

Abstract
Objectives
To assess the prevalence and incidence of Early Childhood Caries (ECC) in African-American children.
Methods
A cohort of 96 African-American children approximately one year of age at baseline was recruited in Uniontown, Alabama, by word of mouth and followed for three years. Oral examinations were conducted annually by one of three trained/calibrated dentists using portable equipment, without radiographs. Dental examinations with WHO criteria assessed surface-level dmf.
Results
The prevalence of dmfs was: 1.1% (all d) at approximately age 1 (n=90, six children were excluded for having no erupted teeth); 12.8% (d=10.5% & f=4.7%) at age 2 (n=86); 39.3% (d=21.4%, m=2.4% & f=22.6%) at age 3 (n=84); and 65.8% (d=28.8%, m=5.5 & f=46.6%) at age 4 (n=73). The percentages of incisors, canines, 1st molars and 2nd molars with dmfs were: 0.1%, 0.0%, 0.0% and 0.0%, at age 1; 2.4%, 0.1%, 0.8%, and 0.6% at age 2; 8.2%, 0.8%, 7.6%, and 6.3% at age 3; and 10.2%, 2.2%, 12.6% and 16.7% at age 4, respectively. The three, one-year, person-level incidence rates were 12.8% (from approximately age 1 to age 2), 38.6% (age 2 to age 3), and 56.2% (age 3 to age 4). From baseline, the two-year incidence was 39.3% and three-year incidence was 65.8%, while the two-year caries incidence from age 1 to age 3 was 66.7% (n=72).
Conclusion
The majority of children developed caries during the three-year follow-up, which is much higher than the 32% prevalence of caries among African-American children under age six years in National Health and Nutrition Examination Survey from 1999–2002.
Keywords: Early Childhood Caries, Prevalence and Incidence
Introduction
Dental caries (cavitated or non-cavitated) of primary teeth in children under the age of 72 months, or what is known as Early Childhood Caries (ECC)1, is considered one of the most significant public health problems, not only in the United States of America, but throughout the world1. The U.S. National Health and Nutrition Examination Survey III (NHANES III) data from 1988–1994 showed that about 8.4% of children who were 2 years old and 40.0% who were 5 years old had at least one filled or decayed (cavitated, excluding non-cavitated) tooth2. More recent data from NHANES, 1999–2002, showed that the prevalence of ECC among children aged 2, 3, 4, and 5 years was 10.9%, 20.9%, 34.4%, and 44.3%, respectively3. Although the overall prevalence of dental caries experience among the U.S. population, including some children’s groups, has decreased drastically in the last fifty years, ECC still presents a serious threat to child welfare2. National statistics in the United States show that ECC is most prevalent among children who are from low socioeconomic status families4. Furthermore, the findings of the national surveys demonstrate that ECC is more prevalent among racial and ethnic minority groups, such as African-Americans, Hispanics, and Native-Americans4. For example, NHANES 1999–2002 showed that the overall prevalence of ECC among white children under the age of 6 years was 25.3%, while it was 31.8% among African-American children3.
ECC is a relatively new term, recommended by the National Institute of Dental and Craniofacial Research in 1999 to replace the old names that described its etiology, such as nursing caries and baby bottle tooth decay5. ECC is a chronic, infectious, transmissible, and multifactorial disease that affects 1% to 17% of preschool children in developed countries and up to 70% of preschool children in developing countries6.
The prevalence of ECC varies by country and population and over time. For example, Kolker et al.7 reported the overall prevalence of ECC among African-American children aged 3–5 years in Detroit, Michigan as 75%. Barnes et al.8 stated that the prevalence of nursing caries (presence of carious lesions in 2 or more maxillary incisors) was 22.2%, 20.5%, 23.8%, and 35.1% among White-Americans, African-Americans, Hispanic-Americans, and Native-Americans, respectively. When nursing caries was defined as the presence of carious lesions in 3 or more maxillary incisors, the prevalence was 14.5%, 13.2%, 14.7%, and 23.2%.
Warren et al.9 reported that ECC prevalence among 698 Iowa Fluoride Study children (median age~5 years) was 37% when non-cavitated lesions were included and 27% when non-cavitated lesions were excluded. Warren et al.10 reported the prevalence of ECC among 212 WIC-enrolled children (6–24 months of age) at baseline to be 9% and at 18-month follow-up to be 77%. Litt et al11 examined 184 predominantly African-American children with mean age of 3.9 years at baseline (prevalence=44% and mean dmfs=2.8) and one-year follow-up (prevalence=58% and mean dmfs=4.6).
Karjalainen et al.12 assessed prevalence of cavitated caries experience among three-year-old Finnish children at baseline (8%) and 3-year follow-up (28%). The mean dmft among all children was 0.2 at baseline and 0.9 at the follow-up. Sakuma et al.13 examined Japanese children aged 1.5–3 years, finding 32% with new cavitated caries increment (mean 1.3 surfaces). Grindefjord et al.14 examined Swedish children aged 2.5 and 3.5 years, with an increase of 26% in the prevalence of ECC during the one-year follow-up (d1 lesions included) and mean dmfs increment was 1.9.
As part of a multi-group fluoride varnish clinical trial, Weintraub et al.15 assessed the development of ECC among 126 caries-free children aged 6–44 months at baseline who did not receive fluoride varnish treatment. Including non-cavitated lesions, 29% had caries incidence after 1-year; at the 2-year follow-up, 24% of children who were caries-free at the 1-year follow-up had caries. Mean d2fs (only cavitated) and d12fs (non-cavitated included) increments were 1.6 and 2.8 for the two-year follow-up.
Despite these and other published studies, gaps remain in our knowledge of ECC prevalence and incidence, especially among African-American children. A better understanding of the existing health disparities regarding ECC is critical for the development of effective prevention efforts. This paper reports on the prevalence and the incidence of ECC among a longitudinal cohort of low-income African-American children studied from age one to four years in order to improve our understanding of caries patterns among this high-risk group.
Methods
Data for this project were obtained from an ongoing prospective study conducted at the University of Alabama at Birmingham (UAB). Ninety-six primary caregivers (mostly mothers) of African-American children were recruited by word of mouth in Perry County, Alabama, from July, 2008 to December, 2009. The study children were recruited one year after recruiting another cohort of children who were five years old at baseline from the same community.
Inclusion criteria for the parent study about caries and bacterial acquisition were as follows: infants had to not have had all their first primary molars erupted, be living with their biological mother, have at least one biological sibling, and the parents had to plan to remain in the area for at least 3 years. Also, the children had to be free from all systemic diseases, and only one child per household could participate. The study was approved by the Institutional Review Board at UAB and informed consent was obtained from the children’s caregivers.
Participating children received oral examinations at baseline (approximately age 1), 1 year follow-up(age 2), 2-year follow-up (age 3) and 3-year follow-up (age 4) by three trained and calibrated examiners, using portable equipment with mirror and light source, without radiographs, using the WHO criteria16. Dental explorers were used only occasionally to confirm that carious lesions were cavitated or to confirm that an esthetic resin or sealant was present.
Calibration of dental examinations included duplicate exams on 8–10 children (~10%) annually. Calibration exams began with older children (mean age was approximately five years at baseline of older children cohort) as part of the ongoing longitudinal study until age 3 exams for the infant cohort (our cohort) were conducted. The results of inter-examiner dental examinations by the three examiners with the infant cohort were compared to assess reliability. Additionally, one examiner served as “gold-standard” and re-examined each subject one week after the calibration exams for assessment of intra-examiner reliability.
Professional topical fluoride application was provided every six months, using fluoride varnish. In addition, referrals to dentists were made, especially when cavitated lesions were observed. Furthermore, oral hygiene instructions were provided by dental personnel, including the examiners, dental hygienists, and dental residents in the Department of Pediatric Dentistry. In addition, compensation of $20 and a preventive oral health kit containing a toothbrush, toothpaste, dental flossers, dental floss and dental mirror were provided.
Specific to the secondary analyses for this study, both prevalence and net caries incidence (NCI) were determined at the surface level, including cavitated lesions only. NCI was assessed two ways: a) when unerupted surfaces at the beginning of the incidence period were included and assumed to be sound and b) when unerupted surfaces at the beginning of the incidence period were excluded. Descriptive statistics were calculated for person-level overall prevalence at each dental examination, overall incidence for all study time periods and incidence by tooth type for all time periods. SAS 9.3 (SAS Institute Inc., Cary, NC, USA) was used for data analysis.
Results
In total, 96 children had dental examinations, including six children who had no erupted teeth at baseline (these six children were excluded only from prevalence analysis at baseline). At follow-up examinations at ages approximately 2, 3 and 4 years, 86, 84, and 73 children were examined, respectively. Boys constituted approximately 57% of the total number of children examined. The mean ages of the study children were approximately 1, 2, 3, and 4 years at baseline and the three follow-up examinations (Table 1).
Table 1.
Prevalence of ECC at the person-level at baseline and the three follow-up examinations*
| Dental exam | Number of children | Sex | Age Mean ± SD |
Person-level prevalence (% of children with dmf>0) | dmft Mean ± SD |
dmfs Mean ± SD |
||
|---|---|---|---|---|---|---|---|---|
| Occlusal | Non-occlusal | Total (% of children with d, m, f>0) | ||||||
| Baseline | 90 | M (52%) F (48%) |
1.1 ±0.3 | 0.0 | 1.1 | 1.1 (1.1, 0.0, 0.0) | 0.02±0.21 | 0.02±0.21 |
| 1st follow-up | 86 | M (57%) F (43%) |
2.0 ±0.4 | 5.0 | 12.5 | 12.8 (10.5, 0.0, 4.7) | 0.45±1.50 | 1.19±4.36 |
| 2nd follow-up | 84 | M (58%) F (42%) |
3.1 ±0.4 | 23.1 | 35.9 | 39.3 (21.4, 2.4, 22.6) | 1.62±3.10 | 6.20±13.92 |
| 3rd follow-up | 73 | M (60%) F (40%) |
4.0 ±0.4 | 52.2 | 56.5 | 65.8 (28.8, 5.5, 46.6) | 3.09±3.94 | 11.51±19.12 |
Six children are excluded at baseline in this table, since no teeth were erupted.
Overall, 23 children from the cohort were examined to assess inter- or intra-examiner reliability at ages 3 and 4. At the person level, there was 100% agreement and kappa =1.0 for presence vs. absence of caries experience (any cavitated dmfs). Using total dmfs count at the person level, intra-examiner weighted kappa was 0.91 (n=17), and inter-examiner weighted kappa was 0.93 (n=23).
Dental caries findings at the person-level (Table 1) showed an increase in the prevalence of dental caries with age. Excluding six children who did not have any erupted teeth at age 1, 1.1% had caries experience (dmf>0) at age 1 (all non-occlusal caries). Similarly, the overall prevalence rate at age 2 was 12.8% (occlusal=5.0% and non-occlusal=12.5%), 39.3% at age 3 (occlusal=23.1% and non-occlusal=35.9%), and 65.8% at age 4 (occlusal=52.2% and non-occlusal=56.5%) at the three follow-up examinations, respectively. At age 1, only one child (1.1%) presented with untreated dental caries, with prevalence rates increasing to 10.5%, 21.4% and 28.8% at the three follow-up examinations, respectively. No filled teeth were observed at age 1, and the prevalence of children who had filled teeth increased dramatically to 4.7%, 22.6% and 46.6% at the three follow-up examinations, respectively. There were no children with extracted teeth due to dental caries at age 1 or age 2. However, there were two (2.4%) and four (5.5%) children with teeth missing due to dental caries at approximately age 3 and 4, respectively. Mean dmft increased from 0.02 to 3.09 and mean dmfs increased from 0.02 to 11.51 from approximately age 1 to 4 (Table 1).
At mean age approximately one, all dmfs was ds, while at mean age approximately two, 31.23% of dmfs was ds and 68.77% was fs. At mean age approximately three, 12.29% was ds, 87.66% was fs and 0.05 was ms, while at mean age approximately four, 9.24% was ds, 83.52% was fs and 7.24 was ms (data not shown).
Figure 1 shows tooth-level caries experience by tooth type. The percentage of incisors with caries experience increased from about 0.4% to 11.1% during the three-year follow-up. Almost all incisor caries experience was on maxillary incisors, such that the percentage of upper incisors that had caries experiences increased from about 0.9% to 21.0% during the three-year follow-up (not shown). Also, the percentages of teeth that had caries experience increased from 0.0% to 4.1% in canines, 0.0% to 15.8% in 1st molars and 0.0% to 31.2% in 2nd molars during the three-year follow-up.
Figure 1.
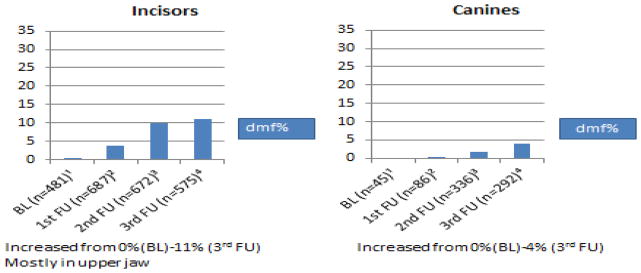
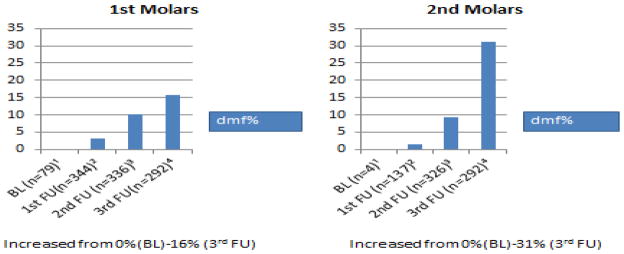
Tooth-level dental caries experience (dmfs%) by tooth type at baseline and the three follow-up examinations (n=number of teeth)
1 Baseline examination (age 1 year)
2 First follow-up (age 2 years)
3 Second follow-up (age 3 years)
4 Third follow-up (age 4 years)
Table 2 shows person-level net caries incidence for each 1-year, 2-year and 3-year period, when unerupted surfaces at the beginning of the time period were included and assumed to be sound (left side). Approximately 66% of the children had at least one new carious surface during the 3-year follow-up (occlusal=50.7% and non-occlusal=57.5%). In addition, Table 2 shows net caries incidence rates at the person-level when only erupted surfaces at the beginning of the time periods were included (right side). Approximately 33% of the children had at least one new dmfs during the 3-year follow-up (occlusal= 21.1% and non-occlusal= 32.8%).
Table 2.
Person-level net caries incidence by study time period
| Incidence period* | Unerupted surfaces included** | Only erupted surfaces included | ||||||
|---|---|---|---|---|---|---|---|---|
| Number of children*** | Incidence (% with Δ dmfs>0) (range) | Number of children | Incidence (% with Δ dmfs>0) (range) | |||||
| Occlusal | Non-occlusal | Total**** | Occlusal | Non-occlusal | Total***** | |||
| Age 1 to age 2 | 86 | 4.7 (0–6) | 11.6 (0–24) | 12.8 (0–30) | 80 | 10.0 (0–4) | 11.3 (0–20) | 12.5 (0–20) |
| Age 1 to age 3 | 84 | 22.6 (0–10) | 38.1 (0–54) | 39.3 (0–64) | 78 | 20.0 (0–4) | 23.1 (0–34) | 23.1 (0–38) |
| Age 1 to age 4 | 73 | 50.7 (0–10) | 57.5 (0–62) | 65.8 (0–72) | 67 | 21.1 (0–4) | 32.9 (0–34) | 33.1 (0–38) |
| Age 2 to age 3 | 83 | 22.9 (0–10) | 37.4 (0–43) | 38.6 (0–53) | 83 | 21.7 (0–10) | 34.9 (0–43) | 38.6 (0–53) |
| Age 2 to age 4 | 72 | 51.4 (0–10) | 58.33 (0–48) | 66.7 (0–57) | 72 | 38.9 (0–6) | 51.4 (0–34) | 59.7 (0–52) |
| Age 3 to age 4 | 73 | 40.1 (0–9) | 46.6 (0–39) | 56.2 (0–47) | 73 | 41.1 (0–8) | 45.2 (0–36) | 54.8 (0–47) |
Approximated ages.
Unerupted surfaces at the beginning of the incidence period were assumed to be sound.
Seventy-two children had all four dental examinations.
When surfaces unerupted at baseline were included, about 66% of the children had caries incidence (maximum 72 surfaces) during the three-year follow-up.
When only surfaces erupted at baseline were included, about 33% of the children had caries incidence (maximum 38 surfaces) during the three-year follow-up.
The left part of Table 3 shows the incidence at the person-level by tooth type for all study time periods, when unerupted surfaces were included. During the three-year follow-up, 35.6%, 9.6%, 27.4% and 49.3% of the children developed new caries incidence on incisors, canines, 1st molars and 2nd molars, respectively. The right half of Table 3 shows the incidence at the person-level by tooth type for all study time periods, when only previously erupted surfaces were included. During the three-year follow-up, approximately 29.9%, 16.7%, 26.3% of the children developed new caries incidence on incisors, canines and 1st molars, respectively. Since all children had all of their 2nd molars un-erupted at baseline, the three-year ECC incidence for 2nd molars could not be determined.
Table 3.
Person-level net caries incidence by tooth type and study time period
| Incidence period | Person-level incidence-unerupted surfaces included*-percentage (number of children) | Person-level incidence- only erupted surfaces included**-percentage (number of children) | ||||||
|---|---|---|---|---|---|---|---|---|
| Incisors | Canines | 1st M | 2nd M | Incisors | Canines | 1st M | 2nd M | |
| Age 1 to age 2 | 11.6% (80) | 1.2% (80) | 5.8% (80) | 1.2% (80) | 11.3% (80) | 8.3% (12) | 10.0% (20) | NA (0) |
| Age 1 to age 3 | 28.6% (78) | 3.6% (78) | 19.1% (78) | 14.3% (78) | 23.9% (78) | 8.3% (12) | 20.0% (20) | NA (0) |
| Age 1 to age 4 | 35.6% (67) | 9.6% (67) | 27.4% (67) | 49.3% (67) | 29.9% (67) | 16.7% (12) | 26.3% (19) | NA (0) |
| Age 2 to age 3 | 22.9% (83) | 3.6% (83) | 19.3% (83) | 14.5% (83) | 22.9% (83) | 3.8% (79) | 19.3% (83) | 23.8% (42) |
| Age 2 to age 4 | 33.3% (72) | 9.7% (72) | 27.8% (72) | 50.0% (72) | 33.3% (72) | 10.0% (70) | 27.8% (72) | 52.6% (38) |
| Age 3 to age 4 | 23.3% (73) | 6.9% (73) | 16.4% (73) | 43.8% (73) | 21.9% (73) | 6.9% (73) | 16.4% (73) | 42.5% (73) |
When surfaces unerupted at baseline were included (assumed to be sound), there were higher percentages of teeth with new caries during the three-year follow-up on their 2nd molars (49%), followed by incisors (36%), 1st molars (27%) and canines (10%).
When only surfaces erupted at baseline were included, there were higher percentages of teeth with new caries during the three-year follow-up on their incisors (30%), followed by 1st molars (26%) and canines (17%).
Discussion
In this report of African-American children living in the Southeastern Black Belt region of the U.S., the percentage of children who experienced dental caries increased from 1.1% at approximately age 1 to 12.8% at age 2, 39.3% at age 3 and 65.8% at age 4, even though these children received fluoride varnish treatments at 6-month intervals. The increases in prevalence and incidence rates over time are most likely due to increased duration of exposure to risk factors and increased number of teeth at risk. Results for 72 children, who completed all four dental examinations and including unerupted surfaces at baseline, showed that about 66% of the children developed at least one carious or filled surface (maximum 72 carious or filled surfaces) during the three-year follow-up. However, when only erupted surfaces at baseline were included, about 33% of the children developed at least one carious or filled surface (maximum 38 carious or filled surfaces) during the three-year follow-up.
The findings of this study showed that the prevalence and ECC increments were greater than those reported in most other studies and surveys. Our results are generally consistent with and somewhat higher than NHANES averaged across ages 0 to 5.993. Kolker et al.7 reported even higher prevalence rates of ECC among African-American children in Detroit, Michigan- with 64.2% and 74.2% among three and four year old children, respectively, compared to 39.3% and 65.8% in our study, respectively. However, Kolker et al.7 used the International Caries Detection and Assessment System (ICDAS) criteria17, iwith non-cavitated lesions included in their analyses. Warren et al.9 reported that the prevalence of ECC among predominately Caucasian children with a mean age of 4.6 was 27.0% when only cavitated lesions were included in the analyses, compared to 65.8% in our study.
In our study, the percentage of children that developed smooth caries incidence (57.5%) was slightly higher than the percentage that developed occlusal caries incidence (50.7%) for all study time periods. O’Sullivan et al.18 examined Connecticut Head Start children with a mean age of 3.8 years at baseline who were followed for two years. At baseline, 60.6% of the children were caries-free (group 1), 28.9% had pit and fissure caries without smooth surface caries (group 2), and 10.6% had maxillary anterior caries with or without occlusal caries (group 3). The mean two-year increases in dmfs were 1.4 in group 1, 2.9 in group 2 and 5.1 in group 3.
Tooth-level analyses of incidence showed that the incidence of ECC on 2nd molars was higher (49%, with unerupted surfaces included during the three-year follow-up) than that of 1st molars (27%, with unerupted surfaces included). This was found despite the fact that 1st molars erupted earlier and were exposed to the oral environment, bacteria and other risk factors for longer periods of time. Biologically, this might be due to the higher susceptibility of newly-erupted teeth to dental caries because of the colonization by microorganisms. Difficulty in accessing 2nd molars during tooth brushing and/or difficulty in properly applying fluoride varnish to them due to difficulty in establishing a dry environment optimal for application of fluoride varnish compared to 1st molars, might also explain this finding. In contrast, Chankanka et al.19 examined Iowa Fluoride Study children at age 5 years. Mean dmfs were 0.09, 0.06, 0.61 and 0.37 among incisors, canines, 1st molars and 2nd molars, respectively. Thus, mean dmfs was the highest among 1st molars, followed by 2nd molars, incisors and canines. However, in our study at age 4, mean dmfs was the highest among 2nd molars (1.25), followed by incisors (0.88), 1st molars (0.36) and canines (0.16).
Limitations of our study were the relatively small sample size and the nature of our sample (convenience sample), reduces our ability to generalize the findings. Furthermore, our study probably underestimated the true prevalence and incidence of ECC, since caries was reported at the cavitated level only (non-cavitated lesions were not reported) and radiographs, which provide an important diagnostic method for interproximal caries, were not used. Also, since children were referred to local dentists for dental care, it is possible that children were treated based on different criteria for caries and need for restoration than the criteria followed by the UAB team. This and other factors related to criteria for full coverage restorations could inflate the “f” portion of the dmfs caries prevalence data20.
Despite these limitations, our study provides additional evidence to the very limited body of literature reporting on the prevalence and incidence of ECC in very young children. While previous studies have reported on ECC in predominantly Caucasian, Hispanic or urban African-American children, our study is the first to report on ECC among rural African-American children. The findings are generally consistent with these earlier studies and suggest that rural African-American children have rates of ECC similar to other minority or disadvantaged groups. The consistency of these findings serves to confirm that high rates of ECC are not unique to certain racial/ethnic groups, and are almost certainly not due primarily to any inherent racial or ethnic factors, but rather are largely the result of poverty, wherever it may exist. Thus, the findings of this study, combined with those of previous ones, suggest that efforts to address and prevent ECC need to focus on developing a better understanding of poverty and how it affects oral health behaviors, and ultimately, oral health. The study is also valuable in that it provides information on dmfs increments at the tooth-type level and surface level among very young, high caries risk children. This information could be valuable in better understanding the patterns of ECC within the oral cavity and how the disease progresses.
Acknowledgments
The authors would like to thank all the coordinators who helped selflessly in Uniontown, Alabama. Also, the authors wish to thank the National Institutes of Health for supporting the project through the grant R01-DE016684.
Contributor Information
Tariq Ghazal, Email: tariq-ghazal@uiowa.edu, College of Dentistry, University of Iowa, Preventive and Community Dentistry, 801 Newton Rd #451, Iowa City, Iowa, United States.
Steven M. Levy, Email: steven-levy@uiowa.edu, University of Iowa, College of Dentistry, 328 Dental Science Building North, Iowa City, Iowa, United States.
Noel K. Childers, Email: nkc@uab.edu, School of Dentistry at University of Alabama, Pediatric Dentistry, 1530 3rd Avenue South, SDB 304, SDB, Birmingham, Alabama, United States.
Barbara Broffitt, Email: barbara-broffitt@uiowa.edu, University of Iowa, Preventive & Community Dentistry, N329 DSB, Iowa City, Iowa, United States.
Gary Cutter, Email: cutterg@prodigy.net, College of Public Health, University of Alabama at Birmingham, Department of Biostatistics, Birmingham, Alabama, United States.
Howard W. Wiener, Email: hwiener@uab.edu, College of Public Health, University of Alabama at Birmingham, Department of Epidemiology, Birmingham, Alabama, United States.
Mirjam Kempf, Email: mkempf@uab.edu, School of Nursing, Health Behavior, Birmingham, Alabama, United States.
John Warren, Email: john-warren@uiowa.edu, University of Iowa, Preventive & Community Dentistry, N-337 Dental Science Bldg., Iowa City, Iowa, United States.
Joseph Cavanaugh, Email: joe-cavanaugh@uiowa.edu, College of Public Health, University of Iowa, Biostatistics, Iowa City, Iowa, United States.
Rerences
- 1.American Academy of Pediatric Dentistry. Policy Early childhood Caries (ECC): Classifications, consequences, and Preventive Strategies. Pediatr Dent. 2008;30(suppl):83. [PubMed] [Google Scholar]
- 2.Beltran-Aguilar ED, Barker LK, Canto MT, Dye BA, Gooch BF, Griffin SO, et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis – United States, 1988–1994 and 1999–2002. MMWR Surveill Summ. 2005;54:1–43. [PubMed] [Google Scholar]
- 3.Kaste LM, Drury TF, Horowitz AM, Beltran E. An evaluation of NHANES III estimate of Early Childhood Caries. J Public Health Dent. 1999;59(3):198–200. doi: 10.1111/j.1752-7325.1999.tb03269.x. [DOI] [PubMed] [Google Scholar]
- 4.Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton-Evans G, et al. Trends in oral health status—United States, 1988–1994 and 1999–2004. [cited 2010 Jun 1] Vital Health Stat. 2007;11(248) Also available from: URL: http://www.cdc.gov/nchs/data/series/sr_11/sr11_248.pdf. [PubMed] [Google Scholar]
- 5.Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, Selwitz RH. Diagnosing and reporting early childhood caries for research purposes: A report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J Public Health Dent. 1999;59:192–7. doi: 10.1111/j.1752-7325.1999.tb03268.x. [DOI] [PubMed] [Google Scholar]
- 6.Milnes AR. Description and epidemiology of nursing caries. J Public Health Dent. 1996;56:38–50. doi: 10.1111/j.1752-7325.1996.tb02394.x. [DOI] [PubMed] [Google Scholar]
- 7.Kolker JL, Yuan Y, Burt BA, Sandretto AM, Sohn W, Lang SW, Ismail AI. Dental caries and dietary patterns in low-income African-American children. Paediatr Dent. 2007;29:6. [PubMed] [Google Scholar]
- 8.Barnes GP, Parker WA, Lyon TC, Drum MA, Coleman GC. Ethnicity, location, age and fluoridation factors in baby bottle tooth decay and caries prevalence of Head Start children. Public Health Rep. 1992;107:167–73. [PMC free article] [PubMed] [Google Scholar]
- 9.Warren JJ, Levy SM, Kanellis MJ. Dental caries in the primary dentition: Assessing prevalence of cavitated and noncavitated lesions. J Public Health Dent. 2002;62(2):109–114. doi: 10.1111/j.1752-7325.2002.tb03430.x. [DOI] [PubMed] [Google Scholar]
- 10.Warren JJ, Weber-Gasparoni K, Marshall TA, Drake DR, Dehkordi-Vakil F, Dawson DV, Tharp KM. A longitudinal study of dental caries risk among very young low SES children. Community Dent Oral Epidemiol. 2009;37:116–122. doi: 10.1111/j.1600-0528.2008.00447.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Litt MD, Reisine S, Tinanoff N. Multidimensional causal model of dental caries development. Public Health Rep. 1995;110:607–607. [PMC free article] [PubMed] [Google Scholar]
- 12.Karjalainen S, Soderling E, Sewon L, Lapinleimu H, Simell O. A prospective study on sucrose consumption, visible plaque and caries in children from 3 to 6 years of age. Community Dent Oral Epidemol. 2001;29:136–42. doi: 10.1034/j.1600-0528.2001.290208.x. [DOI] [PubMed] [Google Scholar]
- 13.Sakuma S, Nakamura M, Miyazaki H. Predictors of dental caries development in 1.5-year-old high-risk children in the Japanese public health service. J Public Health Dent. 2007;67:14–19. doi: 10.1111/j.1752-7325.2007.00003.x. [DOI] [PubMed] [Google Scholar]
- 14.Grindefjord M, Dahllöf M, Modéer T. Caries development in children from 2.5 to 3.5 years of age: a longitudinal study. Caries Res. 1995;29:449–454. doi: 10.1159/000262113. [DOI] [PubMed] [Google Scholar]
- 15.Weintraub JA, Ramos-Gomez F, Jue B. Fluoride varnish efficacy in preventing early childhood caries. J Dent Res. 2006;85(2):172–176. doi: 10.1177/154405910608500211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Health Organization. Oral health surveys: basic methods. 3. Geneva: WHO; 1987. [Google Scholar]
- 17.Pitts N. ICDAS: An international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health. 2004;21:193–8. [PubMed] [Google Scholar]
- 18.O’Sullivan DM, Tinanoff N. The association of early dental caries patterns with caries incidence in preschool children. J Public Health Dent. 1996;56:81–83. doi: 10.1111/j.1752-7325.1996.tb02401.x. [DOI] [PubMed] [Google Scholar]
- 19.Chankanka O, Cavanaugh JE, Levy SM, Marshal T, Warren JJ, Broffitt B, Kolker JL. Longitudinal associations between children’s dental caries and risk factors. J Public Health Dent. 2011;71:289–300. doi: 10.1111/j.1752-7325.2011.00271.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Burt BA. How useful are cross-sectional data from surveys of dental caries? Community Dent Oral Epidemiol. 1997;25:36–41. doi: 10.1111/j.1600-0528.1997.tb00897.x. [DOI] [PubMed] [Google Scholar]