

Abstract
Lymphoscintigraphy is known to be a useful and non-invasive modality for the evaluation of lymphatic abnormality. However, lymphoscintigraphy has limitations in evaluating chyluria because of its lack of anatomical information. Additional single-photon emission computed tomography (SPECT) combined with computed tomography (CT) was considered to be potentially helpful in detecting the abnormal lymphatico-renal communication. A 20-year-old male patient was referred to our hospital for evaluation of recurrent chyluria. During the third recurrence of chyluria, additional SPECT/CT along with lymphoscintigraphy was performed for evaluation. From the combined SPECT/CT images, lymphatic drainage of radiotracers to the kidney was well visualized, helping diagnosis of a patient with chyluria.
Keywords: Chyluria, Radionuclide lymphoscintigraphy, SPECT/CT
Introduction
Chyluria is milky urine composed of albumin, emulsified fat and fibrin in varying proportions that are absorbed by intestinal lacteals. Spontaneous remissions and exacerbations are the common characteristics of chyluria. Chyluria is known to be caused by abnormal lymphatic flow. This may lead to lymphatico-renal shunt, lymphatic ectasia, or varicosities, consequently sending chylous material to the urinary collecting system [1, 2]. It is reported that parasite infection, abdominal operation, lymphangioma of the urinary tract, stenosis of lymphatic vessel, trauma and congenital variation can cause abnormal lymphatic flow, and parasite infection is known to be the most common cause [3, 4]. Chyluria is quite frequently reported in tropical areas such as India, China, Taiwan and Japan; however, it is rarely reported in Korea [5–7].
There are several imaging tools used in diagnosing and localizing chyluria, such as retrograde pyelography, contrast lymphangiography, lymphoscintigraphy, magnetic resonance imaging and computed tomography (CT) [8]. Among these imaging tools, lymphoscintigraphy has advantages in being safe and non-invasive, in localizing, lateralizing and detecting recurrence of chyluria. Kidney or pelvis imaged in the early phase of scan is the most common lymphoscintigraphy pattern for a chyluria patient [9].
The efficacy of single-photon emission computed tomography combined with CT (SPECT/CT) is well known for its use in locoregional evaluation. Many studies have reported the efficacy of SPECT/CT for localizing and identifying the sentinel lymph nodes [10]. Also in many areas such as cardiology, oncology and neurology, the efficacy of SPECT/CT was reported [11]. Considering all these studies, SPECT/CT combined with lymphoscintigraphy should give an advantage in evaluating chyluria.
Here we report a first case of lymphoscintigraphy combined with SPECT/CT in a patient who presented with chyluria.
Case Description
A 20-year-old man who had no history of parasite infection was referred with recurrent chyluria. The first event was reported 10 years ago. In the initial urine analysis, hematuria (four positive), proteinuria (four positive) and leukocyturia (11 positive for white blood cells detected by high-power-field microscopy) were detected, and from a 24-h urine sample, protein (7,600 mg/day) and triglycerides (7,740 mg/day) were detected, indicating chyluria.
For the evaluation, lymphoscintigraphy was acquired 1 h after subcutaneous injection of 37 MBq (1 mCi) 99mTc-labeled antimony sulfide colloid (ASC). Lymphoscintigraphy performed in 2003 showed an asymmetrical uptake in the right kidney and intense bladder retention, which is the most common pattern of chyluria in lymphoscintigraphy (Fig. 1a). After two more episodes of recurrence, laparoscopic lymphatic ligation was performed in 2010. However, a fourth recurrence developed and lymphoscintigraphy was done again, which also showed a similar uptake as in 2003 (Fig. 1b).
Fig. 1.

Anterior-view scan acquired 1 h after subcutaneous injection of 1 mCi 99mTc-ASC. a Lymphoscintigraphy which was done in 2003 shows an asymmetrical uptake in the right kidney and bladder retention. b Lymphoscintigraphy which was done in 2013 also shows an asymmetrical uptake in the right kidney and bladder retention
SPECT/CT images were acquired after 1 h acquisition of lymphoscintigraphy. Maximum intensity projection image shows asymmetrical uptake in the right kidney (Fig. 2a). In the SPECT/CT coronal view, lymphatic flow to the right kidney (Fig. 2barrowhead) and radiotracer accumulation in the renal pelvis (Fig. 2barrow) are visualized. From the axial view, radiotracer accumulation is visualized in the ligation site and from here lymphatic drainage to the right kidney is also well visualized, indicating the lymphatico-renal communication (Fig. 2carrowhead). The visualization of radiotracer excretion through the renal pelvis (Fig. 2darrow) enhanced our confidence in reporting the presence of chyluria. Though chyluria was visualized from the scan, patient discharged without any other procedure done because the symptom subsided after the diet modification.
Fig. 2.
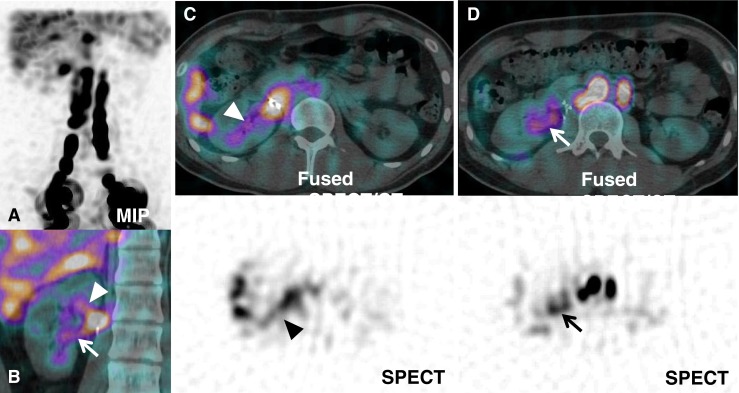
SPECT/CT image was acquired from the upper margin of liver to the iliac crest level, after acquisition of the 1-h lymphoscintigraphy planar image. a MIP image shows asymmetrical uptake in the right kidney. b In the SPECT/CT coronal view, lymphatic flow to the right kidney (arrowhead) and radiotracer accumulation in renal pelvis (arrow) is visualized. c From the axial view, radiotracer accumulation is shown in the ligation site and from here lymphatic drainage to the right kidney is also well visualized, indicating the lymphatico-renal communication (arrowhead). d Radiotracer excretion through the renal pelvis (arrow) is visualized
Discussion
We used 99mTc-ASC as a radiotracer in our study. 99mTc-ASC is an ideal agent for lymphoscintigraphy due to its small particle size (15–40 nm), which permits early migration into the interstitial space and lymphatics and also rapid uptake by lymph nodes [12]. Anterior- and posterior-view regional scans were acquired initially and 1 h after subcutaneous injection of 1 mCi 99mTc-ASC into the first and second interdigital space of both feet. Low-energy high-resolution parallel collimator was used for the image acquisition. After the acquisition of the 1-h lymphoscintigraphy planar image, SPECT/CT images were acquired from the upper margin of liver to the iliac crest level, using a Discovery NM/CT 670 (GE Healthcare, Little Chalfont, UK).
It has been reported that lymphoscintigraphy is a useful noninvasive method for the localization of chyluria and for providing reliable information to perform safe operation [9, 13]. However, dilution of the tracer in the blood stream, tracer uptake in the background organs, and poor camera resolution, makes detection more difficult by lymphoscintigraphy [14]. From a recent study, clinical yield of SPECT/CT evaluating lymphatic transport disorder was described, combining lymphoscintigraphy and SPECT/CT showed more advantage in anatomical correlation of lymphatic transport disorders and understanding the pathology of the disorder [15, 16]. To the best of our knowledge, it is the first study combining SPECT/CT with lymphoscintigraphy for the evaluation of chyluria. Although intraoperative correlation was not done in our case, we assume SPECT/CT lymphoscintigraphy can overcome previously noted limitations of lymphoscintigraphy and by adding more accurate anatomical information, SPECT/CT lymphoscintigraphy will be a powerful diagnostic tool for evaluating chyluria.
Conclusion
We report a rare case of chyluria with lymphatico-renal communication well localized by combining SPECT/CT and lymphoscintigraphy. From our first study of combining SPECT/CT with lymphoscintigraphy, we conclude that SPECT/CT lymphoscintigraphy is a powerful diagnostic tool and diagnostic choice for the evaluation of chyluria.
Acknowledgments
Conflict of Interest
Min Seok Suh, Gi Jeong Cheon, Hyo Jung Seo, Hyeon Hoe Kim, and Dong Soo Lee declare that they have no conflict of interest.
Informed Consent
This study was approved by the Institutional Review Board at Seoul National University Hospital (IRB No. 1409-039-608) and performed in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000. Acquisition of informed consent was exempted by the board because of the retrospective nature of the study. Details that might disclose the identity of the subject were omitted.
References
- 1.Aye UT, Aung ST. Chyluria. Clin Radiol. 1975;26(2):237–42. doi: 10.1016/s0009-9260(75)80051-1. [DOI] [PubMed] [Google Scholar]
- 2.Ngan H, Leong CH. A lymphographic study of chyluria. Br J Radiol. 1977;50(600):863–70. doi: 10.1259/0007-1285-50-600-863. [DOI] [PubMed] [Google Scholar]
- 3.Peng HW, Chou CF, Shiao MS, Lin E, Zheng HJ, Chen CC, et al. Urine lipids in patients with a history of filariasis. Urol Res. 1997;25(3):217–21. doi: 10.1007/BF00941986. [DOI] [PubMed] [Google Scholar]
- 4.Stalens JP, Falk M, Howmann-Giles R, Roy LP. “Milky” urine—a child with chyluria. Eur J Pediatr. 1992;151(1):61–2. doi: 10.1007/BF02073895. [DOI] [PubMed] [Google Scholar]
- 5.Paik YH, Cho YJ, Koo DS, Ree HI, Shim JC. [Studies on the current epidemiological situation of brugian filariasis in endemic areas of Korea] Korean J Parasitol. 1988;26(4):255–62. doi: 10.3347/kjp.1988.26.4.255. [DOI] [PubMed] [Google Scholar]
- 6.Lin TP, Hsu YS, Chen KK, Lin AT, Chang YH, Wu HH, et al. Chyluria—experience of Taipei Veterans General Hospital. J Chin Med Assoc. 2003;66(2):109–12. [PubMed] [Google Scholar]
- 7.Np G. Retroperitoneoscopic management of intractable chyluria. Indian J Urol. 2005;21(1):63–5. doi: 10.4103/0970-1591.19555. [DOI] [Google Scholar]
- 8.Sachit Sharma AKH. Chyluria—an overview. Int J Nephrol Urol. 2009;1(1):14–26. [Google Scholar]
- 9.Sun T, Hu F, Cui S, Chen W, Feng L, Cao R. Localization diagnosis of chyluria by radionuclide lymphoscintigraphy. Zhonghua Yi Xue Za Zhi. 2002;82(4):247–8. [PubMed] [Google Scholar]
- 10.Husarik DB, Steinert HC. Single-photon emission computed tomography/computed tomographyfor sentinel node mapping in breast cancer. Semin Nucl Med. 2007;37(1):29–33. doi: 10.1053/j.semnuclmed.2006.08.001. [DOI] [PubMed] [Google Scholar]
- 11.Bybel B, Brunken RC, DiFilippo FP, Neumann DR, Wu G, Cerqueira MD. SPECT/CT imaging: clinical utility of an emerging technology. Radiographics. 2008;28(4):1097–113. doi: 10.1148/rg.284075203. [DOI] [PubMed] [Google Scholar]
- 12.Wanebo HJ, Harpole D, Teates CD. Radionuclide lymphoscintigraphy with technetium 99m antimony sulfide colloid to identify lymphatic drainage of cutaneous melanoma at ambiguous sites in the head and neck and trunk. Cancer. 1985;55(6):1403–13. doi: 10.1002/1097-0142(19850315)55:6<1403::AID-CNCR2820550640>3.0.CO;2-K. [DOI] [PubMed] [Google Scholar]
- 13.Yuan Z, Luo Q, Chen L, Luo Q, Zhu R. The role of radionuclide lymphoscintigraphy in chyluria. Hell J Nucl Med. 2010;13(3):238–40. [PubMed] [Google Scholar]
- 14.Haddad MC, al Shahed MS, Sharif HS, Miola UJ. Case report: investigation of chyluria. Clin Radiol. 1994;49(2):137–9. doi: 10.1016/S0009-9260(05)83458-0. [DOI] [PubMed] [Google Scholar]
- 15.Weiss M, Landrock S, Wallmichrath J, Baumeister RG, Bartenstein P, Frick A. The clinical yield of SPECT/CT for the assessment of lymphatic transport disorders. First experiences. Nuklearmedizin. 2013;52(6):235–43. doi: 10.3413/Nukmed-0587-13-05. [DOI] [PubMed] [Google Scholar]
- 16.Rahim MK, Kim SE, So H, Kim HJ, Cheon GJ, Lee ES, et al. Recent trends in PET image interpretations using volumetric and texture-based quantification methods in nuclear oncology. Nucl Med Mol Imaging. 2014;48:1–15. doi: 10.1007/s13139-013-0260-2. [DOI] [PMC free article] [PubMed] [Google Scholar]