

Abstract
Background
Cervical cancer is the third most common cancer in women in the world. Papanicolaou smear is known as a standard test for cervical cancer screening; however, the most important challenge is high rates of false negative results. The aim of this study was to compare the quality of smears obtained by anatomical spatula and spatula-cytobrush. The most important factor in false negative result is inappropriate tool of sampling.
Methods
One hundred married women participated in this single blind clinical trial. All participants were interviewed; two samples were obtained from every participant: one with spatula-cytobrush and another one with anatomical spatula. All slides were encoded and were assessed by two pathologists. Then, data were analyzed by means of kappa coefficient.
Results
Cell adequacy was 96.1 % in anatomical spatula method and 91.2 % in spatula-cytobrush method (p= 0.016). The rates for endocervical cells and metaplasia cells in anatomical spatula method were 70.6% and 24.5% respectively and these amounts were 69.6% and 24.5% respectively in the spatula-cytobrush method (p <0.001). No one reported any pain and the amount of bleeding was 38.2% in both methods (P>0.05). Regarding infection and inflammatory reactions there was no statistically significant difference between two methods (p>0.05).
Conclusion
Based on our findings in this study, results of sampling with anatomical spatula method were more acceptable and better than those with spatula-cytobrush sampling.
Keywords: Papanicolaou smear, Cervical neoplasm, Clinical trial
Introduction
Sixty years ago cervical cancer was the main cause of death in women. Currently in Iran estimates indicate that every year 1118 women are diagnosed with cervical cancer and 581 die from the disease. Cervical cancer ranks as the 5th most frequent cancer in Iranian women, and the 5th most frequent cancer among women between 15 and 44 years of age [1]. However, in Southern Asia, the region which is Iran belongs to, about 6.6% of women in general population are estimated to have cervical HPV infection, and 71.2% of invasive cervical cancers are attributed to HPVs 16 or 18. Mortality due to cervical cancer has been reduced by 50% since then. The decrease is because of development and use of a cytologic screening tool known as Papanicolaou smear [2, 3]. Unfortunately, by using traditional methods, false negative results are high (56% cases) due to not having enough endocervical cells. As a result of false negative reports, the disease is not diagnosed early, so it develops to advanced malignancy which eventually increases morbidity and mortality rates [4].
Several factors contribute to the incidence of false negative cases. These factors include sampling error (inappropriate and insufficient sample), use of inappropriate tools for sampling, and error in laboratory reports [5]. Therefore, use of correct tool to prepare the Papanicolaou smear, can reduce false negative results, although insufficient sampling should be taken into account.
In 1991 Suzaly spatula was introduced to the world [6, 7]. This kind of spatula has special advantages for examples it can decrease in number of false negative results because of making enough sample from endocervix, exocervix and transitional zone; sample taking with such device is very easy and sample is taken once from endocervix and exocervix instead of twice sampling; spreading sample on slide is very easy and can be done in one step instead of twice pulling on slides; infection rate is low due to one step sampling; anatomical spatula tab is slender and similar to cervix canal so it can use in females with longer cervical canal; cervical bleeding rate in women with fragile cervix is low because of one step sampling; pathology report is more accurate because samples are less bloody and have enough cells on the slide spread on a thin layer [7].
Therefore, in this study, we determined to compare the quality of slides after sampling with both anatomical spatula and spatula-cytobrush. Anatomical spatula used in this study was the same as Suzaly spatula that embodies the above-mentioned advantages. We hypothesized that this tool would be suitable for Papanicolaou smear, might have economical benefits and could help find hidden cases of cervical malignancy.
Materials and Methods
The present study was a single blind clinical trial in which 100 women were recruited at the outpatient Academic Medical Center in Zeynabiyeh Hospital in Shiraz, Iran, during 2009. The Medical Research Ethics Committee of Shiraz University of Medical Sciences approved the trial protocol before study. Informed consent was obtained through the provision of an information leaflet coupled with verbal reassurance that participation was entirely voluntary. In addition all participants were assured of confidentially and anonymity.
We used two different types of tools in order to take samples from cervix.
Anatomical spatula is a wooden piece with length of 220 mm and width of 5 mm. This spatula has a long narrow arm with a length of 1.7 cm for sampling from endocervix, a shoulder and a completely flat curve for exocervical sampling and because of its anatomic structure is more compatible with women cervix. The arm of the spatula is placed inside the canal whilst its shoulder is on 3 o’clock position in exocervix. With gentle pressure, the spatula should be rotated in a clockwise direction through 360 degrees. Once the cells are spread on the slide, they are parallel to the slide edges and the slide is immediately fixed in a distance about 30 cm (Figure1).
Figure 1.
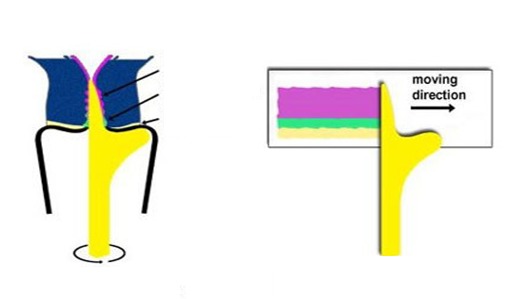
Sample taking and spreading on slide with anatomical spatula
In the common method using cytobrush spatula, first the brush is put into the cervix and is rotated round 360 degrees in a clockwise direction. Then the upper slide is moved so that the brush is drawn on the glass. Then spatula wide head is put on exocervix and with 360 degrees rotation sample is taken from exocervix then pulled in the lower part of slide and is fixed for 30 cm with a fixator.
Women aged 18 and older who attended regular cervical cancer screenings were enrolled in the study using convenience sampling. Their demographic data were gathered before samples. The following procedure was designed in order to take two cervical samples from each participant:
First, every participant lied down on a gynecology bed in lithotomic position and vaginal speculum was inserted. A sterile cotton swab was used to wipe excessive cervical discharge and mucosa. Cervical smears were taken from both endocervix and exocervix by two kinds of spatula. For the first participant we used cytobrush spatula at first and then anatomical spatula but for the second participant we applied firstly anatomical spatula and then cytobrush spatula. We followed this pattern alternately until all participants had two samples either cytobrush spatula- anatomical spatula or anatomical spatula- cytobrush spatula. The slides were labelled by the researcher as 1a, 1b (for the first participant), 2b, 2a (for the second participant), 3a, 3b (for the third participant), etc.
The researcher was the only person who was in charge of taking samples and knew the codes. Two hundred slides were sent out to laboratory to be assessed by two pathologists who were not aware of the order of sampling and did not know which sample was belonged to which tool. The results were based on the Bethesda system.
Data analysis was carried out using SPSS version15 for Windows. We used descriptive statistics in order to summarize demographic data. The kappa was used to compare the results of the two sampling tools.
Cytobrush spatula.
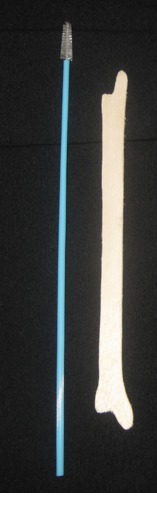
Anatomical spatula.

Results
In this study, no cell samples were returned from laboratory because all slides were satisfactory. The mean age was 30.58 ± 8.4 years ranging from 16 to 55 years. Most prevalent contraceptives used by participants were OCP (29.4%), IUD (22.5%), condom (20.8%), vasectomy (10%) and tubectomy (10%).
Smears obtained by anatomical spatula had better cellular adequacy, however, there was no statistically significant difference between methods (96.1% in anatomical spatula method and 91.2% in spatula-cytobrush) (p =0.16) (Table 1).
Table 1.
Comparison of the distribution and adequacy of cellular anatomical spatula and spatula-cytobrush
| Method | Anatomical spatula | Spatula-cytobrush | p-value | ||
|---|---|---|---|---|---|
| Cellular adequacy | Number | Percent | Number | Percent | |
| Highly Satisfactory | 89 | 96.1 | 93 | 91.2 | 0.16 |
| Moderately satisfactory | 7 | 6.9 | 2 | 2 | |
In anatomical method the percentage of endocervical cells and metaplastic cells were similar to spatula-cytobrush, and their differences were not significant (p 0.06) (Table 2).
Table 2.
Distribution of endocervical cells in the two methods of sampling.
| Method | Anatomical spatula | Spatula-cytobrush | p-value | ||
|---|---|---|---|---|---|
| Cell | Number | Percent | Number | Percent | |
| Endocervical cells | 72 | 70.6 | 71 | 69.6 | 0.06 |
| Metapelastic cells | 25 | 24.5 | 25 | 24.5 | |
The rates of discovered cellular infection and inflammation were similar in both methods (p>0.05 between methods). Almost 6% of participant were infected with Candida Albicans (p>0.05 among methods), and 38% of samples were diagnosed with inflammation in each method (p>0.05 among methods) (Table 3).
Table 3.
Distribution of cellular infection and inflammations in both methods of sampling.
| Method | Anatomical spatula | Spatula-cytobrush | p-value | ||
|---|---|---|---|---|---|
| Cellular phenomenon | Number | Percent | Number | Percent | |
| No infection | 91 | 89.2 | 90 | 70 | 0.07 |
| Infection | 6 | 5.9 | 7 | 6.9 | |
| No inflammation | 56 | 54.9 | 57 | 55.9 | 0.083 |
| Inflammation | 39 | 38.2 | 39 | 38.2 | |
Although slides which were prepared with anatomical spatula had a higher resolution, there was no significant difference between the slides in both methods which had the same quality and showed the same cells (Figure 2 and Figure 3).
Figure 2.
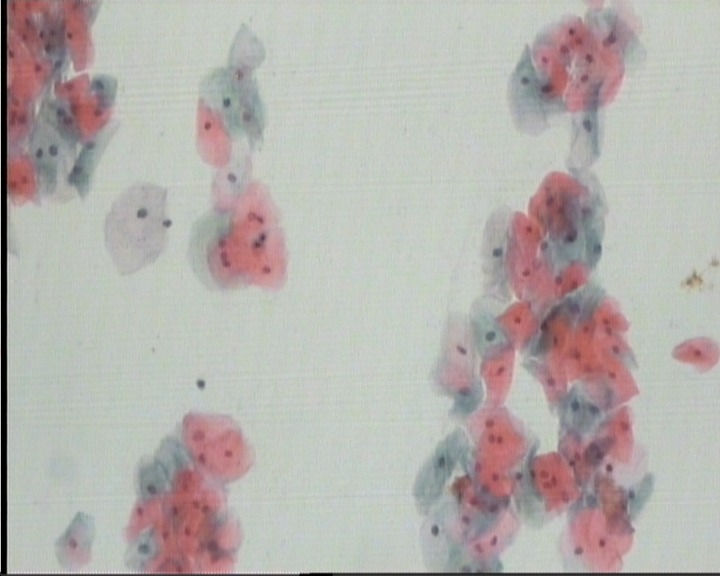
Resolution of cells in sampling with anatomical spatula
Figure 3.
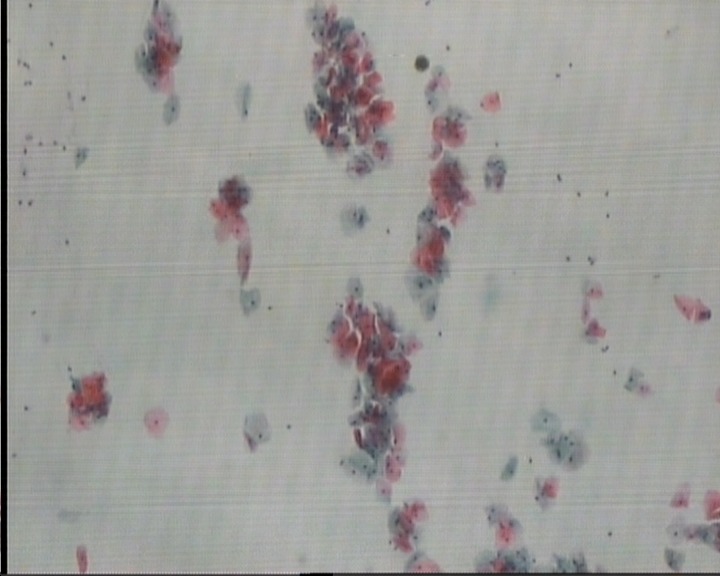
Resolution of cells in sampling with spatula- cytobrush
No pain was reported during taking samples with either anatomical spatula or spatula-cytobrush. Bleeding occurred during taking samples in women with moderate to severe cervicitis, and it was similar in both methods (p>0.05). None of the slides was reported by pathologists to be bloody sample and/or unsatisfactory (Figure 4 and Figure 5).
Figure 4.
The slide stained with blood in sampling with anatomical spatula
Figure 5.
The slide stained with blood in sampling with spatula-cytobrush
Fortunately, none of the samples was reported to have malignant epithelial cells, Atypical Squamous Cells of Undetermined Significance (ASCUS), and/or Cervical Intraepithelial Neoplasia (CIN).
Discussion
Cervical cancer starts invading from cervical transitional zone. In order to take appropriate sample from the transitional zone cells, health care provider needs appropriate sampling device. The results of current study demonstrated that similar results can be obtained from samples taken by anatomical spatula as well as spatula-cytobrush. It was shown that anatomical spatula is a one-step technique which enables physicians to take easily enough endocervix cylindrical cells, exocervix squamous cell, and transitional zone cell.
In a meta-analysis study, cytobrush in accompany with spatula was reported to be the most effective Pap smear device to make high-quality smears and to detect cervical dysplasia [2]. It was shown in previous studies that spatula-cytobrush can be used as the best tool to detect pre-cancerous cells [8].
Another meta-analysis reported that cytobrush alone cannot be a suitable method of sampling from exocevical cells so it should be used along with sharp spatula (Suzaly spatula) [9].
In the current trial, both anatomical spatula and spatula-cytobrush demonstrated similar results. We showed that anatomical spatula can be used alone in order to prepare cervical cell samples. Most studies have reported that smears with no endocevical cells are more likely to carry false negative results. Therefore, in order to minimize the number of false negative results, slides must contain enough squamous cells, transitional zone cells and endocervical cells [10-12]. In our study, 70.6% of smears taken with anatomical spatula contained endocervical cells whereas 69.6% of smears taken with spatula-cytobrush had endocervical cells showing that the possibility of false negative results was less in sampling with anatomical spatula compared to spatula-cytobrush.
Canon et al. compared the results of two methods of sampling with cervical brush and plastic Suzaly spatula showing that the rates of endocervical cells were 90.7% and 98.5% respectively. As smears with endocervical cells are more likely to determine early stage of cervical cancer and Suzaly spatula collected more endocervical cells so it was more valuable to prepare better samples [13, 14].
In a study conducted by Rammou-Kinia et al.[11] the rate of endocervical cells in slides taken by Suzaly spatula were higher and false negative results were less. Moreover, they mentioned that inflammatory lesions, cervical epithelial neoplasia and squamous metaplasia were more likely to be detected by this tool [11].
They also showed that Suzaly spatula was very easy to use and was able to take enough cells from endocervix and exocervicx. Furthermore, they demonstrated that the amount of bleeding was very less and cell adequacy was very high with Suzaly spatula [13].
George et al. stated that slides which were fixed immediately after sampling had less false negative results than those which were exposed to the air and dried before fixation [13]. In the present study, we were able to fix smears taken by anatomical spatula faster than spatula-cytobrush because anatomical spatula was able to take both endo-and exocervical cells at the same time. After transferring cells on the slides, we have not taken another sample so we have fixed smears immediately. Therefore, there were less false negative results in smears taken by this device.
In another study, Noel explained that in women with cervical stenosis, spatula-cytobrush was a suitable device to collect samples from endocervix and also spatula-cytobrush was compared with sharp spatula and showing that in 64.8% of cases spatula-cytobrush was able to take cells from endocervical (p<0.001 among the two methods) [14]. The results of the present study showed that both anatomical spatula and spatula-cytobrush were able to take endocervical cells in 70.6% and 69.6% of cases respectively (p>0.05). These results showed that anatomical spatula is compatible with anatomy of cervix and is able to take enough endocervical cells.
As a result of our study using of anatomical spatula can be considered as a cheap and proper technique in compared to spatula-cytobrush. We concluded that our study had enough support as we used both methods of sampling in each participant; nevertheless, we have not generalized the results of our study to a large population. Further studies with more samples, more different participants, and random sampling are needed to make a decision to use this device as the most proper tool for Pap smear.
Conclusion
Based on our findings, cytology results with both anatomical spatula and spatula-cytobrush were similar, although, anatomical spatula was easier to use. Anatomical spatula was also associated with less pain and bleeding and can be used instead of spatula-cytobrush.
Acknowledgments
We would like to thank Mr. Sadeghi (Zainabiyeh Pathology Hospital) for his friendly cooperation. We also would like to express our sincere gratitude to the Research Deputy of Shiraz University of Medical Sciences for funding this study. The authors thank Faghihi Hospital Staff for their continuing support.
Footnotes
Conflicts of Interest
The authors have no conflict of interest in this article.
Authors' Contribution
KhA designed the study, MK reviewed and wrote the manuscript. PK and NRM reported the results and HRT analyzed the data.
REFERENCES
- 1.Castellsague X, De Sanjose S, Aguado T, Louie KS, Burni L, Munoz J, et al. HPV and cervical cancer in the world 2007 report. Vaccine. 2007;25(3):C1–230. [Google Scholar]
- 2.Bauman BJ. Use of a cervical brush for Papanicolaou smear collection.A meta-analysis. J Nurse Midwifery. 1993;38(5):267–73. doi: 10.1016/0091-2182(93)90105-p. [DOI] [PubMed] [Google Scholar]
- 3.George S, Abrahams Y, Karim SZ, Kothari A. Improving the quality of cervical screening. BJOG. 2004;111(9):960–6. doi: 10.1111/j.1471-0528.2004.00219.x. [DOI] [PubMed] [Google Scholar]
- 4.Aghajani Delavar M, Shafigh E, Mohamadpour RA. Comparison of cervix brush with spatula Ayer for obtaining endocervical cells. J Birjand University Med Sci. 2006;13(1):32–7. [Google Scholar]
- 5.Breek Jonathans. Breek and Novak,s Gynecology, translated by Velendan M. Nasle Farda. 2007;1:430–1. [Google Scholar]
- 6.Rammou-Kinia R, Anagnostopoulou I, Gomousa M. Comparison of spatula and nonspatula methods for cervical sampling. Acta cyto J. 1991;35(1):69–75. [PubMed] [Google Scholar]
- 7.The possibilities of minimizing the number of false – negative result with szalay – spatula Pap test collecting device [Internet]. 2008. Available from: http://www.csmgraf.ch.
- 8.Valenzuela P, Martinez P, Santana A, Garrido N, Cano A, Arnanz F. Comparison of cervical smears secured with different instruments. Acta Obestet Gynecol J. 2001;80(3):262–6. doi: 10.1034/j.1600-0412.2001.080003262.x. [DOI] [PubMed] [Google Scholar]
- 9.Buntinx F, Brouwers M. Relation between sampling device and detection of abnormality in cervical smears: a meta-analysis of randomised and quasi-randomised studies. BMJ. 1996;313(7068):1285–90. doi: 10.1136/bmj.313.7068.1285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Taheri Panah, Hashemi M, Dabirzade SH. Comparison of Ayer-spatula and cervix brush in menopause women. J OF Shahid Beheshti Medical Science. 2006;11(54):385–93. [Google Scholar]
- 11.Rammou-Kinia R, Anagnostopoulou I, Gomousa M. Comparison of spatula and nonspatula methods for cervical sampling. Acta cyto J. 1991;35(1):69–75. [PubMed] [Google Scholar]
- 12.Neinstein LS, Church J, Akiyoshi T. Comparison of cytobrush with cervex-brush for endocervical cytologic sampling. J Adolesent Health. 1992;13(6):520–3. doi: 10.1016/1054-139x(92)90017-6. [DOI] [PubMed] [Google Scholar]
- 13.Cannon JM, Blythe JG. Comparison of the cytobrush plus plastic spatula with the Cervix brush for obtaining endocervical cells. Obstet Gynecol . 1993;82(4 Pt 1):569–72. [PubMed] [Google Scholar]
- 14.Noel ML. Papanicolaou smear adequacy: the cervical cytobrush and Ayre spatula compared with the extended-tip spatula. J Am Board Fam Pract. 1989;2(3):156–60. [PubMed] [Google Scholar]