

Abstract
Background
In a previously published randomized controlled trial (Brown et al. Alcohol Clin Exp Res 2010; 34, 292–301), our research team showed that a 30-minute brief motivational interviewing (BMI) session was more effective in reducing percentages of risky drinking days in drunk driving recidivists than a control information–advice intervention at 12-month follow-up. In this sequel to the initial study, 2 main hypotheses were tested: (i) exposure to BMI increases the time to further arrests and crashes compared with exposure to the control intervention (CTL) and (ii) characteristics, such as age, moderate the benefit of BMI.
Methods
A sample of 180 community-recruited recidivists who had drinking problems participated in the study. Participants gave access to their provincial driving records at baseline and were followed up for a mean of 1,684.5 days (SD = 155.7) after randomization to a 30-minute BMI or CTL session. Measured outcomes were driving arrests followed by convictions including driving while impaired (DWI), speeding, or other moving violations as well as crashes. Age, readiness to change alcohol consumption, alcohol misuse severity, and number of previous DWI convictions were included as potential moderators of the effect of the interventions.
Results
For arrests, Cox proportional hazards modeling revealed no significant differences between the BMI and the CTL group. When analyses were adjusted to age tertile categories, a significant effect of BMI in the youngest age tertile (<43 years old) emerged. For crashes, no between-group differences were detected.
Conclusions
BMI was better at delaying DWI and other dangerous traffic violations in at-risk younger drivers compared with a CTL similar to that provided in many remedial programs. BMI may be useful as an opportunistic intervention for DWI recidivism prevention in settings such as DWI courts. Treatment effectiveness studies are needed to ascertain how the present findings generalize to the real-world conditions of mandated relicensing programs.
Keywords: Driving While Impaired, Driving Under the Influence, Infraction, Accident, Motivational Interviewing, Recidivism
Progress in reducing road traffic crashes related to driving while impaired (DWI) by alcohol has stalled in the first decade of the twenty-first century after 3 decades of significant improvement (Vanlaar et al., 2012). In part, this loss of momentum is attributable to the intervention refractoriness of a more “hard-core” group of repeated offenders (Simpson et al., 2004). More than other drunk drivers, these offenders have severer drinking problems, drive more frequently with higher blood alcohol levels, demonstrate limited problem recognition (Nochajski and Stasiewicz, 2006), and engage in other risky driving behaviors (e.g., speeding, reckless and unbelted driving; Donovan, 1989; Jonah et al., 2001)—factors that converge to further amplify their crash risk.
Both administrative and psychosocial remedial strategies are deployed to counter recidivism following a DWI arrest. While certain administrative strategies such as interlock programs have been associated with reductions in DWI recidivism and crashes while installed (Voas et al., 2010a), high-quality evidence of the lasting effects from most contemporary psychosocial intervention approaches either is unavailable or provides only marginal support for their effectiveness (Anderson et al., 2009; C'de Baca et al., 2001; Dill and Wells-Parker, 2006; Elder et al., 2005; Timko et al., 2011; Voas and Fisher, 2001; Williams et al., 2007). Moreover, many convicted DWI offenders (higher than 50% in some jurisdictions) choose to either not engage or significantly delay participation in remedial programs required for relicensing often involving evaluation and/or treatment of alcohol misuse. Their reluctance to participate appears to stem from a combination of factors, including limited problem recognition, ambivalence about the need to alter drinking behavior, and little readiness to pay relicensing costs. The result is that these individuals might be at greater risk of further drink-driving compared with drivers who more promptly participate in DWI remedial relicensing programs (Brown et al., 2008; Voas et al., 2010b).
The high rate of nonengagement in remedial programs among the riskiest offenders has led to interest in opportunistic, brief motivation-enhancing interventions that could heighten their readiness to change and reduce their alcohol misuse (Dill and Wells-Parker, 2006; Freeman et al., 2005; Nochajski and Stasiewicz, 2006). Motivational interviewing (MI; Miller and Rose, 2009) represents the motivational approach with the most support for its effectiveness in reducing alcohol-related problems in diverse contexts and populations (Dunn et al., 2001; Smedslund et al., 2011). There is emerging evidence that MI may be beneficial in reducing drinking in DWI offenders and self-reported DWI events as well. A randomized controlled trial by our research group (Brown et al., 2010) investigated the impact of one 30-minute session of brief motivational interviewing (BMI) versus a 30-minute information control intervention (CTL). In a nonclinical sample of DWI recidivists diagnosed with alcohol abuse (N = 184), many of whom had significantly delayed participation in relicensing remediation, both interventions reduced days of risky drinking at 6- and 12-month follow-up. BMI, however, produced significantly greater reductions in an alcohol biomarker of excessive drinking at 6-month follow-up as well as in self-reported risky drinking days from the 6- to 12-month follow-ups compared with CTL. This demonstration of BMI's effectiveness in reducing both self-report and biologic indices of alcohol misuse in a community-recruited, nonclinical sample of recidivists extended the results of 2 previous controlled trials that indicated the self-reported benefits of MI in reducing both problem drinking (Woodall et al., 2007) and drink-driving behaviors (Stein et al., 2006) in forensic samples. In addition, subsequent fine-grained analyses of our 1-year outcomes (Brown et al., 2010) indicated that younger age, lower readiness to change, and severity of alcohol use symptoms and consequences were associated with the greatest benefits following exposure to the brief interventions provided (Brown et al., 2012), findings that have been observed in other populations (Heather et al., 1996; Mallett et al., 2010; Witkiewitz et al., 2010). Finally, DWI offenders with antisocial personality disorder tended to fare better with exposure to MI compared with those with no disorder (Woodall et al., 2007). Overall, these strands of evidence hint that brief interventions may hold selective benefits for DWI recidivists possessing certain characteristics associated with high risk.
A reduction in alcohol misuse in DWI recidivists represents an important public health outcome. Nevertheless, our preliminary results did not directly address BMI's advantage of reducing alcohol-related driving risk indicators over time, such as the number of alcohol-related road traffic crashes or DWI reconvictions. At the same time, while possessing more ecological validity, these dependent variables pose important shortcomings that vex most DWI research. Both variables reflect infrequent events subject to bias from arbitrary factors (e.g., enfor-cement practices, incomplete documentation, court delay, frequent plea bargaining to a lesser charge; Dill and Wells-Parker, 2006; Meyer and Gray, 1997; Rauch et al., 2010). As well, many offenders continue to drive under the influence of elevated but under per se blood alcohol concentration limits and under the influence of drug use, which individually or synergistically significantly impair their safe driving ability (C'de Baca et al., 2009). Drug-impaired driving, although increasingly prevalent, is more difficult to detect than alcohol-impaired driving (Brown and Ouimet, 2012; Lapham et al., 2002). Alternatively, self-reported information concerning DWI events is also problematic. It is subjective, often unreliable (Lapham et al., 2002), and when used in outcome studies, vulnerable to bias from sample attrition when follow-up durations are lengthy. To overcome these hurdles, a multidimensional approach to the measurement of alcohol-related driving risks, including using indicators of risky driving behavior (e.g., speeding), can increase the comprehensiveness and sensitivity of analyses (Nochajski and Stasiewicz, 2006; Rauch et al., 2010).
The present study extends Brown and colleagues' (2010) evaluation of the impact of 2 brief interventions in DWI recidivists. Whereas the initial study examined 12-month outcomes via self-reported and biologic markers of alcohol misuse, the present study examined outcomes related to risky driving convictions and crashes over a 5-year period following intervention. Two principal hypotheses were tested in the current study: (i) in DWI recidivists, exposure to BMI significantly delays a subsequent crash or arrest (followed by a conviction) for DWI, speeding, or other moving traffic violations compared with exposure to CTL; and (ii) recidivist characteristics, specifically age, readiness to change, alcohol misuse severity, and intervention refractoriness, moderate the long-term benefits of BMI.
Materials and Methods
Initial Study: Participants, Recruitment, Study Design, and Interventions
A previous report (Brown et al., 2010) provides complete details about participants, recruitment, participant study flow through and attrition, study design, and interventions. In summary, a community-based sample of DWI recidivists (2 or more convictions) with signs of problem drinking (scores equal to or higher than 8 on the Alcohol Use Disorders Identification Test [AUDIT]; Saunders et al., 1993) was recruited through advertisements in local papers, invitation letters sent by the Quebec Licensing and Insurance Bureau (Société de l'assurance automobile du Québec [SAAQ]), and word of mouth. The Ethics Committee of the Douglas Mental Health University Institute approved and provided oversight to the recruitment and all study protocols. At study recruitment, participants were asked for informed consent giving investigators access to their driving records maintained by the SAAQ.
The study was a double-blind randomized controlled trial in which participants were assigned at baseline to either BMI or CTL. Participants were enrolled in the study between July 2005 and January 2007. Both the BMI and the CTL interventions consisted of one 30-minute session designed and manualized in a pilot study (Chanut et al., 2007). BMI was inspired by the principles and techniques of MI (Miller, 1996) and involves an empathic interviewing style that: (i) recognizes, explores, and aims at resolving client ambivalence to facilitate behavior change; (ii) enhances self-efficacy; (iii) entertains flexible strategies for resolving alcohol misuse and DWI; (iv) avoids argumentation, advising, or convincing; (v) deploys tactics to “roll with resistance”; and (vi) seeks to elicit participant expression of intentions and commitment to change risky drinking (i.e., “change talk” and “commitment talk”). The CTL intervention consisted of delivery of scripted information on the risks of alcohol misuse and DWI, advice to change alcohol misuse, and information about available substance abuse treatment services.
Current Study: Participants
For the purposes of the present study, individuals were included who were initially eligible for participation in the Brown and colleagues (2010) study, but who were also licensed in Quebec at intake and gave consent to access their official driving record.
Measures
Driving Records
Participants' driving behavior was monitored via their driving records from study enrollment up to December 31, 2010. Participants gave access to the investigators to their driving records by providing their driving license identification and signing the informed consent at baseline. Each informed consent was also identified with a research identification number. Signed consents were sent to the SAAQ in the fall of 2011 in order to allow all the convictions to be compiled in the SAAQ database. The team received a driving record database from the SAAQ in which participants were only identified by their research identification number. The creation and management of this database conformed to legal and ethical contingencies and standard operating procedures in this regard of both the SAAQ and the Douglas Mental Health University Institute.
Main Dependent Variables
The main dependent variable in this study was the lapse of time in days to a first risky driving event or a crash following exposure to intervention. A risky driving event was operationalized as an arrest for which there was ultimately a conviction for any Criminal Code (e.g., DWI, dangerous operation of a motor vehicle) or Traffic Safety Code violation (e.g., speeding, going through a red light or stop sign, not wearing a safety belt). Time to arrest was chosen over time to conviction because the latter can be confounded by arbitrary factors (e.g., court delay). Crashes included any documented event involving an injury or death.
Moderating Variables
Four moderating variables were examined: age, readiness to change alcohol consumption, alcohol misuse severity, and intervention refractoriness. The 12-item Readiness to Change Alcohol Questionnaire (Heather et al., 1993) based on the Prochaska and DiClemente's Stages of Change model (Prochaska et al., 1992) was used to classify an individual into precontemplation, contemplation, or action concerning their alcohol use. It has been validated for use with the DWI population (Wells-Parker et al., 1998). Alcohol misuse severity was assessed with the AUDIT (Saunders et al., 1993), a 10-item screening questionnaire that validly measures drinking behavior and alcohol-related problems in DWI offenders (Conley, 2001). Intervention refractoriness was gauged by the frequency of past DWI convictions prior to study induction. For the purpose of analyses, age, AUDIT scores, and past DWI convictions were transformed into tertile categories.
Analytic Framework
Cox proportional hazards modeling assessed the effect of assignment to either BMI or CTL in delaying the time to the first documented arrest or crash over the follow-up period. Cox proportional hazards modeling was conducted separately for each potential moderation effect of recidivists' age, intake stage of change, alcohol misuse severity, and number of past DWI convictions. Moderation was indicated by a significant interaction between the group and the moderator variable after accounting for the group and the moderator effects. Alpha for inferences of significance of group main effects was set at p < 0.05, while alpha for inferences of significant moderation effects was corrected for the number of moderator categories (i.e., p < 0.017 for 3 categories).
Results
Current Versus Initial Sample
The final sample included 180 participants (BMI, n = 85; CTL, n = 95). This sample differed from the sample described in Brown and colleagues (2010; i.e., N = 184; BMI, n = 92; CTL, n = 92) in the following ways: (i) 11 participants of the original study were not included in the current study: the recidivism status of 7 participants could not be officially confirmed (e.g., drivers were asked about DWI convictions in the past 15 years, but official documentation was limited to the last 10 years), 2 refused to sign the authorization form to release their driving records, and 2 signed the release but were licensed in another Canadian province, precluding access to their driving record; (ii) 7 participants excluded from the initial study analysis through attrition from 6- and 12-month follow-ups were added in the current study as they had provided informed consent to access their driving records. One hundred and seventy-three participants were common to both the initial study and the current study. Analyses to compare the original Brown and colleagues (2010) study cohort (N = 184) with the present cohort (N = 180) on sociodemographic and moderating variables, and frequency of past DWI convictions indicated no significant differences. Comparisons on these measures between the original study cohort and (i) the 11 participants lost to long-term follow-up and (ii) the 7 participants added in the current study but excluded from the initial study also indicated no significant differences.
General Description of the Current Sample
Participants were mostly men (89.4%), with a mean age in the mid-40s. They were followed up for a mean of 1,684.5 days (SD = 155.7), with a minimum of 1,421 days (3.8 years) for those recruited last into the protocol to a maximum of 1,995 days (5.5 years) for those recruited first. For analysis, age was recoded into tertile categories with the first tertile consisting of an age range from 26.4 to 42.8 years (M = 36.1, SD = 4.4, n = 60), the second from 42.9 to 49.5 years (M = 45.6, SD = 1.8, n = 60), and the third from 49.6 to 64.8 years (M = 55.0, SD = 3.9, n = 60). For the AUDIT, the first tertile ranged up to 17 (M = 12.3, SD = 3.4, n = 62), the second from 18 to 24 (M = 20.7, SD = 1.9, n = 56), and the third from 25 to 40 (M = 30.6, SD = 4.1, n = 62). For intervention refractoriness, the first tertile included offenders with 2 convictions (36.1%, n = 65), the second included 3 convictions (28.9%, n = 52), and the third ranged from 4 to 15 convictions (35.0%, n = 63). Table1 presents demographics at baseline and number of postintervention arrests and crashes of BMI and CTL groups.
Table 1.
Demographics at Baseline and Number of Postintervention Arrests/Convictions and Crashes by Group (Brief Motivational Interviewing [BMI], n = 85 and Control [CTL], n = 95)
| BMI | CTL | |||
|---|---|---|---|---|
| M (%) | SD | M (%) | SD | |
| Demographics | ||||
| Age | 45.9 | 9.0 | 45.2 | 8.0 |
| Male gender | (94.1) | (85.3) | ||
| Education (years) | 12.7 | 2.9 | 13.4 | 2.8 |
| Currently cohabiting | (18.8) | (20.0) | ||
| Annual revenuea | ||||
| $0 to 11,999 | (29.4) | (29.8) | ||
| $12,000 to $29,999 | (34.1) | (29.8) | ||
| $30,000 to $49,999 | (24.7) | (30.8) | ||
| ≥$50,000 | (11.8) | (9.6) | ||
| Full-time or regular part-time employment | (51.7) | (50.6) | ||
| Traffic arrests/convictions and crashes | ||||
| % With at least 1 arrest | (24.7) | (27.4) | ||
| % With at least 1 DWI arrest | (8.3) | (11.6) | ||
| % With at least 1 crash | (4.7) | (6.3) | ||
DWI, driving while impaired.
For CTL, n = 94.
Arrests
Initial descriptive analysis revealed that an arrest resulting in conviction occurred in 47 participants (26.1%) over the follow-up period in the full sample, 24.7% of participants within group BMI and 27.4% of participants within group CTL. Mean time to the first arrest was 1,381.3 days (95% confidence interval [CI] = 1,261.8, 1,500.8) for group BMI and 1,357.9 days (95% CI = 1,235.3, 1,470.4) for group CTL. Figure1 depicts cumulative survival function to the first event across both groups. Initial analysis was carried out to detect a main effect of group in predicting survival time. Cox proportional hazards modeling detected no significant main effect for group ( = 0.17, p = 0.68) in prediction of time to arrest.
= 0.17, p = 0.68) in prediction of time to arrest.
Figure 1.
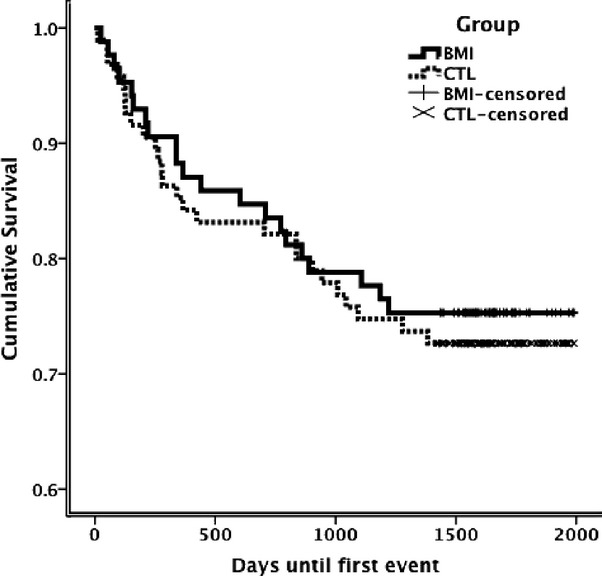
Cumulative survival in days to a first arrest/conviction for driving while impaired, speeding, or other moving traffic violation by group (brief motivational interviewing [BMI], n = 85 and Control [CTL], n = 95).
Of the different moderators tested, and after accounting for both group and age ( = 0.81, p = 0.81), the group–age category interaction added significantly to prediction of time to arrest (
= 0.81, p = 0.81), the group–age category interaction added significantly to prediction of time to arrest ( = 10.53, p = 0.005). Table2 summarizes mean days to an arrest for DWI, speeding, or other moving traffic violations and 95% CI of participants for groups BMI and CTL stratified by age tertiles. In the youngest age tertile (26.4 to 42.8 years of age), time to arrest was significantly predicted by group (
= 10.53, p = 0.005). Table2 summarizes mean days to an arrest for DWI, speeding, or other moving traffic violations and 95% CI of participants for groups BMI and CTL stratified by age tertiles. In the youngest age tertile (26.4 to 42.8 years of age), time to arrest was significantly predicted by group ( = 7.80, p = 0.005, hazard ratio = 4.93, 95% CI = 1.39, 17.51). Figure2 depicts the cumulative survival curves in this age tertile. Analyses revealed no significant effect of group in predicting time to arrest in the second (
= 7.80, p = 0.005, hazard ratio = 4.93, 95% CI = 1.39, 17.51). Figure2 depicts the cumulative survival curves in this age tertile. Analyses revealed no significant effect of group in predicting time to arrest in the second ( = 2.30, p = 0.13) or third (
= 2.30, p = 0.13) or third ( = 0.31, p = 0.58) age tertile categories. No significant moderation effects were found for readiness to change, alcohol misuse severity, or past convictions.
= 0.31, p = 0.58) age tertile categories. No significant moderation effects were found for readiness to change, alcohol misuse severity, or past convictions.
Table 2.
Mean Days and 95% Confidence Intervals (CI) Until a First Arrest Leading to Conviction for Driving While Impaired (DWI), Speeding, or Other Moving Violations by Age Tertile and Group (Brief Motivational Interviewing [BMI], n = 85 and Control [CTL], n = 95)
| Group | n | Mean days | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age tertiles | |||||
| 1st: 26.4 to 42.8 years | BMI | 30 | 1,581.0 | 1,447.3 | 1,714.7 |
| CTL | 30 | 1,188.6 | 942.4 | 1,434.9 | |
| 2nd: 42.9 to 49.5 years | BMI | 24 | 1,159.6 | 896.1 | 1,423.1 |
| CTL | 36 | 1,402.3 | 1,203.7 | 1,600.8 | |
| 3rd: 49.6 to 64.8 years | BMI | 31 | 1,359.7 | 1,140.5 | 1,579.0 |
| CTL | 29 | 1,458.2 | 1,282.6 | 1,633.7 | |
Figure 2.
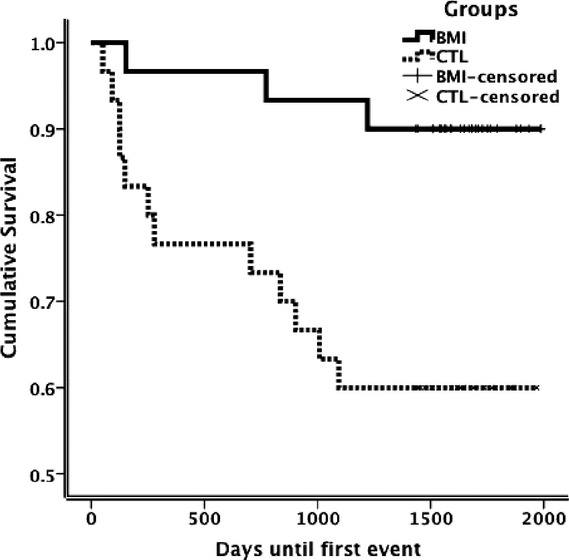
Cumulative survival of participants in first age tertile (26.4 to 42.8 years of age) in days to a first arrest/conviction for driving while impaired, speeding, or other moving traffic violation by group (brief motivational interviewing [BMI], n = 85 and Control [CTL], n = 95).
Crashes
Ten participants were involved in a documented crash (5.6%) over the follow-up period, 4 (4.7%) in group BMI and 6 (6.3%) in group CTL. Mean time to the first crash for participants in groups BMI and CTL were 1,630.1 days (95% CI = 1,567.2, 1,693.1) and 1,606.2 days (95% CI = 1,536.0, 1,676.4), respectively. Group differences or moderation effects were not detected.
Discussion
The present study investigated the outcomes of DWI recidivists randomly assigned to receive either BMI or CTL intervention. Follow-up durations ranged from a minimum of approximately 4 years to a maximum of over 5 years. The main finding was that while group membership alone was not associated with significantly different outcomes across all participants, better outcome with exposure to BMI compared with CTL was uncovered when the effect of age was accounted for: that is, a significantly longer delay in a subsequent conviction for DWI, speeding, or another moving traffic violation was found in the youngest offenders exposed to BMI compared with CTL. As such, BMI is more advantageous in delaying convictions for offenses associated with DWI recidivism status in a particularly at-risk group, namely younger drivers.
This study is unique among the rare investigations evaluating BMI for DWI (for review, see McMurran, 2009) for its combination of randomized controlled trial methodology, length of follow-up, use of objective documented outcome indicators, and recruitment of a naturalistic, nonclinical sample potentially more akin to the DWI recidivist population than undertaken in previous studies. These distinctions also mean that direct comparisons between this study and most previous ones must be undertaken cautiously. Nevertheless, 2 well-controlled studies with random assignment and objective long-term outcomes (i.e., DWI reconviction events) explored the effect of exposure to BMI variants versus no exposure, one with imprisoned DWI offenders and a 24-month follow-up period (Woodall et al., 2007) and the other with DWI remedial program participants and a 6-year follow-up period (Wells-Parker and Williams, 2002). Both studies failed to reject the null hypothesis for a main effect of intervention exposure. In 2 other investigations, however, an effect of BMI exposure was detected. A randomized controlled study with incarcerated adolescents (Stein et al., 2006) found that those exposed to BMI had reduced DWI behavior over a 3-month follow-up period, although its short-term follow-up and reliance on self-report are important methodological shortcomings. The other study (Marques et al., 1999) looked at an objective indicator of elevated blood alcohol levels via alcohol interlock devices installed in the vehicles of convicted offenders for up to a 2-year follow-up duration. It found that offenders from a city where BMI was provided in addition to interlock installation had fewer positive blows than offenders from a city where BMI was not provided. This study more objectively assessed DWI behavior than the Stein and colleagues' (2006) investigation. At the same time, its findings were also potentially confounded by its quasi-experimental methodology and sampling limited to the minority of offenders willing to volunteer for participation in an interlock program. No other studies to our knowledge have explored the impact of BMI on crashes. Overall, when considering heterogeneous samples of DWI offenders and longer-term outcomes, the strongest evidence suggests that exposure to BMI is not more advantageous than a CTL in reducing reconvictions and crashes.
Analyses to discern moderation of effects by participant characteristics on outcome revealed a more nuanced impact of BMI. Understanding characteristics of individuals most apt to benefit from treatment is of enduring clinical and research interest in the substance abuse field. Some selective responsivity in younger individuals to common DWI interventions has been reported (Brown et al., 2012; Wells-Parker et al., 1989). Nevertheless, aside from a few notable exceptions (Wells-Parker and Williams, 2002), subgroup analyses looking at long-term effects of BMI on DWI and other risky driving behavior are rare. Investigation of age-related moderation in BMI's effectiveness in the more extensive substance abuse literature has yielded mixed results regarding substance use outcomes (Foxcroft et al., 2002; Mallett et al., 2010; McCambridge and Strang, 2005). The present findings extend previous support for BMI (Dill et al., 2004; D'Onofrio and Degutis, 2004; Monti et al., 1999) as an appropriate brief intervention strategy for achieving reductions in DWI and other risky driving behavior in younger offenders. More research is needed to understand why BMI is selectively advantageous for younger client groups.
Clinical Implications
In considering the implications of the findings to applied settings, several features of the present study are worth noting. Delivery of both interventions was manualized and highly controlled for fidelity, including the use of the Motivational Interviewing Treatment Integrity protocol (Moyers et al., 2005) and an iterative supervision procedure (for details, see Brown et al., 2010). This level of control is not likely to be feasible in most of the applied settings. Moreover, mandated DWI relicensing programs represent a unique set of conditions and therapeutic challenges (Lapham et al., 2006) and are characterized by the frequent simultaneous use of remedial and deterrence strategies. These distinctions underscore the well-established gap between data garnered from efficacy studies and their real-world deployment. Despite these caveats, the results of the present study, based on a very brief delivery format and a sample of non-help-seeking DWI recidivists, lend support for BMI's potential as an intervention that could be opportunistically and advantageously deployed in settings where younger non-help-seeking DWI offenders are encountered (e.g., emergency rooms, court settings soon after an arrest, frontline health settings). Confirmation of its benefits for reducing driving risks when embedded into these and other specific contexts (e.g., mandated relicensing programs) awaits further effectiveness research.
Limitations
Limits in the generalizability of the findings to mandated DWI remedial programs have been noted above. Arrests/convictions and crashes are rare events (Beitel et al., 2000), a problem that vexes the orchestration of controlled studies in the area (Dill and Wells-Parker, 2006). Measurement of these phenomena would benefit from a much larger sample to better power and stabilize the analyses. Replication of this study using larger samples is warranted to confirm the results. In addition, several local factors may influence convictions for DWI, speeding, or other moving traffic violations, including enforcement rigor and legal dispositions. As a result, the findings may not be readily generalizable to offenders from jurisdictions with significantly different approaches to DWI deterrence and intervention from those in force in the province of Quebec.
Conclusion
In at-risk younger drivers, BMI was more advantageous for reducing DWI and other dangerous traffic violations over a 5-year duration than an intervention similar to that provided in many contemporary remedial programs.
Acknowledgments
This study was supported by grants from the ABMRF/The Foundation for Alcohol Research, the Canadian Institutes of Health Research Team in transdisciplinary studies in DWI onset, persistence, prevention and treatment, the Canadian Psychiatric Research Foundation, and start-up funding from the McGill-Dongier Endowment for Addiction Research. MCO was supported through a career award from the Quebec Health Research Fund (Fonds de recherche du Québec— Santé) and TGB by a career award from the Quebec Council for Research into Society and Culture (now Fonds de recherche du Québec—Société et Culture). The authors would like to thank Edwin Cheung for help in processing the data for this manuscript and Lyne Vézina and François Tardif of the Quebec Licensing and Insurance Bureau (Société de l'assurance automobile du Québec) for compiling participants' driving records to the research team.
References
- Anderson P, Chisholm D, Fuhr DC. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet. 2009;373:2234–2246. doi: 10.1016/S0140-6736(09)60744-3. [DOI] [PubMed] [Google Scholar]
- Beitel GA, Sharp MC, Glauz WD. Probability of arrest while driving under the influence of alcohol. Inj Prev. 2000;6:158–161. doi: 10.1136/ip.6.2.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown TG, Dongier M, Ouimet MC, Tremblay J, Chanut F, Legault L, Ng Ying Kin NMK. Brief motivational interviewing for DWI recidivists who abuse alcohol and are not participating in DWI intervention: a randomized controlled trial. Alcohol Clin Exp Res. 2010;34:292–301. doi: 10.1111/j.1530-0277.2009.01092.x. [DOI] [PubMed] [Google Scholar]
- Brown TG, Dongier M, Ouimet MC, Tremblay J, Chanut F, Legault L, Ng Ying Kin NMK. The role of demographic characteristics and readiness to change in 12-month outcome from two distinct brief interventions for impaired drivers. J Subst Abuse Treat. 2012;42:383–391. doi: 10.1016/j.jsat.2011.09.009. [DOI] [PubMed] [Google Scholar]
- Brown TG, Ouimet MC. Treatments for alcohol-related impaired driving. In: McMurran M, editor. Alcohol-Related Violence: Prevention and Treatment. Chichester: John Wiley & Sons Ltd; 2012. pp. 303–334. [Google Scholar]
- Brown TG, Ouimet MC, Nadeau L, Lepage M, Tremblay J, Dongier M, Ng Ying Kin NMK. DUI offenders who delay relicensing: a quantitative and qualitative investigation. Traffic Inj Prev. 2008;9:109–118. doi: 10.1080/15389580801907908. [DOI] [PubMed] [Google Scholar]
- C'de Baca J, Lapham SC, Liang HC, Skipper BJ. Victim impact panels: do they impact drunk drivers? A follow-up of female and male, first-time and repeat offenders. J Stud Alcohol. 2001;62:615–620. doi: 10.15288/jsa.2001.62.615. [DOI] [PubMed] [Google Scholar]
- C'de Baca J, McMillan GP, Lapham SC. Repeat DUI offenders who have had a drug diagnosis: are they more prone to traffic crashes and violations? Traffic Inj Prev. 2009;10:134–140. doi: 10.1080/15389580802593202. [DOI] [PubMed] [Google Scholar]
- Chanut F, Dongier M, Legault L, Tremblay J, Nadeau L, Ouimet MC, Brown TG. Étude pilote de l'entretien motivationnel chez des personnes condamnées pour conduite avec facultés affaiblies [Motivational Interviewing with DUI offenders: a pilot study] Drogues Santé Société. 2007;6:83–115. [Google Scholar]
- Conley TB. Construct validity of the MAST and AUDIT with multiple offender drunk drivers. J Subst Abuse Treat. 2001;20:287–295. doi: 10.1016/s0740-5472(01)00159-3. [DOI] [PubMed] [Google Scholar]
- Dill PL, Wells-Parker E. Court-mandated treatment for convicted drinking drivers. Alcohol Res Health. 2006;29:41–48. [PMC free article] [PubMed] [Google Scholar]
- Dill PL, Wells-Parker E, Soderstrom CA. The emergency care setting for screening and intervention for alcohol use problems among injured and high-risk drivers: a review. Traffic Inj Prev. 2004;5:278–291. doi: 10.1080/15389580490465364. [DOI] [PubMed] [Google Scholar]
- D'Onofrio G, Degutis LC. Screening and brief intervention in the emergency department. Alcohol Res Health. 2004;28:63–72. [PMC free article] [PubMed] [Google Scholar]
- Donovan DM. Driving while intoxicated: different roads to and from the problem. Crim Justice Behav. 1989;16:270–298. [Google Scholar]
- Dunn C, Deroo L, Rivara FP. The use of brief interventions adapted from motivational interviewing across behavioral domains: a systematic review. Addiction. 2001;96:1725–1742. doi: 10.1046/j.1360-0443.2001.961217253.x. [DOI] [PubMed] [Google Scholar]
- Elder RW, Nichols JL, Shults RA, Sleet DA, Barrios LC, Compton R. Effectiveness of school-based programs for reducing drinking and driving and riding with drinking drivers: a systematic review. Am J Prev Med. 2005;28:288–304. doi: 10.1016/j.amepre.2005.02.015. [DOI] [PubMed] [Google Scholar]
- Foxcroft D, Ireland D, Lowe G, Breen R. Primary prevention for alcohol misuse in young people. Cochrane Database Syst Rev. 2002;3:CD003024. doi: 10.1002/14651858.CD003024. [DOI] [PubMed] [Google Scholar]
- Freeman J, Liossis P, Schonfeld C, Sheehan M, Siskind V, Watson B. Self-reported motivations to change and self-efficacy levels for a group of recidivist drink drivers. Addict Behav. 2005;30:1230–1235. doi: 10.1016/j.addbeh.2004.10.007. [DOI] [PubMed] [Google Scholar]
- Heather N, Rollnick S, Bell A. Predictive validity of the Readiness to Change Questionnaire. Addiction. 1993;88:1667–1677. doi: 10.1111/j.1360-0443.1993.tb02042.x. [DOI] [PubMed] [Google Scholar]
- Heather N, Rollnick S, Bell A, Richmond R. Effects of brief counselling among male heavy drinkers identified on general hospital wards. Drug Alcohol Rev. 1996;15:29–38. doi: 10.1080/09595239600185641. [DOI] [PubMed] [Google Scholar]
- Jonah BA, Thiessen R, Au-Yeung E. Sensation seeking, risky driving and behavioral adaptation. Accid Anal Prev. 2001;33:679–684. doi: 10.1016/s0001-4575(00)00085-3. [DOI] [PubMed] [Google Scholar]
- Lapham SC, C'de Baca J, Chang I, Hunt WC, Berger LR. Are drunk-driving offenders referred for screening accurately reporting their drug use? Drug Alcohol Depend. 2002;66:243–253. doi: 10.1016/s0376-8716(02)00004-2. [DOI] [PubMed] [Google Scholar]
- Lapham SC, Kapitula LR, C'de Baca J, McMillan GP. Impaired-driving recidivism among repeat offenders following an intensive court-based intervention. Accid Anal Prev. 2006;38:162–169. doi: 10.1016/j.aap.2005.08.009. [DOI] [PubMed] [Google Scholar]
- Mallett KA, Ray AE, Turrisi R, Belden C, Bachrach RL, Larimer ME. Age of drinking onset as a moderator of the efficacy of parent-based, brief motivational, and combined intervention approaches to reduce drinking and consequences among college students. Alcohol Clin Exp Res. 2010;34:1154–1161. doi: 10.1111/j.1530-0277.2010.01192.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marques PR, Voas RB, Tippetts AS, Beirness DJ. Behavioral monitoring of DUI offenders with the Alcohol Ignition Interlock Recorder. Addiction. 1999;94:1861–1870. doi: 10.1046/j.1360-0443.1999.9412186111.x. [DOI] [PubMed] [Google Scholar]
- McCambridge J, Strang J. Deterioration over time in effect of motivational interviewing in reducing drug consumption and related risk among young people. Addiction. 2005;100:470–478. doi: 10.1111/j.1360-0443.2005.01013.x. [DOI] [PubMed] [Google Scholar]
- McMurran M. Motivational interviewing with offenders: a systematic review. Leg Crim Psychol. 2009;14:83–100. [Google Scholar]
- Meyer J, Gray T. Drunk drivers in the courts: legal and extra-legal factors affecting pleas and sentences. J Crim Justice. 1997;25:155–163. [Google Scholar]
- Miller WR. Motivational interviewing: research, practice, and puzzles. Addict Behav. 1996;21:835–842. doi: 10.1016/0306-4603(96)00044-5. [DOI] [PubMed] [Google Scholar]
- Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol. 2009;64:527–537. doi: 10.1037/a0016830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monti PM, Colby SM, Barnett NP, Spirito A, Rohsenow DJ, Myers M, Woolard R, Lewander W. Brief intervention for harm reduction with alcohol-positive older adolescents in a hospital emergency department. J Consult Clin Psychol. 1999;67:989–994. doi: 10.1037//0022-006x.67.6.989. [DOI] [PubMed] [Google Scholar]
- Moyers TB, Martin T, Manuel JK, Hendrickson SM, Miller WR. Assessing competence in the use of motivational interviewing. J Subst Abuse Treat. 2005;28:19–26. doi: 10.1016/j.jsat.2004.11.001. [DOI] [PubMed] [Google Scholar]
- Nochajski TH, Stasiewicz PR. Relapse to driving under the influence (DUI): a review. Clin Psychol Rev. 2006;26:179–195. doi: 10.1016/j.cpr.2005.11.006. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol. 1992;47:1102–1114. doi: 10.1037//0003-066x.47.9.1102. [DOI] [PubMed] [Google Scholar]
- Rauch WJ, Zador PL, Ahlin EM, Howard JM, Frissell KC, Duncan GD. Risk of alcohol-impaired driving recidivism among first offenders and multiple offenders. Am J Public Health. 2010;100:919–924. doi: 10.2105/AJPH.2008.154575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saunders JB, Aasland OG, Babor TF, De La Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- Simpson HM, Beirness DJ, Robertson RD, Mayhew DR, Hedlund JH. Hard core drinking drivers. Traffic Inj Prev. 2004;5:261–269. doi: 10.1080/15389580490465355. [DOI] [PubMed] [Google Scholar]
- Smedslund G, Berg RC, Hammerstrom KT, Steiro A, Leiknes KA, Dahl HM, Karlsen K. Motivational interviewing for substance abuse. Cochrane Database Syst Rev. 2011;5:CD008063. doi: 10.1002/14651858.CD008063.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein LA, Colby SM, Barnett NP, Monti PM, Golembeske C, Lebeau-Craven R. Effects of motivational interviewing for incarcerated adolescents on driving under the influence after release. Am J Addict. 2006;15(Suppl 1):50–57. doi: 10.1080/10550490601003680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Timko C, Desai AV, Blonigen DM, Moos BS, Moos RH. Driving while intoxicated among individuals initially untreated for alcohol use disorders: one- and sixteen-year follow-ups. J Stud Alcohol. 2011;72:173–184. doi: 10.15288/jsad.2011.72.173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanlaar W, Robertson R, Marcoux K, Mayhew D, Brown S, Boase P. Trends in alcohol-impaired driving in Canada. Accid Anal Prev. 2012;48:297–302. doi: 10.1016/j.aap.2012.01.030. [DOI] [PubMed] [Google Scholar]
- Voas RB, Fisher DA. Court procedures for handling intoxicated drivers. Alcohol Res Health. 2001;25:32–42. [PMC free article] [PubMed] [Google Scholar]
- Voas RB, Tippetts SS, Fisher D, Grosz M. Requiring suspended drunk drivers to install alcohol interlocks to reinstate their licenses: effective? Addiction. 2010a;105:1422–1428. doi: 10.1111/j.1360-0443.2010.02987.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Voas RB, Tippetts AS, McKnight AS. DUI offenders delay license reinstatement: a problem? Alcohol Clin Exp Res. 2010b;34:1282–1290. doi: 10.1111/j.1530-0277.2010.01206.x. [DOI] [PubMed] [Google Scholar]
- Wells-Parker E, Anderson BJ, McMillen DL, Landrum JW. Interactions among DUI offender characteristics and traditional intervention modalities: a long-term recidivism follow-up. Br J Addict. 1989;84:381–390. doi: 10.1111/j.1360-0443.1989.tb00581.x. [DOI] [PubMed] [Google Scholar]
- Wells-Parker E, Williams M. Enhancing the effectiveness of traditional interventions with drinking drivers by adding brief individual intervention components. J Stud Alcohol. 2002;63:655–664. doi: 10.15288/jsa.2002.63.655. [DOI] [PubMed] [Google Scholar]
- Wells-Parker E, Williams M, Dill P, Kenne D. Stages of change and self-efficacy for controlling drinking and driving: a psychometric analysis. Addict Behav. 1998;23:351–363. doi: 10.1016/s0306-4603(97)00077-4. [DOI] [PubMed] [Google Scholar]
- Williams SB, Whitlock EP, Edgerton EA, Smith PR, Beil TL. Counseling about proper use of motor vehicle occupant restraints and avoidance of alcohol use while driving: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2007;147:194–206. doi: 10.7326/0003-4819-147-3-200708070-00009. [DOI] [PubMed] [Google Scholar]
- Witkiewitz K, Hartzler B, Donovan D. Matching motivation enhancement treatment to client motivation: re-examining the Project MATCH motivation matching hypothesis. Addiction. 2010;105:1403–1413. doi: 10.1111/j.1360-0443.2010.02954.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodall WG, Delaney HD, Kunitz SJ, Westerberg VS, Zhao H. A randomized trial of a DWI intervention program for first offenders: intervention outcomes and interactions with antisocial personality disorder among a primarily American-Indian sample. Alcohol Clin Exp Res. 2007;31:974–987. doi: 10.1111/j.1530-0277.2007.00380.x. [DOI] [PubMed] [Google Scholar]