

Abstract
Background:
We are aware of limited data about the effects of purslane on diabetes. Earlier studies have mostly indicated the beneficial effects in animal models. This study aimed to evaluate the effect of purslane seeds on glycemic status and lipid profiles of persons with type 2 diabetes.
Materials and Methods:
This cross-over randomized controlled clinical trial was conducted on 48 persons with type 2 diabetes. Participants were randomly assigned to receive either 10 g/day purslane seeds with 240 cc low-fat yogurt (intervention group) or only 240 cc low-fat yogurt (as a control group) for 5 weeks. After a 2-week washout period, subjects were moved to the alternate arm for an additional 5 weeks. At baseline and end of each phase of the study, fasting blood samples were collected to quantify plasma glucose levels, as well as serum insulin and lipid profiles. Within-group and between-group changes in anthropometric measures, as well as biochemical indicators, were compared using a paired-samples t-test.
Results:
Mean age of study participants was 51.4 ± 6.0 year. We found a significant reduction in weight (−0.57 vs. 0.09 kg, P = 0.003) and body mass index (−0.23 vs. 0.02 kg/m2, P = 0.004) following purslane seeds consumption. Despite a slight reduction in fasting plasma glucose levels (−2.10 vs. −2.77 mg/dL, P = 0.90), we failed to find any significant effect on serum insulin levels and homeostatic model of assessment of insulin resistance score. Furthermore, purslane consumption decreased serum triglyceride levels (−25.5 vs. −1.8 mg/dL, P = 0.04) but could not affect serum high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and total cholesterol levels. We observed a significant reduction in systolic blood pressure (−3.33 vs. 0.5 mmHg, P = 0.01) and a borderline significant decrease in diastolic blood pressure (−3.12 vs. −0.93 mmHg, P = 0.09) after purslane seeds intake.
Conclusion:
In summary, consumption of purslane seeds for 5 weeks in persons with type 2 diabetes might improve their anthropometric measures, serum triglyceride levels, and blood pressure. Further studies are required to determine the appropriate dosage for these patients.
Keywords: Diabetes, glycemia, hyperlipidemia, medicinal plant, purslane
INTRODUCTION
Diabetes mellitus is a common prevalent chronic disease affecting thousands of people in both developed and developing countries.[1] It was estimated that the number of diabetic patients around the world will rise to 360 million in 2030.[2] In Iran, 7.7% of the adult population is affected.[3] Diabetes is associated with abnormalities that may lead to the development of nephropathy, retinopathy, neuropathy, and cardiovascular disease.[4,5,6] Due to the high cost imposed to the health care system, finding an efficient strategy for better management of diabetes has long been at the center of studies focused on diabetes.
The use of medicinal plants in the management of diabetes has a long history.[7] One of the most important medicinal plants is Portulaca oleracea, or purslane, which is a good source of biologically active compounds including omega-3 fatty acids and β-carotene[8] amino acids, α-tocopherols, ascorbic acid, glutathione,[9] and flavonoids compounds.[10] Several studies have demonstrated the beneficial effects of these compounds on metabolic profiles of persons with type 2 diabetes.[11,12,13,14,15] However, we are aware of limited data about the effects of purslane on diabetes. Earlier studies have indicated hypocholestrolemic[16,17] and hypoglycemic[18,19] effects of purslane in animal models. The beneficial effects of this medicinal plant on insulin resistance have also been shown in rats.[20] As clear, most previous studies have been limited to animal models and we are aware of only one clinical trial that has investigated the effect of purslane seed on lipid profile and glycemic status of persons with type 2 diabetes, in which consumption of 10 g/day of purslane seed for 8 weeks was comparable to 1500 mg/day metformin in influencing fasting plasma glucose (FPG) and serum insulin levels.[21]
It must be kept in mind that most persons with type 2 diabetes take oral hypoglycemic agents (OHAs) for their glycemic control. The additional effects of purslane seeds along with diabetic medications have not yet been assessed. Because of the limited information about the effects of purslane seeds on metabolic control of persons with type 2 diabetes, this study aimed to examine the effects of purslane seeds on lipid profiles and glycemic status of persons with type 2 diabetes.
PATIENTS AND METHODS
Participants
This study was a randomized cross-over clinical trial in which 48 subjects with type 2 diabetes aged 35-65 years, attending Endocrine Research Center of Isfahan University Medical Sciences, were included. This study was carried out in Isfahan, Iran, during January 2012 to July 2012. On the basis of sample size formula suggested for cross-over clinical trials,[22] we considered the type I error of 5% (α =0.05) and type II error of 10% (β = 0.20; Power = 80%) and FPG as a key variable. We reached the sample size of 38 patients for the whole trial. Given the high dropouts in cross-over trials, we enrolled 48 patients in the trial. Diagnosis of type 2 diabetes was done based on the criteria of American Diabetes Association;[23] those with one of the following criteria were considered as having diabetes: FPG ≥126 mg/dL, blood sugar 2-h postparandial ≥200 mg/dL. To be enrolled in the study, participants need to be a person with type 2 diabetes, who were nonsmokers, do not use alcohol, were nonpregnant and nonlactating women and those who did not change the dosage and type of medications in the last 2 months prior to the study. Individuals with a history of hepatic, renal, lung, and cardiovascular disease, as well as those with kidney stones, thyroid diseases, and gastrointestinal bleeding, were not included in the current study.
Totally, 48 persons with type 2 diabetes with the above-mentioned inclusion criteria were included in the study. The study was conducted according to the guidelines laid down in the declaration of Helsinki. All subjects completed written informed consent forms. The study protocol was approved by the Ethical Committee of Tehran University of Medical Sciences, Tehran, Iran and recorded by the identification code of IRCT201205272394N9 in clinical trials registry website of Iran.
Study design
Participants were randomly assigned to the initial arm of the study to receive either 10 g/day purslane seeds powder with 240 cc low-fat yogurt (intervention group) or only 240 cc low-fat yogurt (as control group) for 5 weeks [Figure 1]. A 2-week washout period was applied following which subjects were crossed over to the alternate treatment arm for an additional 5 weeks. We asked participants to add purslane seeds to low-fat yogurt to increase compliance and give a mixture with acceptable taste as well as to reduce its soluble oxalate content.[24] Portulaca oleracea does not have any cytotoxicity or genotoxicity effect, and it is safe for daily use.[25] Compliance was monitored once a week through phone interviews and double-checked by the counting of empty sachets. Participants were asked not to change their regular diet and routine physical activity levels during the study. If participants started insulin injection or changed the dosage and type of medications throughout the study, they were excluded from the study.
Figure 1.
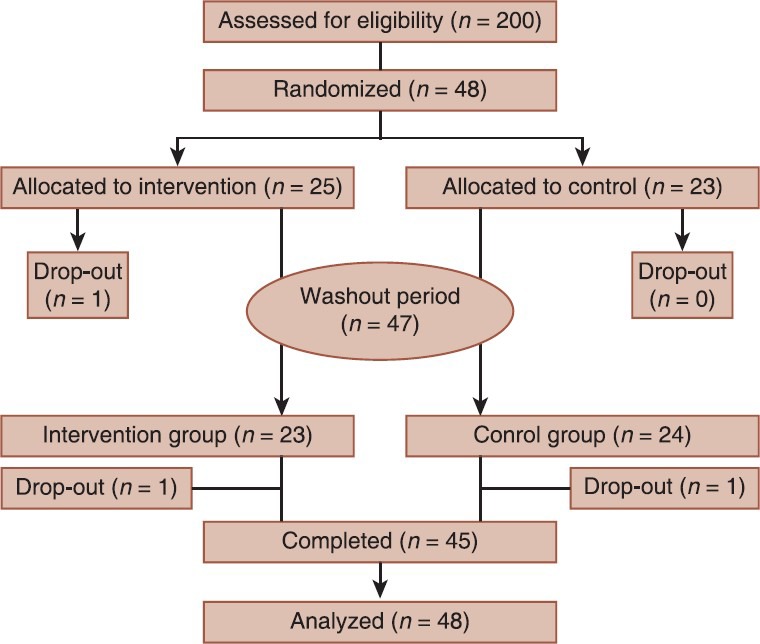
Participants’ flow diagram; intervention group received 10 g/day purslane seeds powder with 240 cc low-fat yogurt; the control group received only 240 cc low-fat yogurt
Purslane seeds were packed in 10 g sachets and were provided to participants at the start of the intervention. We assessed dietary intakes of subjects by the use of dietary records 3 times during each study phase. Nutritionist 4 (First Data Bank, San Bruno, CA, USA) was used to calculate nutrient intakes based on dietary records. Physical activity levels were also assessed through physical activity records during the study once every 2 weeks. Data from physical activity records were expressed as metabolic equivalent of task (MET)-h/day.[26]
Assessment of biochemical measures
At baseline and after each phase of the intervention, fasting blood samples were collected while the subjects were seated. Blood samples were taken according to a standard protocol and centrifuged within 30-45 min of collection. The analysis of samples was performed using Selectra-2 auto-analyzer (Vital Scientific, Spankeren, Netherlands). FPG was measured on the day of blood collection with an enzymatic colorimetric method using glucose oxidase. Serum triglyceride concentrations were assayed with the use of triglyceride kits (Pars AzmoonInc, Tehran, Iran). High-density lipoprotein cholesterol (HDL-C) levels were measured after precipitation of the apolipoprotein B-containing lipoproteins with phosphotungstic acid. Serum low-density lipoprotein cholesterol (LDL-C) levels were also measured using available kits. Serum insulin levels were measured by ELISA using enzyme-linked immunoassay kits. All inter- and intra-assay CVs for biochemical indicators were <5%. Homeostatic model of assessment of insulin resistance (HOMA-IR) was calculated based on the formula suggested by Matthews et al.[27]
Assessment of blood pressure
To measure blood pressure, participants were initially rested for 15 min and then we measured blood pressure with a standard mercury sphygmomanometer while the subjects were in a seated position. The systolic blood pressure was defined as the appearance of the first sound (Korotkoff phase 1), and the diastolic blood pressure was defined as the disappearance of the sound (Korotkoff phase 5) during deflation of the cuff at a 2-3 mm/s decrement rate of the mercury column.
Assessment of anthropometric measures
Weight was measured with a Seca scale while the subjects were minimally clothed and not wearing shoes. Height was measured while the subjects were standing and not wearing shoes by using a tape measure when the shoulders were in a normal position. Body mass index (BMI) was calculated and expressed as kg/m2. Waist circumference (WC) was measured at the narrowest level below the end of the lowest rib.
Statistical methods
To ensure the normal distribution of variables, Kolmogorov–Smirnov test was applied. The analyses were done based on intention-to-treat approach. Missing values were treated based on Last-observation-carried-forward method. Descriptive statistics (means, standard deviation, and range) for general characteristics of the study participants were reported. Data on dietary intakes were compared by paired t-test. For each dependent variable, we computed the changes from baseline by subtracting the baseline value from the end-of-trial value. With-in and between-group changes in dependent variables were compared by the use of paired samples t-test. We also assessed if the carry-over effect was significant. The carry-over effect was tested for by computing the average of the two treatments and comparing the two treatment orders using t-test. As we found no evidence of a carry-over effect, the participants with the two different orders were combined, and the treatment effect was tested for using the paired t-test, since each patient had each treatment. P < 0.05 was considered as statistically significant. All statistical analyses were done using the Statistical Package for Social Science version 16 (SPSS Inc., Chicago, Illinois, USA).
RESULTS
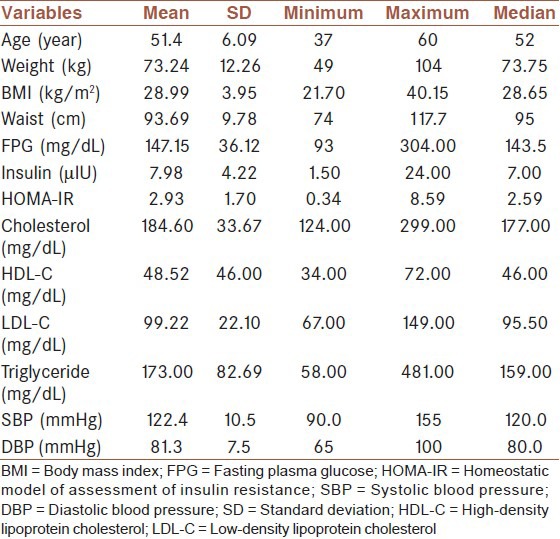
General characteristics of study participants are presented in Table 1. Mean age of subjects was 51.4 years. More than two-thirds of subjects were female and 58% were postmenopause. Almost one-third of the study participants were using dietary supplements throughout the study. All subjects were taking OHAs. Although no significant side effects were observed throughout the study, 12 patients had gastrointestinal problems when using the purslane seeds.
Table 1.
General characteristics of study participant at baseline (n = 48)
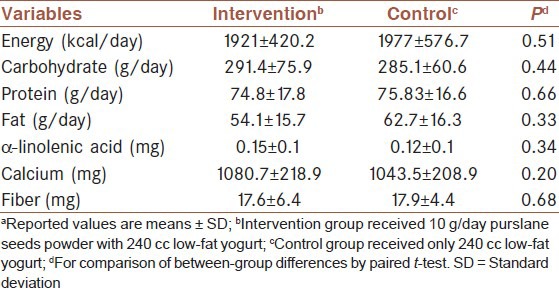
Comparison of dietary intakes of study participants throughout the study revealed no significant differences in macro and micro-nutrient intakes between the two groups [Table 2]. Participants were not significantly different in terms of physical activity levels during the study (32.7 vs. 32.3 MET-h/day, P = 0.34).
Table 2.
Dietary intakes of some nutrients throughout the studya
The effects of the intervention on anthropometric measures are shown in Table 3. Mean weight of the subject in the intervention group at study baseline was 71.2 kg. The intervention for 5 weeks led to a significant weight loss compared with the control (−0.57 vs. 0.09 kg, P = 0.003).
Table 3.
Effect of purslane on anthropometric measures of persons with type 2 diabetesa

Consumption of purslane seeds resulted in a significant reduction in BMI compared with the control group (−0.23 vs. 0.02 kg/m2, P = 0.004). Although the intervention resulted in a significant decrease in WC, there was no significant difference in WC changes comparing the two groups (−0.36 vs. 0.06 cm, P = 0.10).
The effects of the intervention on metabolic profiles of persons with type 2 diabetes are presented in Table 4. After 5 weeks of intervention, we observed 2 mg/dL decrease in FPG in both groups; however, comparing the changes between the two groups, we failed to find a significant difference (−2.10 vs. −2.77 mg/dL, P = 0.90). Neither within nor between-group changes in serum insulin levels and HOMA-IR score were significant following purslane seeds intake. Although both the intervention and control groups had a significant reduction in serum cholesterol levels, there were no significant differences in changes between the two groups. We also failed to find a significant effect of purslane seeds on serum HDL-C and LDL-C levels, neither within- nor between-groups.
Table 4.
Effect of purslane on metabolic profiles of persons with type 2 diabetesa
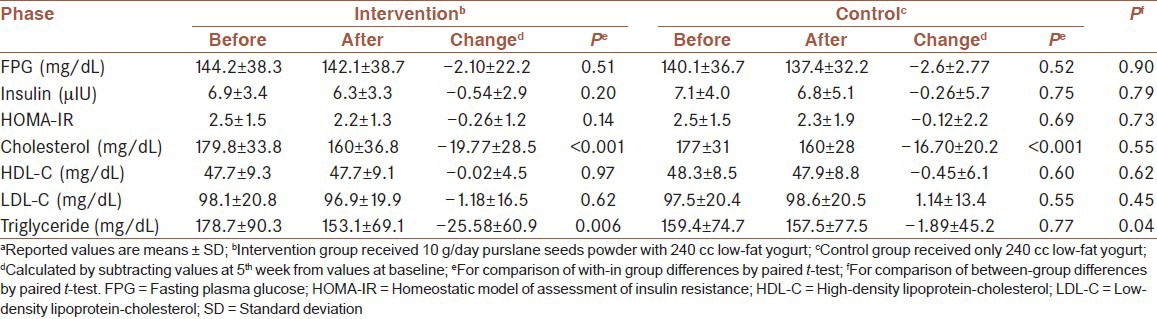
Purslane consumption for 5 weeks resulted in significant decreased levels of serum triglyceride. When we compared the changes between the two groups, we found a greater decrease of serum triglycerides following intervention than that from the control (−25.5 vs. −1.8 mg/dL, P = 0.04).
Within-group changes in the intervention group revealed a significant reduction in systolic and diastolic blood pressure after 5 weeks; however, no significant within-group changes were seen in the control group [Figure 2]. Comparing the changes between the two groups, we found a significant difference in changes in systolic blood pressure (−3.33 vs. 0.5 mmHg, P = 0.01) and a borderline significant (−3.12 vs. −0.93 mmHg, P = 0.09) in diastolic blood pressure between the two groups.
Figure 2.
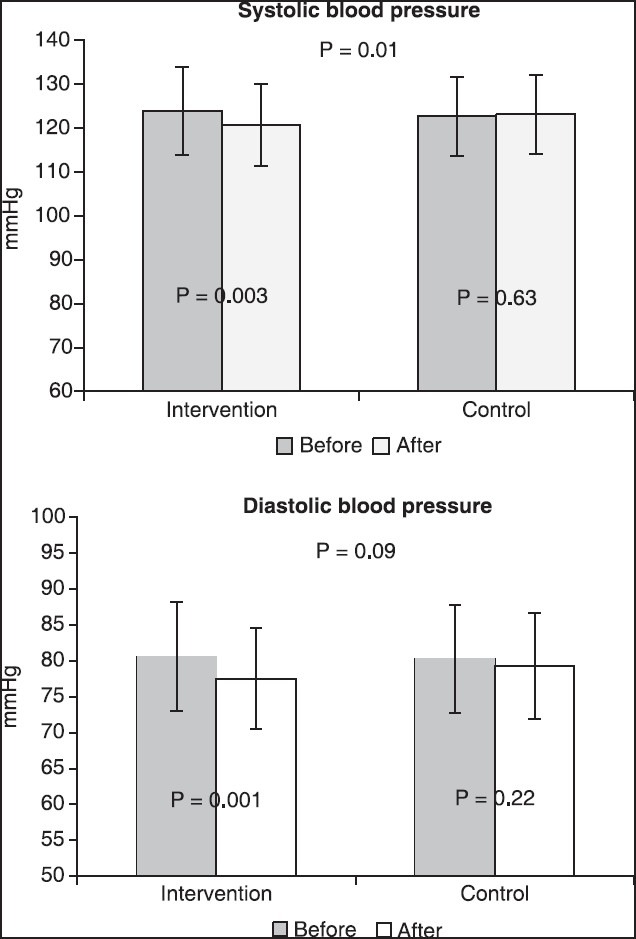
Effect of purslane consumption on blood pressure of persons with type 2 diabetes; intervention group received 10 g/day purslane seeds powder with 240 cc low-fat yogurt; control group received only 240 cc low-fat yogurt
DISCUSSION
This randomized cross-over clinical trial showed that purslane seeds consumption resulted in a significant reduction in weight and BMI. Despite a slight reduction in FPG levels, we failed to find any significant effect on serum insulin levels and HOMA-IR score following the purslane seeds intake. Furthermore, purslane seeds consumption decreased serum triglyceride levels but could not affect serum HDL-C, LDL-C, and total cholesterol levels. Consumption of purslane for 5 weeks led to a significant reduction in systolic blood pressure and a borderline significant decrease in diastolic blood pressure in persons with type 2 diabetes. To our knowledge, this study is among the first investigations examining the effects of purslane seeds intake on serum lipid profiles and glycemic status of persons with type 2 diabetes.
Recent research indicated that purslane, due to containing biologically active compounds, might have a favorable effect in human health.[28] We found that purslane seeds intake for 5 weeks could not affect FPG and serum insulin levels. This finding is in contrast to earlier studies done in animals and humans. Almost all experimental studies have indicated an antihyperglycemic effect of purslane consumption. In an experimental study, Gong et al.[18] showed a significant antihyperglycemic effect of purslane polysaccharides in diabetic rats. Other studies have indicated that the purslane extract might improve insulin resistance and hyperinsulinemia in diabetic rats.[20,29] However, few data are available indicating the effect of purslane on metabolic control of persons with type 2 diabetes in human beings. We are aware of just one report in humans in which El-Sayed[21] found that consumption of purslane in patients with type 2 diabetes, compared with the use of metformin, resulted in a significant reduction in FPG and serum insulin levels. Different findings of our study with others might be explained by the discrepancies in methodology. We used purslane seeds in this study, as El-Sayed did, but other studies used different preparations, like purslane leaves or extracts. The only processing that was done on purslane in our study was powdering. No evidence is available indicating that powdering can alter the composition of purslane. However, combination with yogurt might alter the bioavailability of some components of purslane. Furthermore, the cross-over design of our study might also provide some other explanations for discrepant findings. This is the first cross-over study reporting the effect of purslane seeds. Earlier studies have been experimental or parallel clinical trials. Discrepancy in duration of intervention, dosage of purslane used, study sample size along with compliance of the study participants to the purslane might also help explain the different findings.[18,19,21]
We found that purslane consumption led to a significant reduction in serum triglyceride levels but failed to influence serum HDL-C, LDL-C, and total cholesterol levels significantly. Antihyperlipidemic effects of purslane have earlier been reported by experimental studies.
Movahedian et al.[16] have reported that the use of the purslane extract might significantly reduce serum LDL-C and total cholesterol levels in rabbits fed a high cholesterol diet, but could not affect serum HDL-C. The same findings have also been shown in rats.[17] Few studies have also assessed the effects of purslane on lipid profiles of human. Consumption of 6 g/day freeze-dried purslane leaves in hypercholesterolemic subjects for 4 weeks led to improved total cholesterol levels while it did not influence serum triglycerides.[30] Others have also demonstrated the antihyperlipidemic effect of purslane leaves.[31] In the only available report on persons with type 2 diabetes, consumption of purslane seeds was associated with decreased levels of serum triglycerides, LDL-C, and total cholesterol levels.[21] Lack of any significant effect of purslane seeds on serum cholesterol levels in the current study might be attributed to the normal levels of serum lipids at the study baseline. Almost all earlier previous studies that reported the cholesterol-reducing effects of purslane, patients were hypercholesterolemic.
We found a significant reduction in systolic blood pressure and a borderline significant decrease in diastolic blood pressure after purslane intake. No earlier study has reported the effect of purslane intake on blood pressure and to the best of our knowledge, this study is the first reporting the beneficial effects of purslane seeds intake on blood pressure. However, the effect of omega-3 fat intake on blood pressure has been shown by previous investigations.[32] Given the beneficial effect of purslane on blood pressure, the inclusion of this medicinal plant in dietary management of hypertension could be recommended. However, to reach a definite conclusion in this regard further studies are warranted.
The mechanisms through which purslane intake might affect glycemic status and lipid profiles of persons with type 2 diabetes have been unknown. Several mechanisms might explain its beneficial effects. The weight reduction might be due to the effect of purslane seeds on insulin resistance.[21] Some documents have also attributed the lipolytic effect of purslane to its content of nor-adrenaline.[33] Antihyperglycemic effect of purslane could be attributed to its effect on increased insulin secretion through closing the K+/ATP channels, influencing membrane depolarization and Ca2+ entry.[34] Another study showed that purslane seeds intake could significantly increase glucagon-like peptide-1 levels in persons with type 2 diabetes.[19,35] Purslane seeds contain high amounts of flavonoids.[10,36] The beneficial effects of flavonoids on serum lipid profiles have earlier been shown.[37,38] The effect of purslane intake on lowering serum triglyceride levels might be explained by its high content of omega-3 fatty acids as reported in previous studies.[39,40]
Our findings should be interpreted while considering some limitations. It must be kept in mind that some biomarkers including FPG, HOMA-IR, insulin, total and HDL-C levels were reduced in both intervention and control groups slightly. This indicates that the patients may not be tightly controlled prior to the commencement of the research or were newly diagnosed and did not reach the desired levels of serum biomarkers. This fact might influence our findings and should be considered in the interpretation of the study results. One of our study limitations is the method of assessment of compliance to purslane seeds intake. We assessed compliance through phone interview as well as asking participants to deliver the empty sachets to study personnel. Future studies are better to assess the compliance through the use of an appropriate biomarker. Although findings a suitable biomarker for purslane intake is difficult, measurement of the alpha-linolenic acid content of red blood cells’ membranes might provide some information in this regard. Another limitation of our study is the short duration of intervention. Longer intervention periods might lead to a greater number of dropouts; however, the effects might better be reflected in such interventions. Single measurement of metabolic profile in the current study might lead to misleading findings due to day-to-day variations in these biomarkers. Limited patients who had not a good control of their blood glucose which can effect on our results. Unfortunately, we were not considered duration of diabetes in participants that might influence on finding of the study.
CONCLUSION
This cross-over clinical trial revealed that consumption of purslane seeds for 5 weeks in persons with type 2 diabetes might improve their anthropometric measures, serum triglyceride levels, and blood pressure. Further studies are required to determine the appropriate dosage for these patients.
AUTHOR'S CONTRIBUTION
AE, ShJ and EZ contributed to conception, design, statistical analysis and manuscript drafting. EZ and EF contributed to the data collection. MG supervised statically analysis. AE supervised the study. All author approved the final manuscript for submission.
ACKNOWLEDGMENTS
The present study was supported by Vice-Chancellor for Research, Tehran University of Medical Sciences, Tehran, Iran. We would like to thank Mrs. Saneei, PhD candidate of nutrition in the Isfahan University of Medical Sciences, and Mrs. Tabatabaei for their assistance. We also appreciate the cooperation made by the staff of Endocrine and Metabolism Research Center of Isfahan University of Medical Sciences. Research project number is 18096.
Footnotes
Source of Support: Nil
Conflict of Interest: No conflict of interests.
REFERENCES
- 1.Maiti R, Jana D, Das UK, Ghosh D. Antidiabetic effect of aqueous extract of seed of Tamarindus indica in streptozotocin-induced diabetic rats. J Ethnopharmacol. 2004;92:85–91. doi: 10.1016/j.jep.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 2.Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi: 10.1016/j.diabres.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Esteghamati A, Gouya MM, Abbasi M, Delavari A, Alikhani S, Alaedini F, et al. Prevalence of diabetes and impaired fasting glucose in the adult population of Iran: National Survey of Risk Factors for Non-Communicable Diseases of Iran. Diabetes Care. 2008;31:96–8. doi: 10.2337/dc07-0959. [DOI] [PubMed] [Google Scholar]
- 4.Bate KL, Jerums G. 3: Preventing complications of diabetes. Med J Aust. 2003;179:498–503. doi: 10.5694/j.1326-5377.2003.tb05655.x. [DOI] [PubMed] [Google Scholar]
- 5.Das K, Dang R, Bhaskaran S, Roopashree T, Singh V, Govil J, et al. Recent advances in medicinal plants in diabetes treatment. Phytopharmacology and therapeutic values I. 2008;19:151–91. [Google Scholar]
- 6.Watkins PJ. ABC of diabetes: Retinopathy. BMJ. 2003;326:924–6. doi: 10.1136/bmj.326.7395.924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akhtar MS, Ali MR. Study of anti diabetic effect of a compound medicinal plant prescription in normal and diabetic rabbits. J Pak Med Assoc. 1984;34:239–44. [PubMed] [Google Scholar]
- 8.Liu L, Howe P, Zhou YF, Xu ZQ, Hocart C, Zhan R. Fatty acids and beta-carotene in australian purslane (Portulaca oleracea) varieties. J Chromatogr A. 2000;893:207–13. doi: 10.1016/s0021-9673(00)00747-0. [DOI] [PubMed] [Google Scholar]
- 9.Simopoulos AP, Norman HA, Gillaspy JE, Duke JA. Common purslane: A source of omega-3 fatty acids and antioxidants. J Am Coll Nutr. 1992;11:374–82. doi: 10.1080/07315724.1992.10718240. [DOI] [PubMed] [Google Scholar]
- 10.Zhang Y, Chen J, Ma XM, Shi YP. Simultaneous determination of flavonoids in Ixeridium gracile by micellar electrokinetic chromatography. J Pharm Biomed Anal. 2007;45:742–6. doi: 10.1016/j.jpba.2007.08.014. [DOI] [PubMed] [Google Scholar]
- 11.Popp-Snijders C, Schouten JA, Heine RJ, van der Meer J, van der Veen EA. Dietary supplementation of omega-3 polyunsaturated fatty acids improves insulin sensitivity in non-insulin-dependent diabetes. Diabetes Res. 1987;4:141–7. [PubMed] [Google Scholar]
- 12.Song Y, Manson JE, Buring JE, Sesso HD, Liu S. Associations of dietary flavonoids with risk of type 2 diabetes, and markers of insulin resistance and systemic inflammation in women: A prospective study and cross-sectional analysis. J Am Coll Nutr. 2005;24:376–84. doi: 10.1080/07315724.2005.10719488. [DOI] [PubMed] [Google Scholar]
- 13.Hasanain B, Mooradian AD. Antioxidant vitamins and their influence in diabetes mellitus. Curr Diab Rep. 2002;2:448–56. doi: 10.1007/s11892-002-0110-6. [DOI] [PubMed] [Google Scholar]
- 14.Levy Y, Zaltsberg H, Ben-Amotz A, Kanter Y, Aviram M. Dietary supplementation of a natural isomer mixture of beta-carotene inhibits oxidation of LDL derived from patients with diabetes mellitus. Ann Nutr Metab. 2000;44:54–60. doi: 10.1159/000012821. [DOI] [PubMed] [Google Scholar]
- 15.Pazdro R, Burgess JR. The role of vitamin E and oxidative stress in diabetes complications. Mech Ageing Dev. 2010;131:276–86. doi: 10.1016/j.mad.2010.03.005. [DOI] [PubMed] [Google Scholar]
- 16.Movahedian A, Ghannadi A, Vashirnia M. Hypocholesterolemic effects of purslane extract on serum lipids in rabbits fed with high cholesterol levels. Int J Pharmacol. 2007;3:285–9. [Google Scholar]
- 17.Changizi-Ashtiyani S, Zarei A, Taheri S, Rasekh F, Ramazani M. The effects of Portulaca oleracea alcoholic extract on induced hypercholesteroleomia in rats. Zahedan J Res Med Sci. 2013;15:34–9. [Google Scholar]
- 18.Gong F, Li F, Zhang L, Li J, Zhang Z, Wang G. Hypoglycemic effects of crude polysaccharide from Purslane. Int J Mol Sci. 2009;10:880–8. doi: 10.3390/ijms10030880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Heidarzadeh S, Farzanegi P, Azarbayjani MA, Daliri R. Purslane effect on GLP-1 and GLP-1 receptor in type 2 diabetes. Electron Physician. 2013;5:582–7. doi: 10.14661/2013.582-587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lan S, Fu-er L. Effects of Portulaca oleracea on insulin resistance in rats with type 2 diabetes mellitus. Chin J Integr Med. 2003;9:289–92. [Google Scholar]
- 21.El-Sayed MI. Effects of Portulaca oleracea L. seeds in treatment of type-2 diabetes mellitus patients as adjunctive and alternative therapy. J Ethnopharmacol. 2011;137:643–51. doi: 10.1016/j.jep.2011.06.020. [DOI] [PubMed] [Google Scholar]
- 22.Fleiss JL. Hoboken, New Jersey: Wiley-Interscience; 2011. Design and Analysis of Clinical Experiments. [Google Scholar]
- 23.American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010;33(Suppl 1):S62–9. doi: 10.2337/dc10-S062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Moreau AG, Savage G. Oxalate content of purslane leaves and the effect of combining them with yoghurt or coconut products. J Food Compost Anal. 2009;22:303–6. [Google Scholar]
- 25.Yen GC, Chen HY, Peng HH. Evaluation of the cytotoxicity, mutagenicity and antimutagenicity of emerging edible plants. Food Chem Toxicol. 2001;39:1045–53. doi: 10.1016/s0278-6915(01)00053-9. [DOI] [PubMed] [Google Scholar]
- 26.Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: An update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32:S498–504. doi: 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- 27.Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9. doi: 10.1007/BF00280883. [DOI] [PubMed] [Google Scholar]
- 28.Oliveira I, Valentão P, Lopes R, Andrade PB, Bento A, Pereira JA. Phytochemical characterization and radical scavenging activity of Portulaca oleraceae L. leaves and stems. Microchem J. 2009;92:129–34. [Google Scholar]
- 29.Abdalla HM., Jr Purslane extract effects on obesity-induced diabetic rats fed a high-fat diet. Malays J Nutr. 2010;16:419–29. [PubMed] [Google Scholar]
- 30.Besong S, Ezekwe M, Ezekwe E. Evaluating the effects of freeze-dried supplements of purslane (Portulaca oleracea) on blood lipids in hypercholesterolemic adults. Int J Nutr Metab. 2011;3:43–9. [Google Scholar]
- 31.Gatreh-Samani K, Farrokhi E, Khalili B, Rafieian M, Moradi M. Purslane (Portulaca oleracea) effects on serum paraoxanase-1 activity. J Shahrekord Univ Med Sci. 2011;13:9–14. [Google Scholar]
- 32.Mori TA. Omega-3 fatty acids and hypertension in humans. Clin Exp Pharmacol Physiol. 2006;33:842–6. doi: 10.1111/j.1440-1681.2006.04451.x. [DOI] [PubMed] [Google Scholar]
- 33.Dweck A. Purslane (Portulaca oleracea)-the global panacea. Pers Care Mag. 2001;2:7–15. [Google Scholar]
- 34.Ryle PR, Barker J, Gaines PA, Thomson AD, Chakraborty J. Alloxan-induced diabetes in the rat – protective action of (−) epicatechin? Life Sci. 1984;34:591–5. doi: 10.1016/0024-3205(84)90493-4. [DOI] [PubMed] [Google Scholar]
- 35.Lim GE, Brubaker PL. Glucagon-like peptide 1 secretion by the L-cell the view from within. Diabetes. 2006;55(Suppl 2):S70–7. [Google Scholar]
- 36.Xu X, Yu L, Chen G. Determination of flavonoids in Portulaca oleracea L. by capillary electrophoresis with electrochemical detection. J Pharm Biomed Anal. 2006;41:493–9. doi: 10.1016/j.jpba.2006.01.013. [DOI] [PubMed] [Google Scholar]
- 37.da Silva RR, de Oliveira TT, Nagem TJ, Pinto AS, Albino LF, de Almeida MR, et al. Hypocholesterolemic effect of naringin and rutin flavonoids. Arch Latinoam Nutr. 2001;51:258–64. [PubMed] [Google Scholar]
- 38.Hertog MG, Feskens EJ, Hollman PC, Katan MB, Kromhout D. Dietary antioxidant flavonoids and risk of coronary heart disease: The Zutphen Elderly Study. Lancet. 1993;342:1007–11. doi: 10.1016/0140-6736(93)92876-u. [DOI] [PubMed] [Google Scholar]
- 39.McKenney JM, Sica D. Prescription omega-3 fatty acids for the treatment of hypertriglyceridemia. Am J Health Syst Pharm. 2007;64:595–605. doi: 10.2146/ajhp060164. [DOI] [PubMed] [Google Scholar]
- 40.Skulas-Ray AC, Kris-Etherton PM, Harris WS, Vanden Heuvel JP, Wagner PR, West SG. Dose-response effects of omega-3 fatty acids on triglycerides, inflammation, and endothelial function in healthy persons with moderate hypertriglyceridemia. Am J Clin Nutr. 2011;93:243–52. doi: 10.3945/ajcn.110.003871. [DOI] [PMC free article] [PubMed] [Google Scholar]