

Abstract
Background
The prevalence, degree, and patterns of hearing loss associated with chronic kidney disease (CKD) reported by various studies differ significantly. The effects of haemodialysis and duration of disease on hearing loss remain unclear.
Aims
The aim of this study was to determine the prevalence and degree of hearing loss in CKD patients on haemodialysis.
Methods
This study included 120 CKD patients on haemodialysis. Information regarding age, gender, duration of disease, subjective hearing loss, exposure to ototoxic drugs, comorbidities like diabetes, hypertension, and hypothyroidism, renal functions, electrolytes and number of haemodialysis sessions received were obtained. An equal number of age and sex matched controls were used to determine prevalence of hearing loss in CKD patients after subjecting both groups to pure tone audiometry. We compared CKD patients with and without hearing loss for association of hearing loss with disease duration, number of haemodialysis, and blood parameters.
Results
Hearing loss was present in 41.7 per cent of CKD patients, significantly higher than controls (p=0.001), and was mild in the majority of patients. Impairment was noted across high and low frequencies of audiometric testing. Median duration of disease was the same (18 months) among CKD patients with and without hearing loss (p=0.62). CKD patients with hearing loss received 72 haemodialysis compared to 122 sessions by those without hearing loss (p=0.04).
Conclusion
Mild sensorineural hearing loss is common in CKD. Hearing loss has no specific pattern as it prevails at high and low frequencies. Hearing loss may be inversely associated with the number of haemodialysis sessions but not with duration of disease.
Keywords: CKD, hearing loss, haemodialysis, high frequency loss, low frequency loss
What this study adds:
-
What is known about this subject?
Chronic kidney disease (CKD) is known to be associated with sensorineural hearing loss.
-
What new information is offered in this study?
There is a high prevalence of sensorineural hearing loss in CKD patients. Hearing loss is more obvious in the elderly and in patients who have received fewer haemodialysis sessions. Chronicity of disease is not associated with CKDrelated hearing loss.
-
What are the implications for research, policy, or practice?
CKD patients on haemodialysis should be screened for early detection of hearing loss. Larger prospective studies are needed to establish whether instituting haemodialysis would slow down progression of hearing loss in such patients.
Background
The incidence of chronic kidney disease (CKD) has increased significantly in the past few years, thanks to the huge rise in the number of people suffering from diabetes mellitus and systemic hypertension, which are major risk factors for CKD. Association of CKD with sensorineural hearing loss has been described by several studies in the past, although the basis for this has not been clearly established.1,2 Antigenic similarity between basement membranes of glomeruli and stria vascularis of the inner ear may explain this association to some extent.3 Use of ototoxic drugs, electrolyte disturbances, and hypertension have been implicated in various studies.4-6
Haemodialysis has also been reported to contribute to hearing loss in CKD.7 Studies on the impact of haemodialysis have produced contradictory results, with a sizeable number reporting that haemodialysis plays no role in hearing loss associated with CKD. Although chronicity of disease was found to have no association with hearing loss in many studies,8 a recent study demonstrated that the greater the duration of disease, the greater the hearing loss.9 Thus, despite the multitude of studies regarding hearing loss in CKD, unanswered questions remain regarding the role of haemodialysis and duration of disease. We aimed to determine the prevalence and degree of hearing loss in CKD patients on haemodialysis, and to identify the association between hearing loss and factors like duration of CKD and number of haemodialysis sessions.
Method
This was a hospital-based case control study conducted in a tertiary care teaching hospital. The study comprised 120 adult patients with CKD, who have undergone at least one session of haemodialysis; 120 age and sex-matched controls were also enrolled. We excluded CKD patients with conductive hearing loss and syndromic etiologies of CKD in which hearing loss is a known component. All patients were interviewed using a uniform proforma containing information on age, gender, and risk factors, including diabetes, hypertension, and history of ototoxic drug use. Time since diagnosis of chronic kidney disease and number of haemodialysis sessions were documented. Blood parameters, including haemoglobin, blood urea, serum creatinine, sodium, potassium, chloride, and bicarbonate were also obtained.
All CKD patients and controls were subjected to hearing assessment using standard pure tone audiometry and impedance audiometry. Prevalence and degree of hearing loss was determined in CKD patients and controls. The patients with CKD on haemodialysis were further divided into two groups based on presence or absence of hearing loss. These two groups were compared for any differences with regard to exposure to ototoxic drugs, duration of CKD, number of haemodialysis sessions, and blood parameters. The hearing thresholds at low and high frequency ranges were compared between these groups to identify the pattern of hearing loss. Written informed consent was obtained from CKD patients and controls. Approval of the Institute Ethics and Research Committee was obtained prior to the study.
Statistical methods
In order to estimate a prevalence of 50 per cent with 9 per cent precision, a sample size of 119 was required, hence we included 120 subjects in each group. Prevalence and degree of sensorineural hearing loss was determined using descriptive statistics (mean, median, and standard deviation). CKD patients with and without hearing loss were compared using unpaired t-test for normally distributed variables and Mann Whitney test for non-normally distributed variables. Chi-square test was used to determine association between variables. Differences were considered significant if the p value was less than 0.05.
Results
The majority of patients in both CKD and control groups were male (75.8 per cent). Prevalence of diabetes and hypertension were higher in CKD patients, whereas there was no significant difference in the prevalence of hypothyroidism between CKD patients and controls (Table 1).
Table 1: Prevalence of major risk factors for hearing loss among CKD patients and controls (n=120 in each group).
| Parameter | CKD patients (%) | Controls (%) | p value |
|---|---|---|---|
| Noise exposure | 13 (10.8%) | 9 (7%) | 0.50 |
| Hypertension | 91 (75.8%) | 18 (15%) | 0.001 |
| Diabetes mellitus | 27 (22.5%) | 12 (10%) | 0.01 |
| Hypothyroidism | 10 (8.3%) | 4 (3.3%) | 0.17 |
A significantly higher number of CKD patients reported subjective hearing loss compared to controls (19.2 per cent vs. 5.8 per cent, p=0.003).
Overall, hearing loss as established by pure tone average was present in 50 out of 120 (41.7 per cent) CKD patients and 18 out of 120 (15 per cent) controls (p=0.001). Hearing thresholds were abnormal at low frequencies (250 Hz to 1 kHz) in 33 (27.5 per cent) patients and at high frequencies (2 kHz to 8 kHz) in 93 (77.5 per cent) CKD patients. Hearing thresholds were abnormal across all frequency ranges in 52 (43 per cent) CKD patients. Thus, high-frequency hearing loss was the most common hearing impairment among CKD patients, followed by hearing impairment across all frequencies and low-frequency hearing loss.
Sensorineural hearing loss was mild in the majority of CKD patients. There was significant difference between CKD patients and controls across all degrees of hearing loss (Table 2).
Table 2: Degree of hearing loss among CKD patients and controls (n=120 in each group).
| Degree of hearing loss | CKD patients (%) | Controls (%) | p value |
|---|---|---|---|
| Mild | 28 (23.3%) | 7 (5.8%) | 0.001 |
| Moderate | 10 (8.3%) | 6 (5.1%) | 0.001 |
| Moderately severe | 4 (3.3%) | 1 (0.8%) | 0.001 |
| Severe | 2 (1.7%) | 0 | 0.001 |
| Profound | 1 (0.8%) | 0 | 0.001 |
Of the 50 CKD patients with hearing loss, 38 had bilateral hearing loss, although this was not symmetric. In the control group, of the 18 subjects with hearing loss, 9 had bilateral impairment. The difference was not significant (p=0.07).
Comparison of CKD patients with and without hearing loss
The mean age of CKD patients with hearing loss was 52.7 years (SD=10.9) compared to 47 years (SD=12) among CKD patients without hearing loss (p=0.04). Thus CKD patients with hearing loss were a little older than those without hearing loss.
Twenty-five (50 per cent) of CKD patients with hearing loss had received ototoxic drugs compared to 21 out of 70 (30 per cent) of CKD patients without hearing loss (p=0.04). Frusemide was the most commonly implicated ototoxic drug. History of noise exposure, prevalence of diabetes, hypertension, and hypothyroidism, and mean values of blood parameters like haemoglobin, renal function, and electrolytes were comparable between the two groups (Table 3).
Table 3: Comparison of risk factors and blood parameters between CKD patients with and without hearing loss.
| Parameter/ risk factor | CKD patients with hearing loss (n=50) | CKD patients without hearing loss (n=70) | p value |
|---|---|---|---|
| Mean age (years) | 52.7 | 47 | 0.04 |
| Ototoxic drug exposure (%) | 50 | 30 | 0.04 |
| Noise exposure (%) | 16 | 7.1 | 0.15 |
| Hypertension (%) | 76 | 75.7 | 1.00 |
| Diabetes mellitus (%) | 22 | 22.8 | 1.00 |
| Hypothyroidism (%) | 10 | 7.14 | 0.74 |
| Mean haemoglobin (g/dl) | 9.5 | 9.3 | 0.42 |
| Mean blood urea (g/dl) | 95.3 | 96.06 | 0.91 |
| Serum creatinine (mg/dl) | 5.9 | 6.2 | 0.50 |
| Serum sodium (mEq/l) | 130.7 | 132.6 | 0.1 |
| Serum potassium (mEq/l) | 4.68 | 4.72 | 0.71 |
| Serum chloride (mEq/l) | 103 | 103.2 | 0.88 |
| Serum bicarbonate (mEq/l) | 19.2 | 19.8 | 0.34 |
| Median duration of CKD (months) | 18 | 18 | 0.62 |
| Median number of haemodialysis | 72 | 122 | 0.04 |
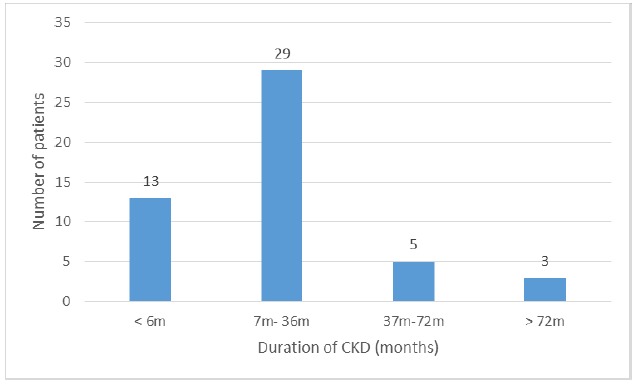
The majority of CKD patients with hearing loss had disease duration between seven months to three years (Figure 1). The median duration of disease in CKD patients with and without hearing loss was 18 months (p=0.62). Thus, duration of CKD had no association with hearing loss.
Figure 1: Duration of disease among CKD patients with hearing loss.
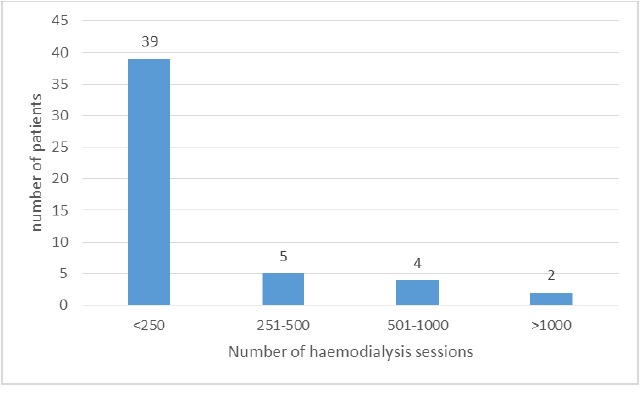
Among CKD patients with hearing loss, the majority received 250 or fewer haemodialysis sessions (Figure 2). The median number of haemodialysis sessions was significantly more in CKD patients without hearing loss (122 vs. 72, p=0.04).
Figure 2: Number of haemodialysis sessions in CKD patients with hearing loss.
Comparison of pure tone thresholds between CKD patients with and without hearing loss revealed that hearing loss was significant at low as well as high frequencies (Table 4).
Table 4:Distribution of hearing impairment at different frequency ranges among CKD patients with and without hearing loss.
| Frequency range | CKD patients with hearing loss (n=50) | CKD patients without hearing loss (n=70) | p value |
|---|---|---|---|
| Low frequencies | 33 | 0 | 0.001 |
| High frequencies | 50 | 43 | 0.001 |
| All frequencies | 45 | 7 | 0.001 |
Discussion
This study found that 41.7 per cent of CKD patients on haemodialysis had hearing loss, considerably higher than the normal population. In other words, every second or third CKD patient on haemodialysis experiences some degree of hearing impairment. The majority of these patients experienced mild hearing loss. Hearing thresholds were abnormal in CKD patients on haemodialysis across all frequencies ranging from 250Hz to 8 kHz. This study also showed that CKD patients with hearing loss received significantly fewer haemodialysis sessions compared to those without hearing loss. About one-half of CKD patients with hearing loss in our study had received ototoxic medications compared to one-third of CKD patients without hearing loss, suggesting a contributory role for ototoxic drugs in genesis of hearing loss in these patients.
The prevalence of hearing loss in CKD patients varies from 28 per cent to 77 per cent according to different studies.10,11 Notably, many older studies have shown higher prevalence of hearing loss, possibly due to small sample sizes. Hearing thresholds were abnormal at high frequencies in 77.5 per cent of CKD patients and at low frequencies in 27.5 per cent in our study. This is in contrast to the study by Gatland et al. who found 41 per cent hearing impairment in low frequencies and 53 per cent in high frequency range.12 Moreover, Qin and Gurbanov reported that the characteristic of hearing loss in CKD patients is high frequency abnormality.13,14
We also observed that hearing loss at high frequencies might be the most common audiometric abnormality in CKD patients, but not the typical one. This difference may be due to several reasons. First, the sample sizes in both studies were small (49 and 63 CKD patients, respectively). Second, Qin used high-frequency audiometry to assess the patients, possibly identifying patients with even mild abnormalities at higher frequencies not employed in conventional audiometry. Third, most of Gurbanov’s subjects had endstage renal disease, precluding generalisation of results to all CKD patients. In line with most previous studies, we too were unable to demonstrate any association between duration of CKD and hearing loss.1,15 Lasisi et al. were among the few to show that longer duration of CKD correlated with higher hearing thresholds (r=0.73, p=0.00387).16
A landmark study by Samir et al. provided evidence that haemodialysis per se might worsen hearing function.7 Subsequent studies by Nikolopoulos et al., Marsh et al., and Rossini et al. were unable, respectively, to arrive at a definite conclusion regarding the effect of haemodialysis on hearing in CKD.17–19 In contrast, Peyvandi et al. proposed in a recent study that prevalence and severity of hearing loss increases with duration of CKD and haemodialysis.20 Our finding that CKD patients with hearing loss received significantly fewer haemodialysis sessions is interesting as it suggests a possible beneficial association between increasing number of dialysis sessions and hearing loss. Thus, it is evident that there are data to indicate contributory as well as beneficial roles for haemodialysis on hearing in CKD patients.
The main limitation of this study was the cross-sectional observational design. We were not able to assess causation, although we found associations between hearing loss in CKD and several factors. However, the advantage offered by the large sample size (both CKD patients and controls) must be mentioned as its greatest strength.
This study, apart from its preliminary findings, also reveals the lacunae in our current understanding of hearing loss in CKD. Although there exists no further doubt that hearing loss is prevalent among CKD patients, well-designed studies with larger sample sizes are needed to elucidate the causal relationships between hearing loss in CKD and haemodialysis. Another logical question that arises in this context is whether a blanket audiometric screening of all CKD patients would help identify mild hearing loss and prevent progression to severe degrees, especially if a beneficial role for haemodialysis can be definitely established in long-term prospective studies. Besides, the association of hearing loss in CKD and ototoxic drugs needs to be addressed by more research as this could have significant implications for clinical practice
Conclusion
A mild degree of sensorineural hearing loss is quite common in CKD patients undergoing haemodialysis. Hearing loss in CKD patients does not follow any specific pattern and prevails at high and low frequencies. These patients are likely to be older and have a significantly greater exposure to ototoxic drugs. Duration of disease is not associated with hearing loss in CKD patients undergoing haemodialysis. However, haemodialysis may have an ameliorative effect on hearing loss in CKD, an association that needs to be tested further by long-term prospective studies.
ACKNOWLEDGEMENTS
We acknowledge Prof D. Balasundaram,vHead of Otorhinolaryngology and Dr Ilangovan and Dr Sanju, Department of Nephrology for their inputs and co-operation in this study.
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The authors declare the following conflict of interest: Dr Aneesh Basheer discloses that he is on the editorial board of the Australasian Medical Journal.
ETHICS COMMITTEE APPROVAL
Approval of the Pondicherry Institute of Medical Sciences Institute Ethics Committee (IEC/RC/12/66) was obtained prior to the study.
Please cite this paper as: Jamaldeen J, Basheer A, Sarma AC, Kandasamy R. Prevalence and patterns of hearing loss among chronic kidney disease patients undergoing haemodialysis. AMJ 2015;8(2):41–46.http://dx.doi.org/10.4066/AMJ.2015.2258
References
- 1.Jakic M, Mihaljevic D, Zibar L, Jakic M, Kotromanovic Z, Roguljic H. Sensorineural hearing loss in hemodialysis patients. Coll Antropol. 2010 Mar;34(1):165–71. [PubMed] [Google Scholar]
- 2.Vilayur E, Gopinath B, Harris DC, Burlutsky G, McMahon CM, Mitchell P. The association between reduced GFR and hearing loss: a cross-sectional population-based study. Am J Kidney Dis. 2010 Oct;56(4):661–9. doi: 10.1053/j.ajkd.2010.05.015. [DOI] [PubMed] [Google Scholar]
- 3.Cosgrove D, Samuelson G, Meehan DT, Miller C, McGee J, Walsh EJ. et al. Ultrastructural, physiological, and molecular defects in the inner ear of a gene-knockout mouse model for autosomal Alport syndrome. Hear Res. 1998 Jul;121((1-2)):84–98. doi: 10.1016/s0378-5955(98)00069-0. [DOI] [PubMed] [Google Scholar]
- 4.Ozturan O, Lam S. The effect of hemodialysis on hearing using pure-tone audiometry and distortion-product otoacoustic emissions. ORL J Otorhinolaryngol Relat Spec. 1998 Nov;60(6):306–13. doi: 10.1159/000027615. [DOI] [PubMed] [Google Scholar]
- 5.Adler D, Fiehn W, Ritz E. Inhibition of Na+,K+-stimulated ATPase in the cochlea of the guinea pig. A potential cause of disturbed inner ear function in terminal renal failure. Acta Otolaryngol. 1980;90((1-2)):55–60. doi: 10.3109/00016488009131697. [DOI] [PubMed] [Google Scholar]
- 6.Albertazzi A, Cappelli P, Di MT, Maccarone M, Di PB. The natural history of uremic neuropathy. Contrib Nephrol. 1988;65:130–7. doi: 10.1159/000415758. [DOI] [PubMed] [Google Scholar]
- 7.Samir M, Riad H, Mahgoub M, Awad Z, Kamal N. Transient otoacoustic emissions in children with chronic renal failure. Clin Otolaryngol Allied Sci. 1998 Feb;23(1):87–90. doi: 10.1046/j.1365-2273.1998.00117.x. [DOI] [PubMed] [Google Scholar]
- 8.Mancini ML, Dello SL, Bianchi PM, Tieri L, Rizzoni G. Sensorineural hearing loss in patients reaching chronic renal failure in childhood. Pediatr Nephrol. 1996 Feb;10(1):38–40. doi: 10.1007/BF00863438. [DOI] [PubMed] [Google Scholar]
- 9.Sharma R, Gaur S, Gautam P, Tiwari R, Narain A, Lalchandani T. A study on hearing evaluation in patients of chronic renal failure. Indian J Otol. 2011;17:109–12. [Google Scholar]
- 10.Meena RS, Aseri Y, Singh BK, Verma PC. Hearing loss in patients of chronic renal failure: a study of 100 cases. Indian J Otolaryngol Head Neck Surg. 2012 Dec;64(4):356–9. doi: 10.1007/s12070-011-0405-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bazzi C, Venturini CT, Pagani C, Arrigo G, D'Amico G. Hearing loss in short- and long-term haemodialysed patients. Nephrol Dial Transplant. 1995 Oct;10(10):1865–8. [PubMed] [Google Scholar]
- 12.Gatland D, Tucker B, Chalstrey S, Keene M, Baker L. Hearing loss in chronic renal failure-hearing threshold changes following haemodialysis. J R Soc Med. 1991 Oct;84(10):587–9. doi: 10.1177/014107689108401006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Qin Y, Sun Y, Zhai L, Lu H, Xu J. [Application of extended high frequency audiometry in the patients with chronic renal failure treated by hemodialysis]. Lin Chuang Er Bi Yan Hou Ke Za Zhi. 2005 Jan;19(1):17–8. [PubMed] [Google Scholar]
- 14.Gurbanov FA. [Hearing status in patients with pronounced chronic kidney insufficiency] Vestn Otorinolaringol. 1999;(2):39–41. [PubMed] [Google Scholar]
- 15.Henrich WL, Thompson P, Bergstrom LV, Lum GM. Effect of dialysis on hearing acuity. Nephron. 1977;18(6):348–51. doi: 10.1159/000180854. [DOI] [PubMed] [Google Scholar]
- 16.Lasisi AO, Salako BL, Kodiya MA, Amusat MA. Osisanya WP. Hearing threshold in patients with chronic renal failure. Saudi Med J. 2007 May;28(5):744–6. [PubMed] [Google Scholar]
- 17.Nikolopoulos TP, Kandiloros DC, Segas JV, Nomicos PN, Ferekidis EA, Michelis KE. et al. Auditory function in young patients with chronic renal failure. Clin Otolaryngol Allied Sci. 1997 Jun;(3):222–5. doi: 10.1046/j.1365-2273.1997.00890.x. [DOI] [PubMed] [Google Scholar]
- 18.Marsh JT, Brown WS, Wolcott D, Landsverk J, Nissenson AR. Electrophysiological indices of CNS function in hemodialysis and CAPD. Kidney Int. 1986 Dec;30(6):957–63. doi: 10.1038/ki.1986.279. [DOI] [PubMed] [Google Scholar]
- 19.Rossini PM, Di SE, Febbo A, Di PB, Basciani M. Brainstem auditory evoked responses (BAERs) in patients with chronic renal failure. Electroencephalogr Clin Neurophysiol. 1984 Jun;57(6):507–14. doi: 10.1016/0013-4694(84)90086-5. [DOI] [PubMed] [Google Scholar]
- 20.Peyvandi A, Roozbahany NA. Hearing loss in chronic renal failure patient undergoing hemodialysis. Indian J Otolaryngol Head Neck Surg. 2013 Dec;65(Suppl 3):537–40. doi: 10.1007/s12070-011-0454-9. [DOI] [PMC free article] [PubMed] [Google Scholar]