

Highlights
-
•
Serious complications during routinely performed procedures due to improper use of V-Loc™ barbed wire can occur.
-
•
When used intraabdominally the V-Loc™ barbed absorbable wire needs to be shortened and the suture stump to be extraperitonealized.
-
•
Surgeons need to be aware of relevant “tricks and traps” of routinely performed procedures.
Keywords: Transabdominal perperitoneal hernia repair, TAPP, V-Loc™ wire, Small bowel volvulus
Abstract
Introduction
Transabdominal preperitoneal endoscopic hernia repair (TAPP) is part of primary surgical health care. While both, the reported recurrence rate and procedure specific morbidity are consistently low, rare serious complications occur.
Presentiation of case
A 36-year-old male patient developed bowel obstruction three days after both-sided TAPP for inguinal hernia repair. A computer tomography scan of the abdomen revealed a small bowel volvulus in the right lower quadrant of the abdomen requiring urgent revisional surgery. Intraoperatively, the small bowel and its mesenterial vessels were found to be twisted around a 5 cm long V-Loc™ barbed absorbable suturing wire. After successful laparoscopic adhesiolysis, removal of the wire and detorquing of the bowel conglomerate, resection of small intestine was not necessary. The patient's further postoperative recovery was uneventful.
Discussion
Due to the barbed configuration of the V-Loc™ wire, a gapless continuous suturing of the peritoneum without laparoscopic knotting is easily and fast to accomplish. In this case the recommendation of the manufacturer to shorten the wire was not strictly followed and neither had the suture stump been extraperitonealized in order to avoid such rare complications.
Conclusion
Surgeons need to be aware of relevant “tricks and traps” of routinely performed procedures and have to know all tools and material they use very well. This case may therefore increase our attention when it comes to little things which actually do matter.
1. Introduction
During the last decade endoscopic surgery has emerged as one of the ‘gold standard’ for inguinal hernia repair with the transabdominal preperitoneal hernia repair (TAPP) being the preferred choice in female patients [1]. This procedure is commonly performed and part of primary surgical health care worldwide. While both the reported recurrence rate and procedure specific morbidity are consistently low, rare serious complications can occur [2].
2. Case report
Herein, we describe the case of a 36 years old male patient who was referred to our tertiary care hospital three days after external both-sided TAPP for inguinal hernia repair. After a good initial recovery the patient developed abdominal pain and bowel obstruction. Further investigations showed increased blood inflammatory markers and absent peristalsis in the ultrasound. A computer tomography (CT) scan of the abdomen revealed a small bowel volvulus in the right lower quadrant of the abdomen (Fig. 1) requiring urgent revisional surgery.
Fig. 1.

Computer tomography (CT) scans in 36 years old man with small bowel volvulus (‘whirlpool-sign’, white asterix) in the lower right quadrant of the abdomen.
Intraoperative, the CT finding was verified, with the small bowel and its mesenterial vessels being twisted around a 5 cm long V-Loc™ barbed absorbable suturing wire. After successful laparoscopic andhesiolysis, removal of the wire and detorquing of the bowel conglomerate, resection of small intestine was not necessary (Fig. 2A–D). The patient’s postoperative recovery was uneventful and the patient was discharged four days after surgery.
Fig. 2.
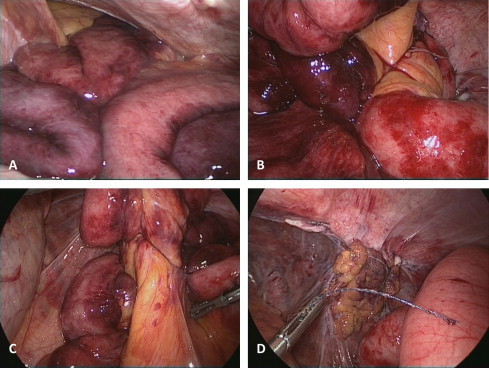
Small bowel and its mesenterial vessels are twisted around a 5 cm long V-Loc™ barbed absorbable suturing wire (A–D).
3. Discussion
The V-Loc™ wire can be used for closure of the peritoneum during the TAPP procedure. Due to its barbed configuration, a gapless continuous suturing of the peritoneum without laparoscopic knotting is easily and fast to accomplish [3].
A similar complication following V-Loc™ suture induced has not been reported in the context of endoscopic hernia repair yet. However, a review of the English language literature revealed few similar reports after intraperitoneal usage of this wire in the context of gynecological and colorectal surgery [4,5].
The common feature of all reported cases was that the recommendation of the manufacturer to shorten the wire (to the length of not more than 2 cm) was not strictly followed and neither had the suture stump been extraperitonealized in order to avoid such rare complications.
4. Conclusion
The key message of this case is as simple as crucial. Surgeons need to be aware of relevant “tricks and traps” of routinely performed procedures and have to know all tools and material they use very well. This case may therefore increase our attention when it comes to little things which actually do matter.
Conflicts of interest
J. Filser, F. Seyfried J. Reibetanz and C-T Germer declare no conflict of interest and no financial support.
K. Kraijnovic makes known, that she is a consultant for KARL STORZ GmbH (Tuttlingen, Germany).
U.A.Dietz makes known that he has or has had business relationships with the following companies: B.Braun-Aesculap, Covidien and Ethicon. Activities in connection with these companies include consulting, speaking, advising and research; U.A. Dietz declares no conflict of interest that directly relates to this study.
Sources of funding
This study was not funded.
Ethical approval
Not applicable.
Consent
Written consent has been obtained from the patient and will be provided if the Editor should ask to see it.
Author contribution
J.F. and F.S. collected data and wrote the manuscript. K.K., C.T.G., J.R. and U.A.D. reviewed/edited the manuscript and contributed to the discussion.
Guarantor
J.F. and F.S. accept full responsibility for the work.
Key learning points
-
•
Serious complications due to improper use of V-Loc™ barbed wire can occur.
-
•
When used intraabdominally the V-Loc™ barbed absorbable wire needs to be shortened and the suture stump to be extraperitonealized.
-
•
Surgeons need to be aware of relevant “tricks and traps” of routinely performed procedures.
Reference
- 1.Bracale U., Melillo P., Pignata G., Di Salvo E., Rovani M., Merola G. Which is the best laparoscopic approach for inguinal hernia repair: TEP or TAPP? A systematic review of the literature with a network meta-analysis. Surg. Endosc. 2012;26:3355–3366. doi: 10.1007/s00464-012-2382-5. [DOI] [PubMed] [Google Scholar]
- 2.Lovisetto F., Zonta S., Rota E., Bottero L., Faillace G., Turra G. Laparoscopic transabdominal preperitoneal (TAPP) hernia repair: surgical phases and complications. Surg. Endosc. 2007;21:646–652. doi: 10.1007/s00464-006-9031-9. [DOI] [PubMed] [Google Scholar]
- 3.Ruff G.L. The history of barbed sutures. Aesthet. Surg. J. – Am. Soc. Aesthet. Plast. Surg. 2013;33:6S–12S. doi: 10.1177/1090820X13498505. [DOI] [PubMed] [Google Scholar]
- 4.Burchett M.A., Mattar S.G., McKenna D.T. Iatrogenic intestinal and mesenteric injuries with small bowel volvulus following use of barbed suture during laparoscopic myomectomy. J. Laparoendosc. Adv. Surg. Tech. A. 2013;23:624–632. doi: 10.1089/lap.2013.0065. [DOI] [PubMed] [Google Scholar]
- 5.Salminen H.J., Tan W.S., Jayne D.G. Three cases of small bowel obstruction after laparoscopic ventral rectopexy using the V-Loc((R)) suture. Tech. Coloproctol. 2014;18:601–612. doi: 10.1007/s10151-013-1074-z. [DOI] [PubMed] [Google Scholar]