of the body slows with age, leading to a decrease in lean muscle tissue and an increase in fat (Rodin et al., 1984). Therefore, changes in body mass index (BMI) associated with age may affect body perceptions, and BMI needs to be assessed in conjunction with body image. Weight is often redistributed with age, resulting in a changing body shape (Voda et al., 1991). Changes in the body associated with menopause may serve as a risk factor for both body dissatisfaction and disordered eating (Gupta, 1990; Peat et al., 2008), and bodily changes due to postmenopause or aging may affect body perceptions.
Changes in physical health may also affect body esteem. Wilcox (1997) found that health evaluation (i.e., feeling that one is in good health) was positively related to appearance evaluation among a primarily White sample of men and women aged 20–80. Factors that influence health status (e.g., diet, exercise, presence of illness, and functional issues) are often directly related to body issues, and women who are in good health may hold more positive feelings about their bodies than do women in poor health.
This study
The goal of this study is to examine the associations between perceptions of age discrimination, body esteem, health, and psychological well-being among late middle-aged women. These constructs are of particular relevance for women in this age group; however, they have not previously been examined concurrently. Based upon prior research, I hypothesized that perceptions of age discrimination would have a negative association with psychological well-being, such that women who reported greater perceptions of age discrimination would also report lower psychological well-being (see Figure 1, path A). Based upon social expectancy theory, I hypothesized that greater perceptions of age discrimination would be associated with lower levels of body esteem (path B) and that this would then be associated with lower levels of psychological well-being (path C). That is, I hypothesized that body esteem would partially mediate the relationship between perceptions of age discrimination and psychological well-being.
I also hypothesized that perceptions of age discrimination would have a negative association with subjective health, such that women who reported greater perceptions of age discrimination would also report worse subjective health (path D). Additionally, I hypothesized that subjective health would have a positive association with body esteem, such that women who reported more positive health status would also report higher levels of body esteem (path E). Additionally, I added BMI into the model as a control variable (paths F and G). I investigated these relationships using structural equation modeling and tested alternate models to assess which model best fit the data.
Method
Participants and Procedure
Analyses presented are based on questionnaires administered through the mail to 244 University of Michigan alumnae in 2008. Participants were in their early 60s (average age = 63.44, standard deviation [SD] = 3.71). The sample included both European American (n = 158) and African American women (n = 79) who completed all questionnaires included in the current study. Participants previously completed surveys as part of the Women’s Life Paths Study, a longitudinal study initiated in 1967 by Sandra Tangri (Tangri & Jenkins, 1993). Participants completed lengthy questionnaires including items pertaining to occupational and family history, health and life satisfaction, and political attitudes and behavior; thus, the questionnaire was not obviously focused on mental health and body image.
On average, the women reported high levels of education (78.7% report having earned a postgraduate degree) and income (28.3% report a yearly household income of between US$50,000 and US$100,000, and 53.7% report yearly income of greater than US$100,000). Most women reported currently living with a partner or spouse (65.2%), and most women (82.4%) reported having children. Finally, the sample primarily identified as heterosexual (93.0%).
Measures
Body mass index.—
Participants were asked to self-report their height and weight, and BMI was calculated as weight in pounds multiplied by 703 divided by height in inches squared. BMI is a commonly used index that classifies adults as underweight (<18.5), normal weight (18.5–24.99), overweight (25–29.99), and obese (>30) (World Health Organization, 2009). In this study, participants’ mean scores on BMI fell within the “overweight” range (see Table 1).
Table 1.
Scale Means, Standard Deviations (SDs), and Correlations
| Instrument | M | SD | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|---|
| 1. Body mass index | 26.45 | 5.73 | — | ||||
| 2. Body esteem | 3.47 | 0.69 | −.45*** | — | |||
| 3. Subjective health | 3.82 | 0.92 | −.35*** | .32*** | — | ||
| 4. Psychological well-being | 4.88 | 0.72 | .04 | .26*** | .21** | — | |
| 5. Perceived age discrimination | 2.98 | 0.83 | .01 | −.31*** | −.14* | −.33*** | — |
Note. N = 237.
*p < .05. **p < .01. ***p < .001.
Perceptions of age discrimination.—
The five questions used to assess perceptions of age discrimination were adapted from measures of racial and gender discrimination and assessed attitudes about the treatment of older individuals (Branscombe et al., 1999; Schmitt et al., 2002). Items were rated on a scale of 1 (strongly disagree) to 6 (strongly agree) and included the statements “I consider myself a person who has been deprived of the opportunities that are available to others because of my age,” “Members of my age group have been deprived of the opportunities that are available to other age groups,” “Older people are excluded from many sectors of public life,” “After ending one’s working life, one is considered to be worthless,” and “The achievements of older people are not appreciated in our society.” Items were averaged to reach a total score, and a higher score reflects greater perceptions of discrimination against older adults. Reliability for this scale was acceptable in the present sample, α = .75.
Subjective health.—
Subjective health was measured using the item “In general, would you say your health is” with responses ranging from 1 (poor) to 5 (excellent). This question has been shown to be a reliable indicator of general health and has been associated with objective assessments of physical health (Benyamini, Leventhal, & Leventhal, 1999) and mortality (Idler & Benyamini, 1997).
Body esteem.—
The appearance esteem (10 items) and weight esteem (8 items) subscales from the Body Esteem Scale (Mendelson, Mendelson, & White, 2001) were used to assess body esteem. Sample items include “I like what I see when I look in the mirror” (appearance esteem) and “I am satisfied with my weight” (weight esteem). Item responses range from 1 (never) to 5 (always) and were averaged, with higher total scores reflecting greater body esteem. One item from the appearance esteem subscale, “I wish I looked like someone else” was omitted from the analyses due to a low item-total correlation. Reliability for this scale was high in the present sample, α = .94.
Psychological well-being.—
The five-item Mental Health subscale from the MOS 36-Item Short-Form Health Survey (Ware & Sherbourne, 1992) assessed general mental health and well-being. Items such as “During the past 4 weeks, have you felt downhearted and blue?” were rated on a 5-point scale ranging from 1 (all of the time) to 5 (none of the time), with higher scores reflecting better mental health. The 5-item subscale was constructed from the longer 38-item Mental Heath Inventory (MHI) by Ware and Sherbourne to serve as an assessment of mental health and includes items from each of the four major mental health dimensions (anxiety, depression, loss of behavior or emotional control, and psychological well-being). The sum of these five items correlated .95 with the full-length 38-item MHI. Reliability for this scale was good in the present sample, α = .82.
Creation of Measured/Observed Variables
I followed Russell, Kahn, Spoth, and Altmaier’s (1998) recommendation to construct three parcels, or measured indicators, for the three latent variables (perceptions of age discrimination, body esteem, and psychological well-being). An exploratory factor analysis was first performed using the maximum likelihood method of extraction, and a single factor was specified to be extracted. The factor loadings from this analysis were rank ordered by their magnitude and successively assigned (from the highest to the lowest factor loading) to each of three parcels; this equalized the average loadings of each parcel on its respective latent factor. Last, items within each parcel were averaged to obtain a total parcel score. Parcel scores were used to estimate their respective latent variable within the SEM analyses.
Results
Any participants’ missing data were excluded from the analyses, and data were examined for normality of distribution. It is recommended that researchers testing structural equation models transform variables that have an absolute value of skewness > 3 or kurtosis > 10 (Kline, 2005). The skewness and kurtosis values for the variables and parcels were lower than these values (skewness range = −1.28 to 1.16 and kurtosis range −0.54 to 2.75); therefore, I did not transform any variable. Next, I calculated the means, SDs, and intercorrelations for all scales used (Table 1) as well as for the parcels used to estimate the model (Table 2). BMI was significantly negatively correlated with body esteem and subjective health. Body esteem was significantly positively correlated with subjective health and psychological well-being and negatively correlated with perceptions of age discrimination. Subjective health was positively correlated with psychological well-being and negatively correlated with perceptions of age discrimination. Last, perceptions of age discrimination were negatively correlated with psychological well-being.
Table 2.
Parcel Means, Standard Deviations (SDs), and Correlations
| Instrument | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Body esteem parcel 1 | 3.99 | .77 | — | |||||||
| 2. Body esteem parcel 2 | 3.20 | .75 | .76*** | — | ||||||
| 3. Body esteem parcel 3 | 3.22 | .75 | .74*** | .73*** | — | |||||
| 4. Psychological well-being parcel 1 | 4.85 | .85 | .30*** | .20** | .27*** | — | ||||
| 5. Psychological well-being parcel 2 | 4.56 | .87 | .22*** | .13* | .22** | .64*** | — | |||
| 6. Psychological well-being parcel 3 | 5.59 | .69 | .19** | .13* | .21** | .65*** | .53*** | — | ||
| 7. Perceived age discrimination parcel 1 | 2.54 | 1.10 | −.34*** | −.24*** | −.28*** | −.29*** | −.32*** | −.21** | — | |
| 8. Perceived age discrimination parcel 2 | 2.74 | 1.19 | −.28*** | −.16* | −.22** | −.24*** | −.27*** | −.10 | .57*** | — |
| 9. Perceived age discrimination parcel 3 | 2.20 | 1.23 | −.24*** | −.18** | −.20** | −.22** | −.23*** | −.15* | .52*** | .36*** |
Note. N = 237.
*p < .05. **p < .01. ***p < .001.
Test of the Hypothesized Latent Variable Model
For all latent variable analyses, EQS version 6.1 (Bentler, 1995) was used. The following fit indices were used: obtaining a root mean square error of approximation that is equal to or lower than 0.06, non-normed fit index, and comparative fit index values that equal or exceed 0.95 are an acceptable to good fit (Hu & Bentler, 1999). Values outside of these ranges reflect an unacceptable fit of the model to the data.
Examination of the measurement model.—
I first evaluated the measurement model using confirmatory factor analysis. The measurement model provided an acceptable to good fit to the data (see Table 3 for fit statistics for the current and all subsequent models). Significant parcel factor loadings ranged from 0.58 to 0.89 (p < .05), indicating that all latent factors were adequately operationalized. Therefore, this measurement model was used to test the hypothesized structural model. Parcel factor loadings are included in Figure 2, and the relationships between the latent variables are presented in Table 4.
Table 3.
Fit Statistics for Measurement Model, Structural Model, and Alternative Models Examined
| Model | χ2 | df | p Value | Δx 2 | CFI | NNFI | RMSEA (CI) |
|---|---|---|---|---|---|---|---|
| 1. Measurement model | 23.49 | 24 | .49 | — | 1.00 | 1.00 | 0.000 (0.000, 0.052) |
| 2. Structural model | 57.06 | 39 | .03 | — | 0.981 | 0.974 | 0.046 (0.014, 0.070) |
| 3. Alternate model 1, removed path from age discrimination to psychological well-being | 70.93 | 40 | .00 | −13.87*** | 0.968 | 0.956 | 0.059 (0.035, 0.081) |
| 4. Alternate model 2, added path from subjective health to psychological well-being | 54.15 | 38 | .04 | 2.916 | 0.983 | 0.976 | 0.044 (0.008, 0.068) |
| 5. Alternate model 3, removed path from body esteem to psychological well-being | 61.81 | 40 | .02 | −4.75* | 0.977 | 0.969 | 0.049 (0.022, 0.073) |
Notes. CFI = comparative fit index; CI = confidence interval; NNFI = non-normed fit index; RMSEA = root mean square error of approximation.
*p < .05. ***p < .001.
Figure 2.
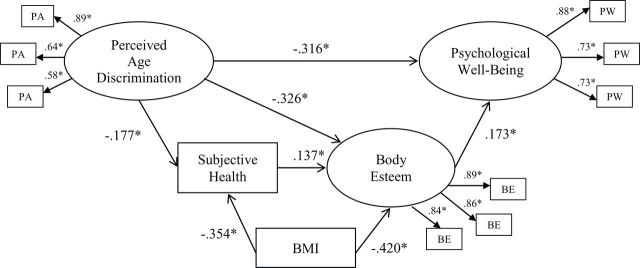
Path coefficients and parcel factor loadings for the structural model. Note. *p < .05.
Table 4.
Correlations Between the Latent Variables Obtained via Analyzing the Measurement Model
| Latent variable | 1 | 2 | 3 |
|---|---|---|---|
| 1. Perceived age discrimination | — | ||
| 2. Body esteem | −.39* | — | |
| 3. Psychological well-being | −.39* | .31* | — |
Note. *p < .05.
Examination of the structural model.—
Next, the hypothesized structural model was evaluated (Figure 2). As expected, this model provided a good fit to the data. All hypothesized path coefficients were significant and are presented in Figure 2. Analyses indicated that BMI and perceptions of age discrimination accounted for 15.7% of the variance in subjective health. BMI, subjective health, and perceptions of age discrimination accounted for 35.8% of the variance in body esteem. Body esteem and perceptions of age discrimination accounted for 16.8% of the variance in psychological well-being.
To examine whether body esteem partially mediated the relationship between perceptions of age discrimination and psychological well-being, the mediation with covariate bootstrap syntax provided by Preacher and Hayes (2004) was used. Using this method, a regression-based model for the effect of perceptions of age discrimination on psychological well-being through body esteem while controlling for BMI was estimated. As shown in Figure 3, body esteem partially mediated the association between perceptions of age discrimination and psychological well-being (indirect effect = −0.0472, SE = 0.0194, 95% confidence interval [CI]: [−0.0958, −0.0157]). Zero does not lie within the CI of the bootstrap estimate of the indirect effect of body esteem in the association between perceptions of age discrimination and psychological well-being, indicating that the indirect effect was indeed significant at p < .05.
Figure 3.
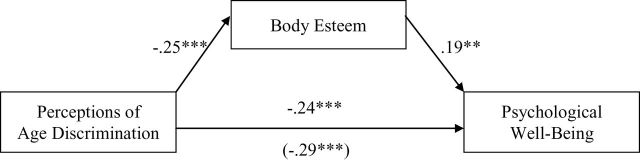
Standardized betas illustrating the mediating effect of body esteem in the relationship between perceptions of age discrimination and psychological well-being. Note. The coefficient in parentheses represents the total effect of perceptions of age discrimination on psychological well-being with body esteem not included in the model as a mediator. Coefficients significantly different from zero are noted by asterisks (**p < .01. ***p < .001).
To provide further evidence for the hypothesized model, a series of alternative models were explored (see Table 3). In each model, a direct path was added to or removed from the model presented in Figure 1. Based on extant literature and theory, the added paths were not expected to be significant, and models with paths removed were not expected to show a significant improvement in overall fit.
In the first alternative model, the path from perceptions of age discrimination to psychological well-being was removed. This path accounts for the direct association between perceptions of age discrimination and psychological well-being, and theoretically this association is expected to be significant (Paradies, 2006). Removing this path tests whether a more parsimonious model is a better fit to this data. The fit of the model was significantly worse when this path was removed. Therefore, this alternative model was rejected.
The second alternative model included a direct path between subjective health and psychological well-being. It is a possible alternative that health may be a partial mediator of the association between ageism and psychological well-being. However, adding this path to the model did not provide a better or worse fit to the data than did the hypothesized model.
Last, a third alternative model removing the path between body esteem and psychological well-being was tested. This path accounts for the direct association between body esteem and psychological well-being and is expected to add unique variance to the model. Removing it tests whether a more parsimonious model is a better fit to this data. The fit of the model was significantly worse when this path was removed. Therefore, this model was rejected.
Post hoc analyses.—
Due to the diverse ethnic makeup of the sample in this study, post hoc analyses were performed to assess whether the observed pattern of results adequately represents both ethnic groups. As is often noted in comparisons between these groups, the African American women reported a significantly higher average BMI than did the European American women (M European American = 25.18, SD = 5.21; M African American = 29.05, SD = 5.89, t(232) = 5.13, p < .001), though both groups’ average falls within the “overweight” range. However, the two groups did not differ significantly on measures of body esteem (M European American = 3.55, SD = 0.64; M African American = 3.61, SD = 0.70, t(236) = 0.58, p = .56), perceptions of age discrimination (M European American = 2.74, SD = 1.04; M African American = 2.94, SD = 1.16, t(235) = 1.33, p = .18), subjective health (M European American = 3.85, SD = 0.96; M African American = 3.76, SD = 0.83, t(235) = 0.68, p = .50), and psychological well-being (M European American = 4.95, SD = 0.68; M African American = 5.09, SD = 0.71, t(237) = 1.47, p = .14). Overall, the average scores for the two groups did not differ on any variables except for the control variable (BMI).
An examination of the pattern of correlations separately by ethnic group (Table 5) showed that for African American women, age discrimination was not significantly associated with body esteem, and subjective health was unrelated to other predictor and outcome variables. For both ethnic groups, body esteem was positively associated with psychological well-being, and age discrimination was negatively associated with psychological well-being. Because there were significant differences in the associations between the variables for the two groups, bootstrapping analyses used to estimate mediational effects were run separately by ethnic group. Results confirmed that body esteem partially mediated the association between age discrimination and psychological well-being among European American women (indirect effect = −.0705, SE = 0.0293, 95% CI: [−0.1395, −0.0244]). However, for African American women, this analysis was not significant (indirect effect = −0.0126, SE = 0.0233, 95% CI: [−0.0709, 0.0303]), indicating that there is not an indirect effect of age discrimination on psychological well-being via body esteem for this group.
Table 5.
Correlations Among Study Measures for European American and African American Women
| Measure | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Subjective health | — | .23** | −.17* | .28** |
| 2. Body esteem | .07 | — | −.34*** | .31*** |
| 3. Age discrimination | −.14 | −.16 | — | −.25** |
| 4. Psychological well-being | .15 | .25* | −.39** | — |
Note. Correlations for European American women (above diagonal) and African American women (below diagonal) controlling for body mass index.
*p < .05. **p < .01. ***p < .001.
Discussion
Researchers had yet to consider broad contextual variables such as ageism in conjunction with body image, and these findings indicate that age discrimination and body esteem are directly associated with older women’s psychological well-being. This study integrated these into one model and examined body esteem as a mediator of the association between age discrimination and psychological well-being for European American and African American women. To gain a nuanced understanding of older women’s body and health issues, we must consider the sociocultural context in which older women’s bodies are routinely evaluated and appraised—the context of ageism.
Social expectancy theory posits that culturally shared standards of attractiveness influence how we view (or stereotype) and interact with others, and these views are internalized and shape individuals’ behavior and self-perceptions (Jackson, 2004). This approach is particularly relevant when considering the effects of ageism on women’s body esteem and psychological well-being. Specifically, women may internalize ageism (Levy, 2001) and begin to view their own bodies through a discriminatory lens, potentially leading to negative body image. A wealth of literature has examined the associations between sexism, body image, and mental health (Fredrickson & Roberts, 1997), yet to date researchers have not considered how other forms of discrimination—such as ageism—may concurrently affect older women’s body image and psychological well-being.
To test this, I examined a structural equation model that examined the associations between these variables, including the indirect association between age discrimination and psychological well-being via body esteem. Overall, the model fit the data well, indicating that perceptions of age discrimination had a significant direct association with psychological well-being, as well as a significant indirect effect through body esteem for women in late middle age. However, post hoc analyses revealed that this pattern differs significantly by ethnic group, and mediation is present for European American but not African American women.
As expected, perceptions of age discrimination were directly associated with psychological well-being for both ethnic groups. That is, older women who reported greater perceptions of age discrimination also reported worse psychological well-being. Depression is the most prevalent mental health issue among older adults (Centers for Disease Control and Prevention and National Association of Chronic Disease Directors, 2009); however, age-specific causes of mental distress often go unexplored. The direct association replicated previous findings that discrimination affects mental health (Schmitt et al., 2002) and confirmed that age-based discrimination is one source of psychological distress for aging women.
Perceptions of age discrimination were significantly negatively associated with subjective health status and body esteem among European American women. Women in this ethnic group who reported greater perceptions of age discrimination had worse self-reported health and lower body esteem than those who reported less awareness of age-related discrimination. The link between ageism and health is complex due to the cultural association between aging and declining health. There is an implicit assumption that old age brings about poor health, and only individuals who are “aging successfully” (Rowe & Kahn, 1997) are able to circumvent or avoid physiological decline. However, this assumption fails to account for other causes of poor health among aging populations, such as discrimination. Furthermore, exposure to ageism is associated with worse body esteem among this ethnic group, indicating internalized ageism may take a toll on women’s self-perceptions with regard to the body.
Unexpectedly, these associations were not significant among African American women. Given the lack of association between age discrimination and body esteem, mediation was not present in this group. African American women have likely faced a lifetime of both overt and subtle racism and sexism, and it is possible that African American women’s responses to discrimination differ from other ethnic groups due to the multiple and intersecting nature of various forms of discrimination (Cole, 2009; King, 2003). African American women perceive themselves as targets of both racism and sexism, and racism is often perceived as a more severe problem than sexism (Miller, 1988). It is possible that ageism is not the most prevalent form of discrimination that African American women are facing and therefore may not have as strong an effect on other aspects of life; however, future research is needed to further explore these patterns.
Further, African Americans hold different definitions of what is considered “healthy” than other ethnic groups, potentially because the meanings associated with this term are often linked to cultural and personal experiences (Damron-Rodriguez, Frank, Enriquez-Haass, & Reuben, 2005). African Americans report thinking about health problems when answering questions about self-reported health, whereas European American individuals tend to think about physical functioning (Krause & Jay, 1994). It is possible that subjective differences in the meaning associated with questions about health could affect the differential associations observed between ethnic groups.
Researchers have suggested a link between subjective health and body esteem among aging women (Chrisler & Ghiz, 1993), but this association had yet to be tested empirically. These findings indicate that European American women who are in better health also feel more positively about their bodies, and those who indicated poorer subjective health were less satisfied with their bodies. Older adults who show signs of physical decline are often judged harshly because health, like beauty, is associated with positive traits and is assumed to be controllable (Calasanti, 2005). It is no coincidence that health and beauty are judged with similar paradigms; both are visible markers that are taken to indicate personal characteristics (Eagly, Ashmore, Makhijani, & Longo, 1991), despite that we often have little control over our health or body features. Older European American women who are in poor health may judge their own bodies harshly because they may perceive a lack of control over the body.
Interestingly, subjective health was unrelated to body esteem for African American women. This lack of an observed association may be one form of the “buffering effect,” the theory African American women are protected from negative body esteem and associated negative outcomes (Abrams, Allen, & Gray, 1993; Molloy & Hertzberger, 1998; Root, 1990). Younger African American women tend to feel more positively about their bodies compared with other ethnic groups (Grabe & Hyde, 2006), and on average, women in this ethnic group are less likely to place their self-worth on maintaining a particular body size (Sabik, Cole, & Ward, 2010). In the current study, African American women reported higher average BMI yet similar levels of body satisfaction compared with European American women. Whereas older European American women may feel more negatively about their bodies as a result of perceived health issues, African American women appear to disassociate health and body esteem, thereby protecting themselves from low body esteem in the face of health issues. The buffering hypothesis has not yet been extended to older women, and this provides preliminary evidence that older African American women may be strategically holding body esteem separate from other aspects of life.
Body esteem was significantly positively associated with psychological well-being for women in both ethnic groups, such that women who felt more positively about their bodies also reported more positive psychological well-being. This finding provides evidence that low body esteem is associated with psychological well-being among older women and confirms that women in this age range are not free from body image concerns (Hurd Clarke et al., 2009; Peat et al., 2008). The misperception that aging women no longer care about their looks is inaccurate (Hurd, 2000), and perpetuating this stereotype may cause medical health professionals to overlook this as an important factor in women’s psychological well-being.
Furthermore, body esteem partially mediated the relationship between perceptions of age discrimination and psychological well-being for European American women. This finding helps explain the mechanism driving the association between perceived age discrimination and psychological well-being; older women who report greater perceptions of age discrimination may internalize these negative stereotypes and may assess themselves and their own bodies in a negative light. Programs aimed at reducing age discrimination may be associated with greater body esteem and psychological well-being for women in this ethnic group.
This study had a number of limitations. First, the measure of health status was subjective and relied on self-report. Although this has been demonstrated as a reliable indicator of health, utilizing multiple measures of health and well-being and taking into account how different kinds of health issues affect functioning (Heidrich, 1993) will strengthen this area of research. Changes in health and physical functioning are likely to affect body image among aging women, and various aspects of health and functioning need to be addressed in future research. The sample for the current study was well educated and included only women in their early 60s. Research has shown that socioeconomic status and education levels can affect health in later life (Shankar, McMunn, & Steptoe, 2010), and future research should examine how class status and other social categories affect these associations.
This study was correlational in design, and future research needs to be conducted to examine the causality of these associations. The sample size for this study was relatively small and thus may have failed to provide sufficient statistical power to distinguish between models tested and prevented the comparison of model fit between ethnic groups.
The average level of age discrimination reported by this sample was low, and it is possible that not many women in the sample have experienced age discrimination due to the relatively young age of the sample (i.e., late middle aged). Additionally, body perceptions may change with age (Covan, 2005), and these patterns may differ for women at older ages. Future research should examine this model among women that have fully transitioned into old age. Researchers have found that subjective well-being increases with age, though there is significant individual variation in the rate of increase in life satisfaction over time (Gana, Bailly, Saada, Joulain, & Alaphilippe, 2013). It is possible that perceptions of age discrimination and body esteem account for some of this variation, and future research should examine these associations longitudinally. Sexual satisfaction is also likely affected by body perceptions and is of concern for older women, for whom sexual unwellness has been associated with poorer self-rated health and depression (Syme, Klonoff, Macera, & Brodine, 2013).
Older women are likely to have spent a lifetime dealing with sexism, and those who are members of ethnic minority groups have also likely faced racism. However, little attention has been given to the effects of concurrent and intersecting forms of discrimination. Future research should consider these intersections (Cole, 2009) and should assess internalized ageism and the effect on the body esteem and mental health of older women in diverse ethnic groups.
To improve the body esteem and psychological well-being of older women, we need to work to make visible and reduce ageism and other forms of discrimination. By doing so, we may increase positive body esteem and improve psychological well-being and health. Second, we need to actively promote programs aimed at increasing positive body esteem among aging women. Perceptions of the body have been linked to identity and health behaviors for women across the life span, and women with positive body esteem are in better health, both mentally and physically (Peat et al., 2008; Wilcox, 1997). Body image is a crucial yet often overlooked aspect of quality of life (Cash & Fleming, 2002). Feelings about the body are central to well-being for all individuals, but particularly for older women, for whom body appearance and function directly affect psychological well-being.
Funding
This work was supported by the National Science Foundation Graduate Student Research Fellowship under grant no. DGE 0718128 and by training grant T32 AG000204 from the National Institute on Aging (N. J. Sabik).
Acknowledgments
I am grateful to Elizabeth Cole, Nicky Newton, and Alyssa Zucker for helpful feedback on the manuscript.
References
- Abrams K. K., Allen L. R., Gray J. J. (1993). Disordered eating attitudes and behaviors, psychological adjustment, and ethnic identity: A comparison of black and white female college students. The International Journal of Eating Disorders, 14, 49–57. 10.1002/1098-108X(199307)141<49AID-EAT2260140107>3.0.CO;2-Z [DOI] [PubMed] [Google Scholar]
- Antonucci T. C., Blieszner R., Denmark F. L. (2010). Psychological perspectives on older women. In H. Landrine & N. F. Russo (Eds.), Handbook of diversity in feminist psychology (pp. 233–257). New York, NY: Springer Publishing Co. [Google Scholar]
- Bedford J. L., Johnson C. S. (2006). Societal influences on body image dissatisfaction in younger and older women. Journal of Women & Aging, 18, 41–55. 10.1300/J074v18n01_04 [DOI] [PubMed] [Google Scholar]
- Bentler P. M. (1995). EQS structural equation program manual. Encino, CA: Multivariate Software. [Google Scholar]
- Benyamini Y., Leventhal E. H., Leventhal H. (1999). Self-assessments of health. What do people know that predicts their mortality? Research on Aging, 21, 477–500. 10.1177/0164027599213007 [Google Scholar]
- Branscombe N. R., Schmitt M. T., Harvey R. D. (1999). Perceiving pervasive discrimination among African Americans: Implication for group identification and well-being. Journal of Personality and Social Psychology, 28, 135–149. 10.1037/0022-3514.77.1.135 [Google Scholar]
- Butler R. N. (1969). Age-Ism: Another form of bigotry. Gerontologist, 9, 243–246. 10.1093/geront/9.4_Part_1.243 [DOI] [PubMed] [Google Scholar]
- Calasanti T. (2005). Ageism, gravity, and gender: Experiences of aging bodies. Generations, 29, 8–12. [Google Scholar]
- Cash T. F., Fleming E. C. (2002). The impact of body image experiences: Development of the body image quality of life inventory. The International Journal of Eating Disorders, 31, 455–460. 10.1002/eat.10033 [DOI] [PubMed] [Google Scholar]
- Celejewski I., Dion K. K. (1998). Self-perception and perception of age groups as a function of the perceiver’s category membership. International Journal of Aging & Human Development, 47, 205–216. 10.2190/GL4R-FJ7G-XGEK-MRR6 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention and National Association of Chronic Disease Directors. (2009). The state of mental health and aging in America. Issue brief 2: Addressing depression in older adults: Selected evidence-based programs. Atlanta, GA: National Association of Chronic Disease Directors. [Google Scholar]
- Chrisler J. C., Ghiz L. (1993). Body image issues of older women. Women & Therapy, 14, 67–75. 10.1300/J015v14n01_07 [Google Scholar]
- Cole E. R. (2009). Intersectionality and research in psychology. The American Psychologist, 64, 170–180. 10.1037/a0014564 [DOI] [PubMed] [Google Scholar]
- Covan E. K. (2005). Meaning of aging in women’s lives. Journal of Women & Aging, 17, 3–22. 10.1300/J074v17n03_02 [DOI] [PubMed] [Google Scholar]
- Damron-Rodriguez J., Frank J. C., Enriquez-Haass V. L., Reuben D. B. (2005). Definitions of health among diverse groups of elders: Implications for health promotion. Generations, 29, 11–16. [Google Scholar]
- Eagly A. H., Ashmore R. D., Makhijani M. G., Longo L. C. (1991). What is beautiful is good, but…: A meta-analytic review of research on the physical attractiveness stereotype. Psychological Bulletin 110, 109–128. 10.1037//0033-2909.110.1.109 [Google Scholar]
- Forman M., Davis W. N. (2005). Characteristics of middle-aged women in inpatient treatment for eating disorders. Eating Disorders, 13, 231–243. 10.1080/10640260590932841 [DOI] [PubMed] [Google Scholar]
- Fredrickson B. L., Roberts T. A. (1997). Objectification theory: Toward understanding women’s lived experiences and mental health risks. Psychology of Women Quarterly, 21, 173–206. 10.1111/j.1471-6402.1997.tb00108.x [Google Scholar]
- Gana K., Bailly N., Saada Y., Joulain M., Alaphilippe D. (2013). Does life satisfaction change in old age: Results from an 8-year longitudinal study. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 68, 540–552. 10.1093/geronb/gbs093 [DOI] [PubMed] [Google Scholar]
- Garner J. D. (1999). Feminism and feminist gerontology. Journal of Women & Aging, 11, 3–12. 10.1300/J074v11n02_02 [DOI] [PubMed] [Google Scholar]
- Garstka T. A., Schmitt M. T., Branscombe N. R., Hummert M. L. (2004). How young and older adults differ in their responses to perceived age discrimination. Psychology and Aging, 19, 326–335. 10.1037/0882-7974.19.2.326 [DOI] [PubMed] [Google Scholar]
- Grabe S., Hyde J. S. (2006). Ethnicity and body dissatisfaction among women in the United States: A meta-analysis. Psychological Bulletin, 132, 622–640. 10.1037/0033-2909.132.4.622 [DOI] [PubMed] [Google Scholar]
- Gupta M. A. (1990). Fear of aging: A precipitating factor in late onset anorexia nervosa. International Journal of Eating Disorders, 9, 221–224. 10.1002/1098-108X(199003)9:2 [Google Scholar]
- Heidrich S. M. (1993). The relationship between physical health and psychological well-being in elderly women: A developmental perspective. Research in Nursing & Health, 16, 123–130. 10.1002/nur.4770160207 [DOI] [PubMed] [Google Scholar]
- Herek G. M., Gillis J. R., Cogan J. C. (1999). Psychological sequelae of hate-crime victimization among lesbian, gay, and bisexual adults. Journal of Consulting and Clinical Psychology, 67, 945–951. 10.1037//0022-006X.67.6.945 [DOI] [PubMed] [Google Scholar]
- Hess T. M., Auman C., Colcombe S. J., Rahhal T. A. (2003). The impact of stereotype threat on age differences in memory performance. Journals of Gerontology, 58B, 3–11. 10.1093/geronb/58.1.P3 [DOI] [PubMed] [Google Scholar]
- Hu L., Bentler P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. 10.1080/ 10705519909540118 [Google Scholar]
- Hurd L. C. (2000). Older women’s body image and embodied experience: An exploration. Journal of Women & Aging, 12, 77–97. 10.1300/J074v12n03_06 [DOI] [PubMed] [Google Scholar]
- Hurd Clarke L., Griffin M., Maliha K. (2009). Bat wings, bunions, and turkey wattles: Body transgressions and older women’s strategic clothing choices. Aging & Society, 29, 709–726. 10.1017/S0144686X08008283 [Google Scholar]
- Idler E. L., Benyamini Y. (1997). Self-rated health and mortality: A review of twenty-seven community studies. Journal of Health and Social Behavior, 38, 21–37. 10.2307/2955359 [PubMed] [Google Scholar]
- Inzlicht M., McKay L., Aronson J. (2006). Stigma as ego depletion: How being the target of prejudice affects self-control. Psychological Science, 17, 262–269. 10.1111/j.1467-9280. 2006.01695.x [DOI] [PubMed] [Google Scholar]
- Jackson L. A. (2004). Physical attractiveness: A sociocultural perspective. In Cash T. F., Pruzinsky T. (Eds.), Body images: A handbook of theory, research, and clinical practice (pp. 13–21). New York, NY: Guilford Press. [Google Scholar]
- King K. R. (2003). Racism or sexism? Attributional ambiguity and simultaneous membership in multiple oppressed groups. Journal of Applied Social Psychology, 33, 223–247. 10.1111/j.1559-1816.2003.tb01894.x [Google Scholar]
- Kline R. B. (2005). Structural equation modeling. New York, NY: Guilford Press. [Google Scholar]
- Klonoff E. A., Landrine H., Campbell R. (2000). Sexist discrimination may account for well-known gender differences in psychiatric symptoms. Psychology of Women Quarterly, 24, 93–99. 10.1111/j.1471–6402.2000.tb01025.x [Google Scholar]
- Krause N. M., Jay G. M. (1994). What do global self-rated health items measure? Medical Care, 32, 930–942. 10.1097/ 00005650-199409000-00004 [DOI] [PubMed] [Google Scholar]
- Levy B. R. (2000). Handwriting as a reflection of aging self-stereotypes. Journal of Geriatric Psychology, 33, 81–94. [Google Scholar]
- Levy B. R. (2001). Eradication of ageism requires addressing the enemy within. The Gerontologist, 41, 578–579. 10.1093/geront/41.5.578 [DOI] [PubMed] [Google Scholar]
- Levy B. R., Hausdorff J. M., Hencke R., Wei J. Y. (2000). Reducing cardiovascular stress with positive self-stereotypes of aging. The Journals of Gerontology, 55B, 205–213. 10.1093/geronb/55.4.P205 [DOI] [PubMed] [Google Scholar]
- Levy B. R., Slade M. D., Kunkel S. R., Kasl S. V. (2002). Longevity increased by positive self-perceptions of aging. Journal of Personality and Social Psychology, 83, 261–270. 10.1037/0022- 3514.83.2.261 [DOI] [PubMed] [Google Scholar]
- Lewis D. M., Cachelin F. M. (2001). Body image, body dissatisfaction, and eating attitudes in midlife and elderly women. Eating Disorders, 9, 29–39. 10.1080/106402601300187713 [DOI] [PubMed] [Google Scholar]
- Mangweth-Matzek B., Rupp C. I., Hausmann A., Assmayr K., Mariacher E., Kemmler G. … Biebl W. (2006). Never too old for eating disorders or body dissatisfaction: A community study of elderly women. International Journal of Eating Disorders, 39, 583–586. 10.1002/eat.20327 [DOI] [PubMed] [Google Scholar]
- Mendelson B. K., Mendelson M. J., White D. R. (2001). Body-esteem scale for adolescents and adults. Journal of Personality Assessment, 76, 90–106. 10.1207/S15327752JPA7601_6 [DOI] [PubMed] [Google Scholar]
- Miller F. S. (1988). Network structure support: Its relationship to the psycho-social development of Black females. Journal of Black Psychology, 15, 17–39. [Google Scholar]
- Molloy B. L., Hertzberger S. D. (1998). Body image and self esteem: A comparison of African American and Caucasian women. Sex Roles, 38, 631–643. [Google Scholar]
- Nelson T. D. (2005). Ageism: Prejudice against our feared future self. Journal of Social Issues, 61, 207–221. 10.1111/j.1540- 4560.2005.00402.x [Google Scholar]
- Nemmers T. M. (2004). The influence of ageism and ageist stereotypes on the elderly. Physical and Occupational Therapy in Geriatrics, 22, 11–20. 10.1300/J148v22n04_02 [Google Scholar]
- Paradies Y. (2006). A systematic review of empirical research on self-reported racism and health. International Journal of Epidemiology, 35, 888–901. 10.1093/ije/dyl056 [DOI] [PubMed] [Google Scholar]
- Pascoe E. A., Richman L. S. (2009). Perceived discrimination and health: A meta-analytic review. Psychological Bulletin, 135, 531–554. 10.1037/a0016059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peat C. M., Peyerl N. L., Muehlenkamp J. J. (2008). Body image and eating disorders in older adults: A review. The Journal of General Psychology, 135, 343–358. 10.3200/GENP.135.4.343-358 [DOI] [PubMed] [Google Scholar]
- Preacher K. J., Hayes A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers, 36, 717–731. 10.3758/BF03206553 [DOI] [PubMed] [Google Scholar]
- Rodin J., Silberstein L., Striegel-Moore R. (1984). Women and weight: A normative discontent. Nebraska Symposium on Motivation 1984 (pp. 267–304). Lincoln, NE: University of Nebraska Press. [PubMed] [Google Scholar]
- Root M. P. P. (1990). Disordered eating in women of color. Sex Roles, 22, 525–536. 10.1007/BF00288168 [Google Scholar]
- Rowe J. W., Kahn R. L. (1997). Successful aging. The Gerontologist, 37, 433–440. 10.1093/geront/37.4.433 [DOI] [PubMed] [Google Scholar]
- Russell D. W., Kahn J. H., Spoth R., Altmaier E. M. (1998). Analyzing data from experimental studies: A latent variable structural equation modeling approach. Journal of Counseling Psychology, 45, 18–29. 10.1037/0022-0167.45.1.18 [Google Scholar]
- Sabik N. J., Cole E. R., Ward L. M. (2010). Are all minority women equally buffered from negative body image? Intra-ethnic moderators of the buffering hypothesis. Psychology of Women Quarterly, 34, 139–151. 10.1111/j.1471-6402.2010.01557.x [Google Scholar]
- Saucier M. G. (2004). Midlife and beyond: Issues for aging women. Journal of Counseling and Development, 82, 420–425. 10.1002/ j.1556–6678.2004.tb00329.x [Google Scholar]
- Schmitt M. T., Branscombe N. R. (2002). The meaning and consequences of perceived discrimination in disadvantaged and privileged social groups. In Stroebe W., Hewstone M. (Eds.), European review of social psychology (Vol. 12, pp. 167–199). Chichester, England: Wiley. 10.1080/14792772143000058 [Google Scholar]
- Schmitt M. T., Branscombe N. R., Kobrynowicz D., Owen S. (2002). Perceiving discrimination implications for well-being in women and men. Personality and Social Psychology Bulletin, 28, 197–210. 10.1177/0146167202282006 [Google Scholar]
- Shankar A., McMunn A., Steptoe A. (2010). Health-related behaviors in older adults: Relationships with socioeconomic status. American Journal of Preventive Medicine, 38, 39–46. 10.1016/j.amepre.2009.08.026 [DOI] [PubMed] [Google Scholar]
- Slotterback C. S. (1996). Projections of aging: Impact of generational differences and the aging process on perceptions of adults. Psychology and Aging, 11, 552–559. 10.1037//0882-7974.11.3.552 [DOI] [PubMed] [Google Scholar]
- Sontag S. (1972). The double standard of aging. Saturday Review of Literature, 39, 29–38. [Google Scholar]
- Swim J., Stangor C. (Eds.) (1998). Prejudice: The target’s perspective. San Diego, CA: Academic Press. [Google Scholar]
- Syme M. L., Klonoff E. A., Macera C. A., Brodine S. K. (2013). Predicting sexual decline and dissatisfaction among older adults: The role of partnered and individual physical and mental health factors. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 68, 323–332. 10.1093/geronb/gbs087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szymanski D. M., Henning S. L. (2007). The role of self-objectification in women’s depression: A test of objectification theory. Sex Roles, 56, 45–53. 10.1007/s11199-006-9147-3 [Google Scholar]
- Tangri S. S., Jenkins S. R. (1993). The University of Michigan class of 1967: The women’s life path study. In Hulbert K. D., Schuster D. T. (Eds.), Women’s lives through time: Educated women of the twentieth century. San Francisco, CA: Jossey-Bass Publishers. [Google Scholar]
- Tiggemann M. (2004). Body image across the adult life span: Stability and change. Body Image, 1, 29–41. 10.1016/S1740-1445(03) 00002-0 [DOI] [PubMed] [Google Scholar]
- Voda A. M., Christy N. S., Morgan J. M. (1991). Body composition changes in menopausal women. Women & Therapy, 11, 71–96. 10.1300/J015V11N02_07 [Google Scholar]
- Ware J. E., Sherbourne C. D. (1992). The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30, 473–483. 10.1097/00005650-199206000-00002 [PubMed] [Google Scholar]
- Wilcox S. (1997). Age and gender in relation to body attitudes: Is there a double standard of aging? Psychology of Women Quarterly, 21, 549–565. 10.1111/j.1471–6402.1997.tb00130.x [Google Scholar]
- Williams D. R., Mohammed S. A. (2009). Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine, 32, 20–47. 10.1007/s10865-008-9185-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams D. R., Neighbors H. W., Jackson J. S. (2003). Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health, 93, 200–208. 10.2105/AJPH.93.2.200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams D. R., Yu Y., Jackson J., Anderson N. (1997). Racial differences in physical and mental health: Socio-economic status, stress and discrimination. Journal of Health Psychology, 2, 335–351. 10.1177/135910539700200305 [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2009). Global database on body mass index Retrieved from http://apps.who.int/bmi/
- Zucker A. N., Landry L. J. (2007). Embodied discrimination: The relation of sexism and distress to women’s drinking and smoking behaviors. Sex Roles, 56, 193–203. 10.1007/s11199-006-9163-3 [Google Scholar]