

Abstract
Background:
Considering the effectiveness of craniofacial photographic analysis for diagnosis and management of obstructive sleep apnea-hypopnea syndrome (OSAHS) as well as ethnic differences in indexes measured by this method, this study designed to compare the surface facial dimensions, including nose width, intercanthal width and mandibular width of Iranian patients with mild, moderate and severe OSAHS.
Materials and Methods:
In this cross sectional study subjects with mild, moderate and severe OSAHS based on apnea-hypopnea index, were studied. To determine cephalometric measurements, face and neck digital photographs were taken from participants following a standardized procedure. Cephalometric measurements including face, intercanthal and mandibular widths were compared between studied groups.
Results:
In this study, 100 participants enrolled. From which 20 (20.8%), 35 (36.45%) and 41 (42.7%) of them had mild, moderate and severe OSAHS, respectively. Mean of nose, intercanthal and mandibular width were significantly higher in patients with severe OSAHS than those with mild or moderate OSAHS (P < 0.05). In both genders, mandibular width were higher in severe forms of OSAHS. Disease severity was significantly associated with increased age and mandibular width (P < 0.05).
Conclusion:
Mandibular width was the most important index, which had a significant association with the disease severity. It seems that our results could be used both for diagnosis and follow-up of OSAHS management. They could be used as baseline information as well as a clinical and research tool in the field of OSAHS.
Keywords: Intercanthal, mandible, nose, obstructive sleep apnea hypopnea syndrome, severity
INTRODUCTION
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is characterized by coexistence of daytime sleepiness with at least five apnea or hypopnea per hour of sleep.[1] This condition occurs in around 1-4% of middle-aged males.[2,3,4]
In patients with OSAHS, airway narrowing and decrease in its muscle tone lead to airway obstruction.[1] In addition, the patients are at increased of hypertension, diabetes mellitus, hepatic dysfunction, somnolence, nocturia and nocturnal choking.[5]
Though the most important risk factor in the pathogenesis of OSAHS is obesity, but there are growing the body of evidences that indicated that craniofacial morphology also considered as an important interacting factor in this regard.[6,7,8]
Computed tomography, magnetic resonance imaging (MRI) and cephalometry are the most accurate diagnostic tools, which provide details of bony and soft tissue structures properly. These methods commonly used for research applications due to their higher cost, radiation exposure and time-consuming analysis. Thus, the use of some noninvasive alternative methods including craniofacial anthropometry and photogrammetry has been developed recently. Accordingly the later methods have not the limitation of previous methods. Recently photogrammetry has become as one of the favorable methods due to its noninvasively and readily accessibility.[9,10]
Several investigations revealed significant differences in craniofacial morphological parameters of subjects with and without OSAHS.[11]
It is recognized from these studies that the correlation between the number of surface facial dimensions and upper airway structures and craniofacial morphology appear useful for prediction of OSAHS.[12,13] Moreover, these craniofacial features differ between ethnic populations.[14,15]
Hence, considering the effectiveness of mentioned assay for diagnosis and management of the disease as well as ethnic differences in indexes measured by this method, this study designed to compare the surface facial dimensions, including nose width, intercanthal width and mandibular width of Iranian patients with mild, moderate and severe OSAHS.
MATERIALS AND METHODS
In this cross sectional study, subjects complaining of snoring, daytime sleepiness and dyspnea referred to a private sleep disorder clinic for polysomnography from January 2013 to December 2013 were enrolled.
The protocol of the study was approved by the Regional Ethics Committee of the Isfahan University of Medical Sciences (research project number: 392294).
From selected subjects those with craniofacial anomalies associated with syndromes (such as apert and crouzon), excessive facial hair, previous facial trauma which affected facial landmarks, systemic disease (such as renal failure, thyroid dysfunction) and psychiatric disorders were excluded from the study. From which those with apnea/hypopnea index (AHI) values >5 diagnosed as those with OSAHS were selected finally. Selected patients underwent full overnight polysomnography and based on the AHI they classified in three groups of severity of the disease as follows; mild (5≤ AHI <15), moderate (15≤ AHI <30) and severe (30≤ AHI).[16] To determine cephalometric measurements, face and neck digital photographs were taken from participants following a standardized procedure on the same day as the polysomnography. Cephalometric measurements were compared between studied groups.
Cephalometric measurements
Photographs obtained with the patients seated upright in a straight ahead and in the extended head position using a single lens reflex digital camera (SX 220 HS 50-70 mm lens; Canon, Japan). Bony landmarks were preidentified in the patients by palpation and marked with red tapes. Pixel measurements were converted to metric dimensions using image analysis software (image J1, 44p; java1.6.0-20 [32-bit], 41scommands; 58 macros).
These measurements represented mandibular width (distance between right mandibular angle and left mandibular angle), intercanthal width and nose width.
Statistical analysis
Data analyzed using SPSS version 20 (SPSS Inc., Chicago, IL, USA) software. Continuous and categorical variables were presented as mean (standard deviation) or median (25th and 75th percentiles) and number (%), respectively. Shapiro–Wilk test was used to determine the normal distribution of studied variables. Continuous and categorical variables in studied groups were compared using Kruskal–Wallis and Chi-square tests, respectively value <0.05 considered statistically significant.
RESULTS
Totally 100 participants were enrolled in this study. According to the findings of polysomnograghy 4 of them were cases of simple snorers, and they had <5 episodes of apnea/hypopnea per hour while the other 96 patients were diagnosed with OSAHS. Mean age of patients with OSAHS was 48.6 ± 12.3 with a male:female ratio of 2:1. From studied population 20 (20.8%), 35 (36.45%) and 41 (42.7%) of them had mild, moderate and severe OSAHS, respectively.
Demographic characteristics and cephalometric measurements of studied population in three subgroups of OSAHS are presented in Table 1. Accordingly patients with moderate to severe OSAHS were significantly older than milder ones. Mean of nose, intercanthal and mandibular width were significantly higher in patients with severe OSAHS than those with mild or moderate OSAHS (P < 0.05).
Table 1.
Demographics characteristics and cephalometric measurements of patients with mild, moderate and severe OSAHS

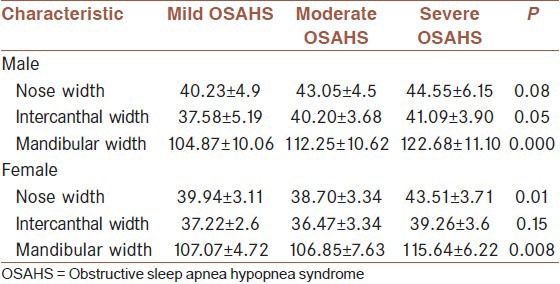
Cephalometric measurements of studied population in three subgroups of OSAHS according to sex groups are presented in Table 2. In both genders, mandibular width were higher in severe forms of OSAHS.
Table 2.
Cephalometric measurements of studied population in three subgroups of OSAHS according to sex groups
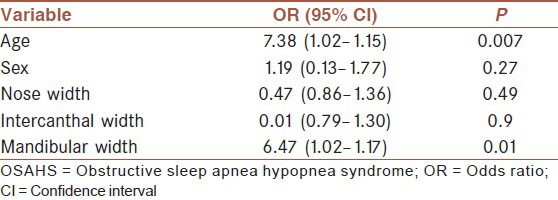
The relation between studied cephalometric measurements and severity of OSAHS using logistic regression are presented in Table 3. Accordingly disease severity was associated with increased age and mandibular width.
Table 3.
The relation between studied cephalometric measurements and severity of OSAHS
DISCUSSION
In this study, differences between phenotypic craniofacial indexes performed using craniofacial photogrammetry technique among patients with different degree of OSAHS. The results demonstrated increased value of nose, intercanthal and mandibular width in patients with severe OSAHS. Severity of the disease was significantly associated with increased age and mandibular width.
In this study, we used craniofacial photogrammetry method among Iranian population.
Though the method which is used in this study is not the gold standard diagnostic tool in this regard, but some of its advantages including its availability, safety, inexpensiveness and quick made results made it as a feasible technique. Moreover, evidences confirmed that it captures both skeletal anatomy and soft tissues and different indexes measured by this method allow quantification of the surface morphology.[17] These mentioned advantages could not assess by other imaging techniques.
Several researches worldwide showed that the measures are different in various ethnic groups.[18,19] Lee et al. reported that the Chinese had more craniofacial bony restriction than Caucasian in the same degree of OSAHS severity.[19]
Most reported studies in this field have compared phenotypical craniofacial indexes among patients with OSAHS and a group of healthy subjects. There were few studies regarding the association of the indexes and OSAHA according to the disease severity. Previous researches that indicated the relationship between craniofacial measurements and OSAHS severity mostly used the neck measurements. They suggested that from craniofacial measurements face and mandibular width may be useful for evaluating OSAHS severity.[20]
In this study, we compare the indexes in patients with different degree of OSAHS. The implication of our results could be used for diagnosis, treatment and follow-up of patients with OSAHS. In our study though mean of nose, intercanthal and mandibular width in patients with severe OSAHS were significantly higher than moderate and mild form of the disease, but logistic regression showed that from mentioned indexes only mandibular width had significant association with severity of the disease. The importance of mandibular index measured both by MRI and phenotypical craniofacial measurements in patients with OSAHS have been reported in many studies.[20,21]
The method was first described by Lee et al. In a case-control study, they have investigated the craniofacial morphological phenotype of patients with OSAHS and a control group. In their primary analysis, patients have higher measurements of mandible (13.0 ± 0.11 vs. 12.3 ± 0.12), intercanthal (3.50 ± 0.04 vs. 3.27 ± 0.05) and nose (3.97 ± 0.04 vs. 3.72 ± 0.05) width than control group.[20]
Comparing their measurements with ours, it seems that Iranian patients with OSAHS had lower mandibular width and higher nose and intercanthal width than Australian population. Iranian patients with moderate to severe OSAHS had increased value of mentioned measurements than those with a mild form of the disease.
Albajalan et al. have indicated that Malay subjects with moderate-severe OSAHS had a shorter maxillary and mandibular length when compared with a mild OSAHS sample.[22]
Regarding sex differences the results of the current study showed that the mandibular width was higher in severe forms of the disease both in male and female, but reminder indexes were not similar in both genders. It seems that the results would be more accurate with larger sample size.
In this study, there was a significant association between increasing age and severity of OSAHS. Lam et al. in Canada also have indicated that patients with obstructive sleep apnea were older than healthy subjects.[23]
The limitations of this study were small sample size, lack of a control group and lack of lateral dimensions of craniofacial structures.
In sum, the findings of the current study indicated the phenotypic craniofacial differences among patients with different severity of OSAHS using the novel method of craniofacial photographic analysis. Mandibular width was the most important index which had a significant association with the disease severity. It seems that our results could be used both for diagnosis and follow-up of OSAHS management. Our results could be used as baseline information as well as a clinical and research tool in the field of OSAHS. It is recommended to design further studies with consideration of mentioned limitation for obtaining more conclusive results in this regard.
AUTHOR'S CONTRIBUTION
BA, AP, EA, TP, IF and MG contributed to the design of the work. MA analyzed data and interpreted the work. AP and EA drafted the work. BA, AP, EA, MA, and TP were involved in revising article. All authors approved the version to be published and agreed to be accountable for all aspects of the work.
ACKNOWLEDGMENTS
We thank the University authorities who offered critical administrative support and managerial services in carrying out the study, and also all of the researchers for their help and support. This paper was derived from a research project (research project number; 392294) approved by School of Medicine, Isfahan University of Medical Sciences.
Footnotes
Source of Support: Isfahan University of Medical Sciences (research project number: 392294).
Conflict of Interest: None declared.
REFERENCES
- 1.Fogel RB, Malhotra A, Dalagiorgou G, Robinson MK, Jakab M, Kikinis R, et al. Anatomic and physiologic predictors of apnea severity in morbidly obese subjects. Sleep. 2003;26:150–5. doi: 10.1093/sleep/26.2.150. [DOI] [PubMed] [Google Scholar]
- 2.Hui DS, Ko FW, Chan JK, To KW, Fok JP, Ngai JC, et al. Sleep-disordered breathing and continuous positive airway pressure compliance in a group of commercial bus drivers in Hong Kong. Respirology. 2006;11:723–30. doi: 10.1111/j.1440-1843.2006.00932.x. [DOI] [PubMed] [Google Scholar]
- 3.Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. doi: 10.1056/NEJM199304293281704. [DOI] [PubMed] [Google Scholar]
- 4.Kim J, In K, Kim J, You S, Kang K, Shim J, et al. Prevalence of sleep-disordered breathing in middle-aged Korean men and women. Am J Respir Crit Care Med. 2004;170:1108–13. doi: 10.1164/rccm.200404-519OC. [DOI] [PubMed] [Google Scholar]
- 5.Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol (1985) 2005;99:1592–9. doi: 10.1152/japplphysiol.00587.2005. [DOI] [PubMed] [Google Scholar]
- 6.Okubo M, Suzuki M, Horiuchi A, Okabe S, Ikeda K, Higano S, et al. Morphologic analyses of mandible and upper airway soft tissue by MRI of patients with obstructive sleep apnea hypopnea syndrome. Sleep. 2006;29:909–15. doi: 10.1093/sleep/29.7.909. [DOI] [PubMed] [Google Scholar]
- 7.Miles PG, Vig PS, Weyant RJ, Forrest TD, Rockette HE., Jr Craniofacial structure and obstructive sleep apnea syndrome – a qualitative analysis and meta-analysis of the literature. Am J Orthod Dentofacial Orthop. 1996;109:163–72. doi: 10.1016/s0889-5406(96)70177-4. [DOI] [PubMed] [Google Scholar]
- 8.Lowe AA, Fleetham JA, Adachi S, Ryan CF. Cephalometric and computed tomographic predictors of obstructive sleep apnea severity. Am J Orthod Dentofacial Orthop. 1995;107:589–95. doi: 10.1016/s0889-5406(95)70101-x. [DOI] [PubMed] [Google Scholar]
- 9.Todd ES, Weinberg SM, Berry-Kravis EM, Silvestri JM, Kenny AS, Rand CM, et al. Facial phenotype in children and young adults with PHOX2B-determined congenital central hypoventilation syndrome: Quantitative pattern of dysmorphology. Pediatr Res. 2006;59:39–45. doi: 10.1203/01.pdr.0000191814.73340.1d. [DOI] [PubMed] [Google Scholar]
- 10.Kitano I, Park S, Kato K, Nitta N, Takato T, Susami T. Craniofacial morphology of conotruncal anomaly face syndrome. Cleft Palate Craniofac J. 1997;34:425–9. doi: 10.1597/1545-1569_1997_034_0425_cmocaf_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 11.Hui DS. Craniofacial profile assessment in patients with obstructive sleep apnea. Sleep. 2009;32:11–2. [PMC free article] [PubMed] [Google Scholar]
- 12.Benumof JL. Obstructive sleep apnea in the adult obese patient: Implications for airway management. J Clin Anesth. 2001;13:144–56. doi: 10.1016/s0952-8180(01)00232-x. [DOI] [PubMed] [Google Scholar]
- 13.Sforza E, Bacon W, Weiss T, Thibault A, Petiau C, Krieger J. Upper airway collapsibility and cephalometric variables in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2000;161:347–52. doi: 10.1164/ajrccm.161.2.9810091. [DOI] [PubMed] [Google Scholar]
- 14.Wong ML, Sandham A, Ang PK, Wong DC, Tan WC, Huggare J. Craniofacial morphology, head posture, and nasal respiratory resistance in obstructive sleep apnoea: An inter-ethnic comparison. Eur J Orthod. 2005;27:91–7. doi: 10.1093/ejo/cjh077. [DOI] [PubMed] [Google Scholar]
- 15.Cakirer B, Hans MG, Graham G, Aylor J, Tishler PV, Redline S. The relationship between craniofacial morphology and obstructive sleep apnea in whites and in African-Americans. Am J Respir Crit Care Med. 2001;163:947–50. doi: 10.1164/ajrccm.163.4.2005136. [DOI] [PubMed] [Google Scholar]
- 16.Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep. 1999;22:667–89. [PubMed] [Google Scholar]
- 17.Lee RW, Sutherland K, Chan AS, Zeng B, Grunstein RR, Darendeliler MA, et al. Relationship between surface facial dimensions and upper airway structures in obstructive sleep apnea. Sleep. 2010;33:1249–54. doi: 10.1093/sleep/33.9.1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hui DS, Ko FW, Chu AS, Fok JP, Chan MC, Li TS, et al. Cephalometric assessment of craniofacial morphology in Chinese patients with obstructive sleep apnoea. Respir Med. 2003;97:640–6. doi: 10.1053/rmed.2003.1494. [DOI] [PubMed] [Google Scholar]
- 19.Lee RW, Vasudavan S, Hui DS, Prvan T, Petocz P, Darendeliler MA, et al. Differences in craniofacial structures and obesity in Caucasian and Chinese patients with obstructive sleep apnea. Sleep. 2010;33:1075–80. doi: 10.1093/sleep/33.8.1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lee RW, Chan AS, Grunstein RR, Cistulli PA. Craniofacial phenotyping in obstructive sleep apnea – a novel quantitative photographic approach. Sleep. 2009;32:37–45. [PMC free article] [PubMed] [Google Scholar]
- 21.Sutherland K, Schwab RJ, Maislin G, Lee RW, Benedikstdsottir B, Pack AI, et al. Facial phenotyping by quantitative photography reflects craniofacial morphology measured on magnetic resonance imaging in Icelandic sleep apnea patients. Sleep. 2014;37:959–68. doi: 10.5665/sleep.3670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Albajalan OB, Samsudin AR, Hassan R. Craniofacial morphology of Malay patients with obstructive sleep apnoea. Eur J Orthod. 2011;33:509–14. doi: 10.1093/ejo/cjq108. [DOI] [PubMed] [Google Scholar]
- 23.Lam B, Ip MS, Tench E, Ryan CF. Craniofacial profile in Asian and white subjects with obstructive sleep apnoea. Thorax. 2005;60:504–10. doi: 10.1136/thx.2004.031591. [DOI] [PMC free article] [PubMed] [Google Scholar]