

Abstract
Objectives
Parents influence a child’s diet by modeling food choices, selecting the food they will make available, and controlling the child’s intake. Few studies have examined the covariation between parent’s behavior management practices and their guidance and support for a young child’s nutritional environment in early childhood. We hypothesized that parents’ positive behavior support (PBS), characterized as skillful behavior management and proactive structuring of children’s activities, would predict dietary quality over the course of early childhood (age 2 to 5 years), a critical period for the development of a dietary lifestyle through the lifespan.
Methods
Participants included 731 culturally diverse, low-income families in a randomized, controlled trial of the Family Check-Up. Families participated in a yearly home visit videotaped assessment when children were 2 to 5 years. PBS and dietary quality of meals parents served to their children were assessed by coding videotapes of structured parent–child interactions, including a meal preparation task. A cross-lagged panel model was used to evaluate the longitudinal relation between PBS and the dietary quality of meals served during the meal preparation task.
Results
Analyses revealed that PBS repeatedly predicted meals’ dietary quality the following year: age 2–3 (β = .30), age 3–4 (β = 0.14), age 4–5 (β = 0.37). Dietary quality significantly predicted PBS 1 year later: age 3–4 (β = 0.16), age 4–5 (β = 0.14). As expected, the relative strength of the relationship from PBS to dietary quality was significantly stronger than the reverse, from dietary quality to PBS.
Conclusions
Positive behavior management and proactive parenting practices are an important foundation for establishing a healthy nutritional environment for young children. These findings suggest that family-centered prevention interventions for pediatric obesity may benefit from targeting PBS in service of promoting better dietary quality.
Keywords: dietary quality, early childhood, eating behavior, positive parenting
Introduction
Pediatric obesity is a significant public health concern because of its high prevalence and serious long-term physical and psychological consequences (National Center for Health Statistics, 2012). It is well established that dietary practices and physical activity significantly influence the risk of obesity across the lifespan (Spruijt-Metz, 2011). Pediatric obesity and eating behaviors can best be understood within an ecological framework in which child characteristics interact with the environment and affect health outcomes (Davison & Birch, 2001). The family, particularly the parents or other primary caregivers, may influence diet and food preference by modeling and controlling the portion sizes and dietary quality of the food they make available to their children (Davison & Birch, 2001; Fisher, 2007). Further, children become more familiar with and more likely to consume the food items to which they are exposed (Hill, 2002; Ventura & Birch, 2008). Other parenting practices that influence children’s diets and weight status include prompting children to eat, restricting access to food, and using dessert as reward for eating more healthy foods, such as fruits, vegetables, and dairy (Rhee, 2008; US Department of Health and Human Services, 2000). Perhaps a less evident way that parents influence their child’s diet is through fundamental parenting practices not specific to diet and eating behaviors (Kitzmann & Beech, 2011; Rhee, 2008). To identify ways to help parents provide their children with more healthy dietary options, and thus aid in obesity prevention efforts, it would therefore be logical to examine parenting factors that contribute to parents’ efforts to present healthy and nutritious food options to their children.
Empirical studies have linked parenting styles and parenting skills to children’s diet and exercise and thus on children’s weight status (Rhee, 2008). Rhee (2008) provided a conceptual model that highlights the role of positive parenting behaviors on children’s healthy diets through the establishment of a healthy home environment (i.e., making healthy food available, modeling healthy dietary habits). In Rhee’s model, family interactions and parenting behaviors are postulated to affect children’s eating behaviors, diet, and physical activity, which in turn are hypothesized to influence the child’s weight status. Planning family meals, making healthy food options available, and encouraging the family to eat healthy and stay active (e.g., watch less television) requires organization and planning, appropriate monitoring from parents, and effective management of the family’s daily routines and child behavior; thus, children from families with less than optimal parenting behaviors may be at higher risk for obesity. Further, parents in such families may find it especially challenging to manage children’s preferences for food of low nutritional quality. Therefore, interventions that target only nutrition and diet in early childhood may be less effective than those that also target specific parenting skills.
The key to successful family-centered interventions is the identification of specific parenting practices that are modifiable (Dishion & Patterson, 1999). Unfortunately, the majority of studies have examined the diets of families with young children with measures that tap only the global parenting styles (e.g., authoritative, authoritarian, permissive) rather than specific parenting behaviors. Findings that have related parenting styles to dietary practices are inconsistent. Although some studies have found that authoritative parenting, characterized by high levels of warmth and behavioral control and by open communication (Baumrind, 1971), is associated with availability and higher consumption of fruits and vegetables by children (Blissett, 2011; Kremers, Brug, de Vries, & Engels, 2003), other studies have found nonsignificant relations (Vereecken, Rovner, & Maes, 2010). No longitudinal studies have linked parenting behaviors to dietary practices, and no intervention studies have shown that changes in discrete parenting strategies are related to changes in dietary practices (Ventura & Birch, 2008).
To this end, we examined the reciprocal relation between positive behavior support (PBS) and dietary quality of the meals served to children. PBS is a key and observable parenting behavior found to be significantly prognostic of early conduct problems (Dishion et al., 2008) and self-regulation skills (Lunkenheimer et al., 2008). There is a growing consensus in education, counseling and psychology that PBS is an effective and easily disseminated set of behavior management practices for schools and families (Carr et al., 1999; Dishion et al., 2008; Sugai & Horner, 2006). PBS emphasizes the use of nonaversive, reinforcing caregiver–child interactions and involves the caregiver being proactive and structuring children’s activities in ways that reduce opportunities for problem behavior, as well as promote children’s motivation for self-regulation (Lunkenheimer et al., 2008). One of the key principles of PBS is prompting and reinforcing children’s positive behavior, and therefore, it is optimally measured using direct observations of caregivers’ use of positive reinforcement strategies, stating clear expectations for positive behaviors, positively engaging with the child, and structuring the child’s environment to provide a context for healthy development. Previous research with the study sample has indicated that participating in the Family Check-Up (FCU; Dishion & Stormshak, 2007) an evidence-based parenting intervention, leads to improvements in parents’ use of PBS in toddlerhood, which in turn is related to reduced problem behavior 2 to 5 years later (Dishion et al., 2008; Lunkenheimer et al., 2008).
Recently we found positive intervention effects of the FCU on dietary quality of meals and reduced growth in body mass index (BMI) from age 5 to 9 (Smith et al., 2014). This finding is consistent with other early prevention work focusing on parenting practices to have collateral benefits on growth in childhood obesity (Brotman et al., 2012). Although promising, this research would benefit from studies examining how parenting practices such as PBS and dietary quality are linked over time and the extent to which PBS is a skill set that is also relevant to parents’ practice of offering healthy meals and ability to manage children’s preferences for healthy foods. A developmental process model of the links between parents’ preparation of healthy meals and PBS provides an empirical basis for the design and refinement of intervention programs for the prevention of pediatric obesity
In this study we used a cross-lag panel model to evaluate the longitudinal relationship between PBS and dietary quality of meals served to children from ages 2 to 5. It was hypothesized that higher levels of PBS would be prospectively related to better dietary quality of meals served to children. In the case that better dietary quality was prospectively related to higher levels of PBS, we hypothesized that the relative strength from PBS to dietary quality would be stronger than the opposite direction. Because children from families of lower socioeconomic status are at higher risk for obesity (Ogden, Carroll, Kit, & Flegal, 2014), we tested intervention condition, child gender, and family poverty status, assessed at age 2, as moderators of the relation between PBS and dietary quality over time to ensure generalizability. We did not hypothesize that the model would differ for any of the tested moderating variables.
Materials and Methods
This study included 731 families (49% female children) in a randomized, controlled trial who were recruited from Women, Infants, and Children Nutrition Program (WIC) sites in three geographically and culturally diverse U.S. regions near Charlottesville, Virginia; Eugene, Oregon; and Pittsburgh, Pennsylvania. Families with children between ages 2 years 0 months and 2 years 11 months who indicated risk on 2 out of 3 screening measures for socioeconomic, family, and child factors were invited to participate in the study. The most predominantly represented caregiver participants were biological mothers (> 90% at each age), and each caregiver–child dyad engaged in a yearly assessment. The sample is culturally diverse and includes European American (50.1%), African American (27.9%), Latino/Hispanic (13.4%), and American Indian, Asian American, Native Hawaiian, and multiple ethnicities (8.6%). The institutional review boards of the Universities of Oregon, Pittsburgh, and Virginia approved this research. Germane to the current study, the weight status of the children in the sample at age 5, based on the World Health Organization growth reference data for children ages 5 to 19 years (Onis et al., 2007), had the following distribution: underweight (2.7%), normal weight (62.0%), at risk for overweight (9.4%), at greater risk for overweight (8.9%), overweight (16.9%). In 2011–2012, 8.4% of children ages 2–5 and 17.7% of children ages 6–11 in the United States were obese (Ogden et al., 2014).
Following the first assessment at age 2, 367 families were randomly assigned to the intervention condition (FCU) and 364 were assigned to a WIC services as usual condition. The FCU consists of three sessions that are individually tailored to the needs of each family: (1) an initial interview, (2) a home-based assessment, and (3) a feedback session. First, caregivers and children who agreed to participate in the study had an initial contact session and then were scheduled for a 2.5-hour home visit each year from ages 2 to 5. Ninety percent of the families participated in the assessment at age 3 and 85% of the families participated at ages 4 and 5. The visit consisted of a series of age-appropriate interaction tasks and the completion of questionnaires by the caregiver(s). The tasks included a free play task followed by a clean-up task. Beginning at age 3 these tasks were followed by a delay of gratification task, teaching task, and age-appropriate inhibition task. Lastly, parent-child dyads participated in a 10-minute meal preparation and lunchtime task. During the meal preparation task families were instructed to prepare a meal for their child in their normal way and were told that the child could not be playing with toys or with others while the parent prepared the meal. The parents were to feed their children at the end of the 10-minute preparation time. The purpose of the meal task was the assessment of parenting behaviors, but not those specific to mealtime or feeding. Parents were informed in advance of this task and the meeting time was normally scheduled for lunchtime, albeit some visits occurred closer to dinnertime.
Only families in the intervention condition were eligible to participate in a feedback session each year. During the feedback session the therapists discussed parenting and family strengths and possible areas for improvement as gathered from the assessment. Engagement in the feedback session was entirely voluntary in each year of the study for families assigned to the intervention condition; thus, participation rates were variable across years and within families. More detailed information concerning the recruitment, intervention procedures, and engagement rates can be found in Dishion, Shaw, et al.(2008) and Dishion, Brennan, et al.(2014).
Measures
Positive behavior support
The PBS construct is a latent variable comprised of three behavioral observation scales assessed across all interaction tasks: First is a composite (mean) score of five scores assessed using the Coder Impressions Inventory (COIMP; Dishion, Hogansen, Winter, & Jabson, 2004). While viewing the home-based interaction tasks, coders used a 9-point Likert scale ranging from 1 (not at all) to 9 (very much) to rate each measure across all tasks. The five behaviors observed are: “Does the parent encourage positive child behavior with praise and/or incentives?”; “Does the parent prompt the child to transitions and/ or future requests for behavior change?”; “Is the parent appropriately contingent in responding to positive or compliant child behavior?”; “Does the parent give the child choices for behavior change whenever possible?”; “Does the parent use verbal structuring to make the task manageable?” Average interrater agreement was high at each age, ranging from 87% to 88% agreement. Second is dyadic positive engagement (DE), which was assessed using a dynamic systems approach with a moment by moment direct observation coding system: Relationship Affect Coding System (Peterson, Winter, Jabson, & Dishion, 2008). Using a 6 by 6 grid, we defined dyadic positive engagement as the region where either the caregiver or child was coded to be positively or neutrally engaged and the other member of the dyad was coded to be behaving likewise (4 total cells), following the approach used with families of adolescents (Dishion, Forgatch, Van Ryzin, & Winter, 2012). Reliability coefficients were in “excellent” range, with overall kappa scores of .93 at each age and percent agreement of .93, .94, .93, and .94 at ages 2, 3, 4, and 5, respectively. Kappa coefficients were obtained from Noldus Observer (Noldus Information Technology, 2012). The kappa coefficients are computed based on the duration and sequencing of coded behavior. Only interaction tasks administered across all four ages (the teaching, inhibition, and meal tasks) were included in the analysis. Third is based on the home visitor’s (a research assistant) observation score of positive behavior support. Home visitors indicated whether certain behaviors were present during the home visit, which included “Parent caresses or kisses child at least once”; “Parent keeps child in visual range and looks often”; “Parent seemed in good control of child.” Note that although the PBS construct used in this study reflects the same underlying parenting behaviors as previous versions of PBS published from this dataset, different indicators were used to allow for longitudinal evaluation. The previous version of PBS (Dishion et al., 2008; Lunkenheimer et al., 2008; Smith et al., 2014) included a measure only available at the age 2 and 3 assessments.
Dietary quality
A new coding team observed only the 10 minute videotaped meal preparation task at ages 2 through 5 years. Coders rated the nutritional quality of the food items served to the child during the meal preparation and lunchtime task on a 9-point Likert scale ranging from 1 (not at all nutritious) to 9 (very nutritious). A score ranging from 1 to 3 indicated a meal high in carbohydrates and fats, with very few fruits and vegetables. A meal with a score of 4–6 consisted of multiple food groups but had higher caloric density and fat content than a meal with a score of 7–9. Scores of 7–9 were given for meals with a variety of food groups represented, including fresh fruits and vegetables, and with lower caloric and fat content. Interrater agreement was high (83%).
Poverty
Poverty status was calculated by adjusting families’ gross household income reported at age 2 for inflation using the U.S. Department of Labor Bureau of Labor Statistics Consumer Price Index to reflect 2010 levels. Using this index, 76% were below the poverty line.
Statistical Analyses
Data analyses were conducted in Mplus 7.1 (Muthén & Muthén, 2012) using maximum likelihood estimation for the confirmatory factor analysis (CFA) and maximum likelihood estimation with robust standard errors for the cross-lagged panel model, which provides more valid estimates of standard errors when dependent variables are not normally distributed. Determination of model fit included the comparative fit index (CFI; Bentler, 1990), the root mean square error of approximation (RMSEA; Steiger, 1990), and the standardized root mean residual (SRMR; Bentler, 1995). CFI values greater than 0.93 indicate good fit to the data (Byrne, 1994). RMSEA values less than 0.06 indicate good model fit (Hu & Bentler, 1999). SRMR values less than .08 are considered good fit (Hu & Bentler, 1999).
CFA was used to assess the measurement of the PBS latent variable with the specified indicators. With acceptable fit for the PBS construct, a cross-lagged panel model was then constructed to evaluate the relation between PBS and nutritional quality across ages 2, 3, 4, and 5. Variables assessed concurrently were allowed to correlate. With cross-lagged models, it is possible to determine the direction of causality between variables measured across time and the strength of this relation (Finkel, 2004). We tested for significant differences between the relative strengths of the two directions of the cross-lags (i.e., PBS to dietary quality, dietary quality to PBS). First, we compared a model in which the paths were constrained to be equal within their respective directions with one in which all the cross-lagged paths were constrained to be equal to each other. A significant decrement in model fit after imposing the second constraint indicates that there are significant differences in the relative strength of the associations by direction. We then tested for moderation of the model by intervention condition, child gender, and the geographical region of data collection.
Results
Table 1 contains the intercorrelations and descriptive statistics of the age 2 variables in this study. Of note, nutritional quality was positively and significantly (p < .001) correlated to PBS (r = .24); correlations between intervention condition and study variables were small and generally nonsignificant. Omnibus tests of group differences were run to compare the means of study variables for the treatment and control groups. There were no significant differences between treatment and control groups and the relation between PBS and dietary quality was not expected to be attenuated by the intervention, lending support for the use of the whole sample in subsequent analyses.
Table 1.
Intercorrelations Between Study Variables at Age 2
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Child gender | – | -.049 | -.007 | .019 | -.047 | -.036 |
| 2. Child race/ethnicity | – | -.020 | .047 | -.019 | -.044 | |
| 3. Intervention condition | – | .011 | -.005 | -.001 | ||
| 4. Poverty | – | -.001 | -.073 | |||
| 5. Dietary quality of meals | – | .258*** | ||||
| 6. PBSa | – | |||||
| Mean | 4.33 | |||||
| Standard deviation | 2.10 | |||||
| N | 725 | 731 | 731 | 720 | 594 | 722 |
Note. Intercorrelations for variables at ages 3, 4, and 5 are available upon request from the corresponding author.
p < .05,
p < .01,
p < .001;
Regression factor scores
CFA of the PBS Construct
PBS was estimated as a latent variable with three indicators. The CFA model provided good fit to the data, χ2(30) = 50.110, CFI = .989, RMSEA = .030, SRMR = 0.023. Standardized factor loadings for all the indicators of PBS were statistically significant (p < .01) and greater than .40 at each age with the following ranges: COIMP, .596– .686; DE, .490– .572; Home visitor’s observation score, .512– .615; indicating that all factors contributed to the latent construct.
Cross-Lagged Panel Model
The cross-lagged panel model (Figure 1) provided good fit to the data, χ2(74) = 151.605, CFI = .963, RMSEA = .038, SRMR = 0.035. PBS significantly (p < .01) predicted dietary quality at each subsequent age: age 2–3 (β = .30), age 3–4 (β = 0.14), and age 4–5 (β = 0.37). Dietary quality at age 3 significantly predicted PBS at age 4 (β = .16), and age 4 significantly predicted PBS at age 5 (β = 0.14). Dietary quality at age 2 did not significantly predict PBS at age 3.
Figure 1.
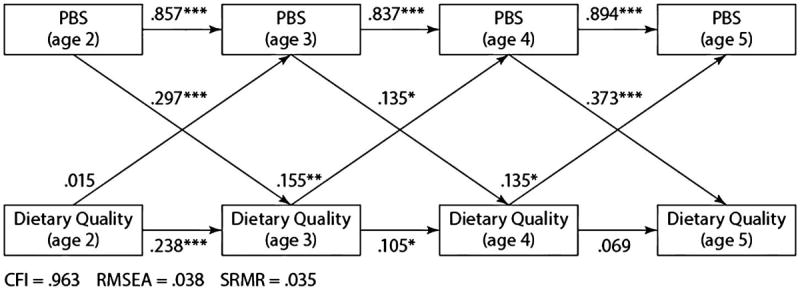
Cross-lagged panel model.
Results of nested model deviance tests indicated that the cross-lagged paths from PBS to dietary quality were significantly stronger relative to those in the opposing direction. Moderation analyses revealed no significant invariance by intervention group assignment, child gender, or family poverty status.
Discussion
There are noteworthy findings of this study. The first is that a relatively reliable measure of the caregiver’s ability to prepare healthy meals can be assessed with a 10 minute videotaped task. The reliability and stability coefficients suggest that dietary practices are relatively stable and directly observable. Our research suggests that the food prepared during this task uniquely predicts future growth in body weight, and is related to parents’ behavior management skills as captured in the PBS construct. This finding alone suggests that caregiver’s skill and attention to meal preparation is clearly an important facet of programs designed to promote healthy eating or that target nutrition as part of the overall program. Of interest is the potential exploration of the differential validity of this observational meal preparation measure and caregiver reports of the nutritional quality with respect to growth in children’s healthy eating habits and body weight.
The second important finding is that caregiver’s use of PBS is helpful for their ability to maintain and manage high quality nutritional meals over the course of early childhood. Our findings are consistent with those from previous research in that a link was identified between fundamental parenting behaviors and dietary practices (Kremers et al., 2003; Schmitz et al., 2002; Smith et al., 2014). However, our study extended previous findings within a longitudinal design and revealed that higher ratings of parents’ PBS strategies from ages 2 to 5 are associated with serving meals with higher dietary quality in subsequent years. Conversely, dietary quality at ages 3 and 4 predicted PBS at subsequent years. As hypothesized, the relative strength of the link from PBS to dietary quality was greater than that for dietary quality to PBS.
Our results also support the existing research finding that parents who show high levels of warmth and sensitivity are more likely to serve more nutritious meals to their children and a greater number of fruits and vegetables (Rhee, 2008; Schmitz et al., 2002). Although the provision of more nutritional meals does not necessarily relate to consumption of those food items, the relationship between nutritional quality in early childhood and trajectories of BMI from ages 5 to 9.5 found in this sample (Smith et al., 2014) indicates a salient connection between dietary quality and later BMI. Further, Smith and colleagues found that intervention effects on PBS were related to serving more nutritious meals, which predicted healthier weight trajectories. Despite finding intervention effects on PBS in this sample by using an intention-to-treat analytic approach (Smith et al., 2014), we did not find that intervention group assignment moderated the relationship between PBS and dietary quality in our model. This suggests that even though there is malleability in positive parenting behaviors, the processes in our model represent a naturally occurring relationship between PBS and dietary quality that was not changed by the intervention. Similarly, the model was found to be equivalent across genders and levels of poverty.
Our findings are relevant to early interventions for the complications of obesity and maladaptive eating practices, which would include conditions such as Type 2 diabetes mellitus and other diet-controlled metabolic syndromes that commonly prescribe dietary modification as part of the treatment plan. Given that PBS was related to better dietary quality, even though diet was not specifically targeted, family-based interventions for these conditions may benefit from targeting PBS as an effective means of improving specific health behaviors, such as providing more nutritious meals,
Limitations and Future Directions
Although this study has a number of strengths, including a large geographically and culturally diverse randomized sample, inclusion of pertinent covariates, a longitudinal design, and observational assessment of parenting, child behaviors, and dietary quality of meals served, it has some limitations. First, ratings of dietary quality were based on one meal each year. Although these ratings appear to be stable across the 4 years, future studies could use a larger sampling of meals and more objective indices to assess diet. Second, the semi-structured meal task limited parents to 10 minutes for meal preparation, which could have constrained the types of meals they were able to prepare. Further, the presence of research staff and constraints of the tasks (i.e., time limit, the child not being allowed to play with toys) could also have influenced the types of meals prepared. Third, our model did not address a prominent shortcoming in the literature: examination of the relationship between parenting skills, physical activity, and provision of healthy meals in the same model (Rhee, 2008; Schmitz et al., 2002). Last, recruitment of families who were using WIC services limited the generalizability of our findings to families with less socioeconomic risk and families of similar high risk who are not engaged in WIC services, which likely would affect the dietary quality of food available to the child.
Conclusions
Our findings provide initial strong evidence of the temporal link between observable parenting behaviors and dietary practices from ages 2 to 5. Although dietary quality and parenting practices are highly interrelated, our study revealed a stronger relation between parenting and later dietary quality than vice versa. These findings lend additional support to the inclusion of parenting behaviors in models of eating and feeding behaviors in early childhood. Further, these findings suggest that interventions that effectively increase PBS during early childhood have the potential to reduce rates of overweight and obesity in later developmental periods and decrease the prevalence of weight-related mental and physical health conditions.
highlights.
We examine the reciprocal relation between parenting and dietary quality of meals
We use observational measures of parenting and of dietary quality of meals
Positive behavior support positively predicts dietary quality of meals over time
Acknowledgments
This research was supported by National Institute on Drug Abuse grant DA016110 to Drs. Dishion, Shaw, and Wilson. Zorash Montaño was supported by minority fellowship SM60563-40 from the Department of Health and Human Services. Seed funding from the College of Liberal Arts and Sciences at Arizona State University awarded to Thomas Dishion supported Dr. Smith’s and Zorash Montano’s research. The authors also gratefully thank Cheryl Mikkola for editorial support, the observational coding team at the Child and Family Center, the rest of the Early Steps team in Eugene, Pittsburgh, and Charlottesville, and the families who have participated in the study.
Abbreviations
- COIMP
Coder Impressions Inventory
- FCU
Family Check-Up
- PBS
positive behavior support
- RPC
Relationship Process Code
- WIC
Women, Infants, and Children Nutrition Program
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Baumrind D. Current patterns of parental authority. Developmental Psychology Monograph. 1971;4:101–103. [Google Scholar]
- Bentler PM. Comparative fit indexes in structural models. Psychological bulletin. 1990;107(2):238. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bentler PM. EQS structural equations program manual. Encino, CA: Multivariate Software; 1995. [Google Scholar]
- Blissett J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite. 2011;57(3):826–831. doi: 10.1016/j.appet.2011.05.318. [DOI] [PubMed] [Google Scholar]
- Brotman LM, Dawson-McClure S, Huang K-Y, Theise R, Kamboukos D, Wang J, Ogedegbe G, et al. Early childhood family intervention and long-term obesity prevention among high-risk minority youth. Pediatrics. 2012;129(3):e621–e628. doi: 10.1542/peds.2011-1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byrne BM. Structural equation modeling with EQS and EQS/Windows: Basic concepts, applications, and programming. Sage; 1994. [Google Scholar]
- Carr EG, Horner RH, Turnbull AP, Marquis JG, Magito McLaughlin D, McAtee ML, Doolabh A, et al. Positive behavior support for people with developmental disabilities: A research synthesis. Washington, DC: American Association on Mental Retardation; 1999. [Google Scholar]
- Davison KK, Birch LL. Childhood overweight: A contextual model and recommendations for future research. Obesity Reviews. 2001;2(3):159–171. doi: 10.1046/j.1467-789x.2001.00036.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Brennan LM, Shaw DS, McEachern AD, Wilson MN, Jo B. Prevention of problem behavior through annual Family Check-Ups in early childhood: Intervention effects from home to early elementary school. Journal of Abnormal Child Psychology. 2014;42(3):343–354. doi: 10.1007/s10802-013-9768-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Forgatch MS, Van Ryzin MJ, Winter C. The nonlinear dynamics of family problem solving in adolescence: The predictive validity of a peaceful resolution attractor. Nonlinear dynamics, psychology, and life sciences. 2012;16(3):331. [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Patterson GR. Model-building in development psychopathology: A pragmatic approach to understanding and intervention. Journal of Clinical Child Psychology. 1999;28(4):502–512. doi: 10.1207/S15374424JCCP2804_10. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Shaw D, Connell AM, Gardner F, Weaver C, Wilson MN. The Family Check-Up With High-Risk Indigent Families: Preventing Problem Behavior by Increasing Parents’ Positive Behavior Support in Early Childhood. Child development. 2008;79(5):1395–1414. doi: 10.1111/j.1467-8624.2008.01195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Stormshak EA. Intervening in children’s lives: An ecological, family-centered approach to mental health care. American Psychological Association; 2007. [Google Scholar]
- Finkel SE. Cross-lagged. In: Lewis-Beck M, Bryman AE, Liao TF, editors. The Sage encyclopedia of social science research methods. Vol. 1. Sage; 2004. [Google Scholar]
- Fisher JO. Effects of Age on Children’s Intake of Large and Self-selected Food Portions. Obesity. 2007;15(2):403–412. doi: 10.1038/oby.2007.549. [DOI] [PubMed] [Google Scholar]
- Hill AJ. Developmental issues in attitudes to food and diet. Proceedings of the Nutrition Society. 2002;61(02):259–266. doi: 10.1079/PNS2002152. [DOI] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6(1):1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Kitzmann KM, Beech BM. Family-based interventions for pediatric obesity: Methodological and conceptual challenges from family psychology. Couple and Family Psychology: Research and Practice. 2011;1(S):45–62. doi: 10.1037/2160-4096.1.S.45. [DOI] [PubMed] [Google Scholar]
- Kremers SPJ, Brug J, de Vries H, Engels RCME. Parenting style and adolescent fruit consumption. Appetite. 2003;41(1):43–50. doi: 10.1016/S0195-6663(03)00038-2. [DOI] [PubMed] [Google Scholar]
- Lunkenheimer ES, Dishion TJ, Shaw DS, Connell AM, Gardner FEM, Wilson MN, Skuban EM. Collateral benefits of the Family Check-Up on early childhood school readiness: Indirect effects of parents’ positive behavior support. Developmental Psychology. 2008;44(6):1737–1752. doi: 10.1037/a0013858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén BO, Muthén LK. Mplus, Version 7.1. Los Angeles, CA: Muthén & Muthén; 2012. [Google Scholar]
- Nader PR, O’Brien M, Houts R, Bradley R, Belsky J, Crosnoe R, Susman EJ, et al. Identifying risk for obesity in early childhood. Pediatrics. 2006;118(3):e594–e601. doi: 10.1542/peds.2005-2801. [DOI] [PubMed] [Google Scholar]
- National Center for Health Statistics. Health, United States, 2011: With Special Feature on Socioeconomic Status and Health. Hyattsville MD: 2012. [PubMed] [Google Scholar]
- Noldus Information Technology. The Observer XT reference manual 11.0. Wageningen, the Netherlands: Author; 2012. [Google Scholar]
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onis Md, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization. 2007;85:660–667. doi: 10.1590/S0042-96862007000900010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson J, Winter C, Jabson J, Dishion TJ. The Relationship Affect Coding System coding manua. University of Oregon; Eugene, OR 97403 Eugene, OR: 2008. Available from the Child and Family Center, 6217. [Google Scholar]
- Rhee KE. Childhood overweight and the relationship between parent behaviors, parenting style, and family functioning. The ANNALS of the American Academy of Political and Social Science. 2008;615(1):11–37. doi: 10.1177/0002716207308400. [DOI] [Google Scholar]
- Schmitz KH, Lytle LA, Phillips GA, Murray DM, Birnbaum AS, Kubik MY. Psychosocial correlates of physical activity and sedentary leisure habits in young adolescents: The teens eating for energy and nutrition at school study. Preventive Medicine. 2002;34(2):266–278. doi: 10.1006/pmed.2001.0982. [DOI] [PubMed] [Google Scholar]
- Smith JD, Montaño Z, Dishion TJ, Shaw DS, Wilson MN. Preventing weight gain and obesity: Indirect effects of a family-based intervention in early childhood. Prevention Science. 2014 doi: 10.1007/s11121-014-0505-z. Available ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spruijt-Metz D. Etiology, treatment, and prevention of obesity in childhood and adolescence: A decade in review. Journal of Research on Adolescence. 2011;21(1):129–152. doi: 10.1111/j.1532-7795.2010.00719.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steiger JH. Structural model evaluation and modification: An interval estimation approach. Multivariate behavioral research. 1990;25(2):173–180. doi: 10.1207/s15327906mbr2502_4. [DOI] [PubMed] [Google Scholar]
- Sugai G, Horner RH. A promising approach for expanding and sustaining school-wide positive behavior support. School Psychology Review. 2006;35(2):245. [Google Scholar]
- US Department of Health and Human Services. Report of the Surgeon General’s conference on children’s mental health: A national action agenda. 2000 [PubMed] [Google Scholar]
- Ventura A, Birch L. Does parenting affect children’s eating and weight status? International Journal of Behavioral Nutrition and Physical Activity. 2008;5(1):15. doi: 10.1186/1479-5868-5-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vereecken C, Rovner A, Maes L. Associations of parenting styles, parental feeding practices and child characteristics with young children’s fruit and vegetable consumption. Appetite. 2010;55(3):589–596. doi: 10.1016/j.appet.2010.09.009. [DOI] [PubMed] [Google Scholar]