

Abstract
Background:
Cigarette smoking is one of the preventable causes of diseases and deaths. The most important preventive measure is technique to resist against peer pressure. Any educational program should design with an emphasis upon theories of behavioral change and based on effective educational program. To investigate the interventions through educational program in prevention of cigarette smoking, this paper has used the Extended Parallel Process Model (EPPM).
Materials and Methods:
This study is a quasi-experimental study. Two middle schools were randomly selected from male students in Shiraz. Therefore, we randomly selected 120 students for the experimental group and 120 students for the control group. After diagnostic evaluation, educational interventions on the consequences of smoking and preventive skills were applied.
Results:
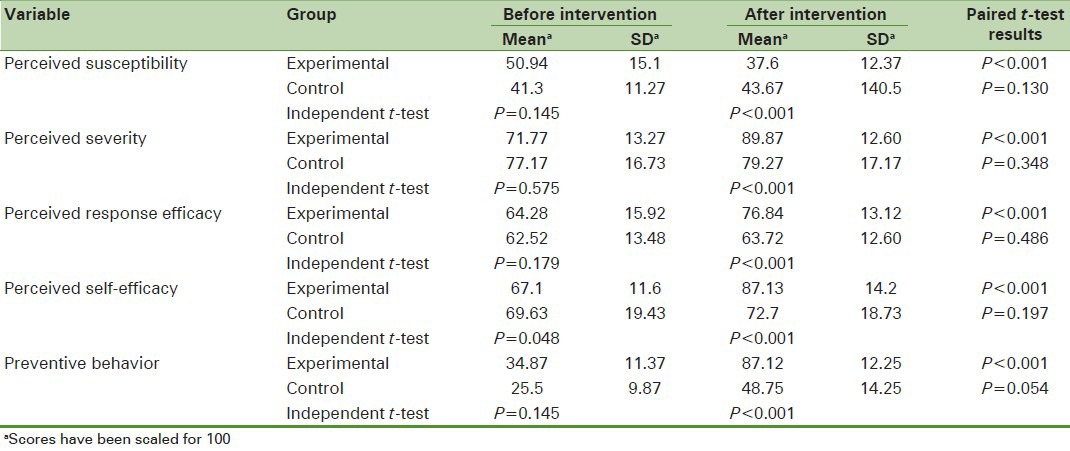
Our results indicated that there was a significant difference between students in the control and experimental groups in the means of perceived susceptibility (P < 0.000, t = 6.84), perceived severity (P < 0.000, t = −11.46), perceived response efficacy (P < 0.000, t = −7.07), perceived self-efficacy (P < 0.000, t = −11.64), and preventive behavior (P < 0.000, t = −24.36).
Conclusions:
EPPM along with educating skills necessary to resist against peer pressure had significant level of efficiency in improving preventive behavior of cigarette smoking among adolescents. However, this study recommends further studies on ways of increasing perceived susceptibility in cigarette smoking among adolescents.
Keywords: Cigarette smoking, extended parallel process model, health education, students
INTRODUCTION
Cigarette smoking is one of the preventable causes of deaths and diseases, responsible for a tenth of adult mortality rate around the world.[1] It is predicted that by 2030, smoking will be the cause of 70% of annual mortality rate globally in developing countries.[2,3] The prevalence of smoking among male teens of 13–15 years of age has been 17% in eastern Mediterranean in the period of 2005–2010.[4] According to WHO data, the latest statistics on Iran indicate that the daily consumption of tobacco has been 20.4% among males.[5] Scientific findings show that smoking is harmful not only for smokers, but also for individuals around smokers indirectly.[6,7,8] It is believed that the transition period from adolescence to early adulthood brings significant changes in behavior and psychology of the individuals. Taking decisions on a healthy lifestyle is the basis for personality building of the individual. Indeed, the adult health is affected by healthy behavior of the childhood and adolescence.[9] Early initiation of cigarette smoking is very worrying. Given, the many studies have shown that it is a strong predicting factor of smoking in adulthood.[10,11] Initiation of cigarette smoking in younger ages will be accompanied with difficulties to quit smoking in adult life.[12] Several investigations indicate that the prevalence of cigarette smoking in both boys and girls is increasing.
In other words, the age of initiation of cigarette smoking is decreasing.[13,14,15,16] Mohtasham Amiri[17] and WHO report[4] showed that the average age to initiate cigarette smoking was at 13 years. Other studies indicated that the prevalence of cigarette smoking among adolescents was related to a smoker among family members, friends, the lack of knowledge about consequences of cigarette smoking, socioeconomic status of the parents, and school conditions.[18,19,20,21] Therefore, researchers in industrial countries have emphasized upon prevention of smoking in young people, and programs have been designed and implemented to achieve this objective. These programs aimed to improve students’ knowledge, change in their attitudes, and behavior with a level of success.[22,23,24] Thus, any program aimed for training resistance skills against drug abuse, and cigarette smoking should be implemented with an emphasis upon theories of behavioral change and based on effective educational programs. A fear-based theory is the effective approach for preventing unhealthy behaviors. Extended Parallel Process Model (EPPM) provides a major theoretical framework of change in behavior.[25,26] Because adolescents can be predisposed to engage in high-risk behaviors. Therefore, this is an attempt to apply the EPPM for designing effective programs to reduce high-risk behaviors such as cigarette smoking [Figure 1].
Figure 1.
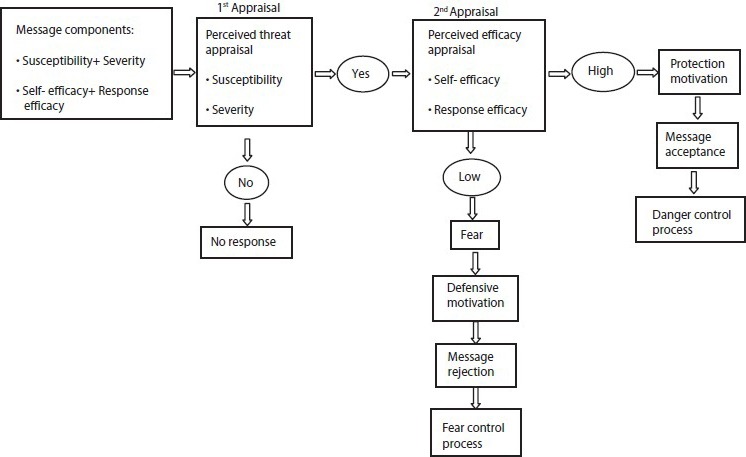
The extended parallel process model. adapted from witte (1994)[53]
According to the EPPM, if people believe that they are highly exposed for suffering diseases or health risks, they will be more motivated to confront with risks and diseases, and then the assessment begins for the efficacy of recommended strategies, and the outcome of efficacy of recommended strategies is assessed to counter risks. In fact, fear of threat will cause people to counter with health risks by adopting strategies. Consequently, it is possible the change of attitude, intention, and behavior will increase.[25,26] Wong and Capella[27] believed that motivation of health-risk message regarding cigarette smoking according to EPPM has been effective in nonsmoking programs among individuals. If so, the threat must be very strong to cause fear in individuals. In such a moment, special measures (response efficacy of the message) to overcome the threats come to minds of the individuals. A person who has received a message should believe that he or she could act according to recommended process (high self-efficacy).[27] Thus, this study was designed to determine the effect of educational programs based on parallel process model for prevention of cigarette smoking among middle school students in Shiraz city. It is expected that this study provides the appropriate solution to prevent cigarette smoking among adolescents and enhances their health promotion and community by providing useful results.
MATERIALS AND METHODS
This study was interventional quasi-experimental research that was carried out among male students of middle schools in Shiraz in the period 2009–2010. Through simple random sampling, two schools were selected. Finally, from each school, four classes were randomly selected. According to the sample size formula, we randomly selected 120 students for the experimental group and 120 students for the control group. Approximately, 10% of participants were excluded from the study because of the absence of educational sessions as well as unwillingness to continue in the study. All participants were enrolled voluntarily and anonymously into the study. Then, a questionnaire according to EPPM was modified based on Witte's EPPM scale[26,28] for cigarette smoking and its consequences. The questionnaire were designed with 19 items about demographic and background information such as age, having father who had experiences with smoking (yes/no), having friends who smoked (yes/no), insistence to smoke by friends (yes/no), age of the first-time smoking (10 years; 11 years; 12 years; and 13 years), most important reason for smoking (urgent need, to alleviate pain, having smoker friends, adventurism, and feeling happy), and also EPPM variables were designed to measure perceived susceptibility with six items (e.g. “I may smoke like some of the young people in the future”), perceived severity with six items (e.g. “I believe that smoking causes lung cancer”), perceived response efficacy with five items (e.g. “I protect myself against smoking with using the resistance skills”), and perceived self-efficacy with six items (e.g. “I believe that I cannot resist pressure from my friends”). Preventive behavior with six items include: Have you smoked in the past 2 months? (yes/no); in the last 2 months, when you exposed to smoke, have you attempted to get away from it?(yes/no); in the last 2 months, have you ever tried that your family acquired more information about consequences of cigarette smoking, and ways to prevent it? (yes/no); in the last 2 months, do you have to talk about the consequences of cigarette smoking, and ways to prevent it for smoker? (yes/no), if yes, whom did you talk? (family, peers and friends, others); when your friends and peers offer you a cigarette, what is your answer? (I smoke cigarette, I’m not saying against them offer and immediately leave there, and I stay with them, but I’m not smoking). To increase self-efficacy for ability to “say no” and ability to “resist peer pressure” to cigarette smoking was used the role-playing method. Each item of constructs of EPPM was measured by Likert scale having five descriptors of strongly agrees to strongly disagree. To measure the reliability and validity of the questionnaire, a pilot study was conducted on 35 students. Estimated reliability coefficients for each EPPM variables were as follows: Perceived susceptibility (α = 0.75), perceived severity (α = 0.65), perceived response efficacy (α = 0.70), and perceived self-efficacy in applying skills of resistance against smoking (α = 0.77), indicating internal consistency. To measure the validity, the experts of panel were established. After pretest and determination of a critical point as to which stages of threat control process (risk control or fear control), the required content was developed for the target group. An educational program was implemented as the following: In a school chosen as the experimental group, three types of posters with contents of cigarette, its risks on physical health, and skills to resist (“say no” to cigarette smoking) were placed. Then, five lectures and discussion sessions were held within displaying a video clip that each lasted 40 min. All sessions were held in the conference halls of the respective schools. The educational sessions’ topics are as follows: First session: Having a discussion about definition and physiology of addiction, second session: To debate about knowledge of smoking, and discussion about influencing factors on initiation of smoking, third session: Identifying and understanding about the complications and consequences of cigarette smoking, and benefits of quitting smoking, fourth session: Ability to detection of high-risk situations and problem-solving skills. Fifth session: Ability to “say no” and ability to “resist peer pressure” to cigarette smoking. The video clip included physical, psychological, and social effects and consequences of cigarette smoking. In the end of each session, a question was asked as scenario and home assignment aimed at active learning and better preparation by students in the next session. If any student who did not do homework, questions were asked them. A handbook entitled guide to prevention of smoking in adolescents was developed and distributed among the participants. Furthermore, in the research, to enhance the effect of active learning and educational intervention, the peer education method was applied through choosing the most popular student and teacher in each class by direct voting by students. Due to time constraints and being close to the program of examinations in the target group, 2 months after the intervention, the questionnaire was completed by both the experimental and control groups. The data were analyzed with SPSS 16 using χ2, McNamara, independent t-test, and paired t-test with 0.05 significance level.
RESULTS
As shown in Table 1, more than one-third of students experienced an initial cigarette smoking at 13 years old (43.8%). Further, less than one-third of participants in the experimental group and more than one-quarter in the control group reported that their father smoked (30.8% and 26.7% respectively). The results showed that less than one-fifth of students stated that their friends experienced cigarette smoking (9.2%). In addition, less than one-fifth of participants reported that their friends insisted that they smoke (5%). Less than one-third of students reported curiosity as their most important reason for cigarette smoking (31.2%).
Table 1.
Frequency and relative frequency distribution of demographic and background variables of participants in the control and experimental groups
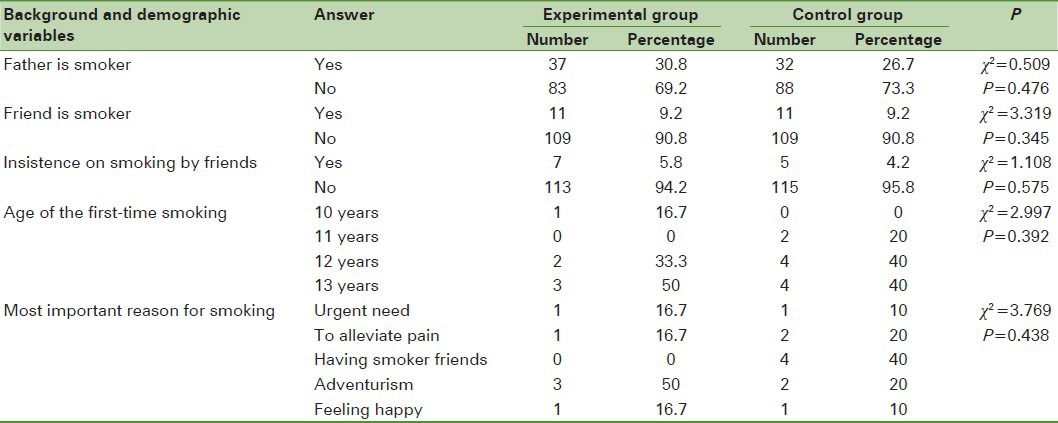
Table 2 shows that there was no significant difference in background and demographic variables between the experimental and control groups. To compare the means of scores for EPPM constructs and preventive behavior components, independent and paired t-tests were carried out on the experimental and control groups before and after the educational intervention. Table 2 displays that before the educational program, there was no significant difference between the experimental and control groups in scores of EPPM constructs and preventive behavior, except for the scores of perceived self-efficacy (P = 0.048). The result indicated that there was a significant difference between the mean of scores of perceived susceptibility, perceived severity, perceived response efficacy, perceived self-efficacy, and preventive behavior on cigarette smoking before and after educational intervention in the experimental group (P < 0.001); whereas, there was no significant difference between the same variables before and after the educational intervention in the control group (P > 0.05).
Table 2.
Comparison of mean of scores for extended parallel process model constructs and preventive behavior, before and after intervention in the experimental and control groups
DISCUSSION
The results of this study showed that educational interventions based on the EPPM can increase preventive behaviors of cigarette smoking among students. The extended nature of problems arising from smoking and drug consumption and failure of approaches taken to prevent and to treat are two strong motivating factors to develop and apply new preventive approaches.[29]
In this study, after the educational intervention, the mean score of perceived susceptibility declined significantly in the experimental group. This result is consistent with similar findings of other studies, so that Witte[25,30] maintained that if people do not feel at-risk for a threat (low perceived susceptibility), or do not feel the threat to be significant (low perceived severity), they simply will ignore information about the threat. Hong[31] concluded that when individuals knew more information about ways of coping with a health threat, their perceived susceptibility toward the threat reduced. Pechmann et al.[32] indicated that message themes about cigarette smoking increased health-risk severity perceptions but were undermined by low perceived vulnerability. Although students believed the serious complications and consequences of smoking, on the other hand, perceived severity scores were high; but these students did not perceive that they were at high risk for cigarette smoking. Some studies have reported that people tend to believe they are less likely to experience negative events and more likely to experience positive events than other people. This phenomenon has been named “optimistic bias”.[33,34] Adolescents may engage in more risk-related behaviors, such as the consumption of alcohol and drugs, cigarette smoking, or unprotected sexual intercourse for two major reasons. First, adolescents may have feelings of invulnerability to harm, thus promoting risky behavior. Second, adolescents sometimes do not perceive their actions as unsafe and engage in risky behaviors out of ignorance of the consequences.[33,34,35,36] Both a sense of invulnerability and low perceived susceptibility to danger are instances of optimistic bias. In both instances, individuals perceive that they are less likely than others to be afflicted with poor health outcomes, such as cigarette smoking. Perhaps because of low perceived susceptibility, high percentage of participants experienced an initial cigarette smoking at 13 years old. This may endanger their health in the future. Ziaadini et al.[37] and Mohtasham Amiri[17] revealed that the average age of initial cigarette smoking was 13 years. Lack of perceived susceptibility to smoking among these participants may be due to a lack of knowledge about the role and the effect of peer pressure. This result suggests that health educators may need to emphasize perceived susceptibility in cigarette smoking prevention programs.
The increased perceived severity in the experimental group demonstrated the effectiveness of messages with the content of fear appeals. Sharifi-rad et al.[38] revealed that education programs have a significant effect on increasing the perceived severity after interventions. In addition, Rahnavard et al.[39] indicated the effect of health education on increasing the perceived severity score after educational intervention. For the first time, Rogers[40,41] provided a definition of perceived threat and efficiency as important variables in his studies. In EPPM, the perceived threat consisted of two components; the perceived susceptibility and perceived severity from the threat.[25,42] Sharifi-rad et al.[38] also revealed that the mean score of the perceived threat has significantly increased after educational intervention. Further, Cho and Witte[43] and Hong[31] concluded that perceived threat on health behavior should be somewhat high so that individuals feel at risk and perceive the seriousness of the threat.
The increased perceived response efficacy score in the experimental group in our study probably reflects the effect of messages and educational programs according to resistance skills or rejecting persistence of friends and peer groups, and problem-solving skills. Peer pressure and invitation for cigarette smoking and other drugs by friends have been one of the most risk factors for the experience of smoking. Cigarette smoking among friends and members of the family, especially the parents of smoking, can be a major factor in the tendency toward smoking in adolescents. Lorenzo-Blanco et al.,[44] Schuck et al.,[45] and Rafiee et al.[46] indicated that having smoker peers or parents had been the most important motivating factors to smoke among adolescents. Fujimoto et al.[47] and Zadeh et al.[48] showed that friends were an important factor in the initiation of smoking. Offering and insistence on smoking by friends may be stimulus factor to start cigarette smoking in adolescents. Leatherdale et al.[49] revealed a positive correlation between smoking and having smoker friends. Further Ziaadini et al.[37] showed the most common situations where male students smoked, when they were accompanied by their friends. Individuals are influenced by peer pressure on early teens; therefore, educational programs for resistance skills, especially “say no” to insistence on smoking, by friends played an important role in prevention of cigarette smoking and drug abuse. Several studies have emphasized on confronting peer pressures in prevention of drug abuse and smoking.[50,51] Several studies indicated that according to EPPM, individuals evaluated the efficacy of the recommended response so that they determine the easy, feasible, and effective recommended response. When individuals believe that messages are useful and also they are able to actually use them, the perceived response efficacy would increase consequently.[25,30] The findings of Moscato et al.[52] indicated that perceived response efficacy and perceived threat were significantly correlated to drinking alcohol. Other studies[53,54] reported that perceived response efficacy and their effect on change in behavior increased after educational interventions.
There was a significant difference for perceived self-efficacy with using resistance skills against cigarette smoking between the experimental and control group before educational intervention. It seems that this difference would be accounted for by the very nature of youth in protecting or adventuresome behaviors. However, after implementing interventions, the self-efficacy score of the experimental group displayed a significant increase compared to that of the control group. In this respect, the findings of Allahverdi Pour et al.,[35] Valente et al.,[55] and Ulgen et al.[56] reported that the mean scores of perceived self-efficacy were significantly high after the interventional programs. These findings indicated that training life skills (resistance against peer pressures and problem solving skills) with emphasis upon perceived self-efficacy would provide a giant leap forward in prevention and control of smoking among adolescents and adults.
The improvement of preventive behavior of smoking in the experimental group after education was indicative of the effect of EPPM components in prevention of smoking. Several studies[38,39,57] showed that the preventive behavior score increased significantly after interventional programs. On the basis of these results, it is necessary to emphasize perceived susceptibility, perceived response efficacy, and self-efficacy in smoking resistance programs. Thus, EPPM could help improve the efficiency of fear appeal messages for prevention of cigarette smoking. There were a few limitations in this study. First, adolescents who have not entered school for any reason were not considered for this study. Second, the sample size was small. Third, a longer follow-up was not possible. Furthermore, incorrect responses were likely because of self-reporting of students.
CONCLUSION
Educational programs based on EPPM increased the perceived threat and perceived efficacy for the preventive behavior of smoking. Many teens and young adults are less vulnerable to threats and health risks. Thus, increasing the perceived threat causes an increase in susceptibility and severity of threat in adolescents. On the other hand, educating skills to resist peer pressure based on the perceived response efficacy of messages and strategies can be effective in the prevention of smoking. Therefore, planning for school-based interventions should be developed with emphasis on the EPPM variables, and programs for prevention of smoking should be started in younger adolescents.
ACKNOWLEDGMENTS
The authors would like to thank the Vice Chancellor of Research and Technology of Hamadan University of Medical Sciences for financial support of this study.
Footnotes
Source of Support: Research Deputy, Hamadan University of Medical Sciences
Conflict of Interest: None declared
REFERENCES
- 1.Christophi CA, Savvides EC, Warren CW, Demokritou P, Connolly GN. Main determinants of cigarette smoking in youth based on the Cyprus GYTS. Prev Med. 2009;48:232–6. doi: 10.1016/j.ypmed.2009.01.003. [DOI] [PubMed] [Google Scholar]
- 2.Bawazeer AA, Hattab A, Morales E. First cigarette smoking experience among secondary school students in Aden, Republic of Yemen. East Mediterr Health J. 1999;5:440–9. [PubMed] [Google Scholar]
- 3.Gu D, Wu X, Reynolds K, Duan X, Xin X, Reynolds RF. Cigarette Smoking and Exposure to Environmental Tobacco Smoke in China: The International Collaborative Study of Cardiovascular Disease in Asia. Am J Public Health. 2004;94:1972–6. doi: 10.2105/ajph.94.11.1972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tobacco: WHO region; [Last accessed on 2012 Dec 18]. World Health Organization (WHO) Available from: http://www.who.int/healthinfo/WHS2012_CORRIGENDUM.pdf . [Google Scholar]
- 5.Tobacco: WHO Report on the Global Tobacco Epidemic; 2011. [Last accessed on 2012 Dec 25]. World Health Organization (WHO) Available from: http://www.who.int/tobacco/surveillance/policy/country_profile/irn.pdf . [Google Scholar]
- 6.Mannino DM, Moorman JE, Kingsley B, Rose D, Repace J. Health effects related to environmental tobacco smoke exposure in children in the United States: Data from the Third National Health and Nutrition Examination Survey. Arch Pediatr Adolesc Med. 2001;155:36–41. doi: 10.1001/archpedi.155.1.36. [DOI] [PubMed] [Google Scholar]
- 7.Rauh VA, Whyatt RM, Garfinkel R, Andrews H, Hoepner L, Reyes A, et al. Developmental effects of exposure to environmental tobacco smoke and material hardship among inner-city children. Neurotoxicol Teratol. 2004;26:373–85. doi: 10.1016/j.ntt.2004.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jamrozik K. Estimate of death attributable to passive smoking among UK adults: Database analysis. BMJ. 2005;330:812–5. doi: 10.1136/bmj.38370.496632.8F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dowdell EB, Santucci ME. Health risk beahavior assessment: Nutrition, Weight and tobacco use in on urban seventh-grade class. Public Health Nurs. 2004;21:128–35. doi: 10.1111/j.0737-1209.2004.021206.x. [DOI] [PubMed] [Google Scholar]
- 10.Jones S, Sharp D, Husten C, Crossett L. Cigarette acquisition and proof of age among US high school students who smoke. Tob Control. 2002;11:20–5. doi: 10.1136/tc.11.1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dalton MA, Beach ML, Ada-Mejia AM, Longacre MR, Matzkin AL, Sargent JD, et al. Early exposure to movie smoking predicts established smoking by older teens and young adults. Pediatrics. 2009;123:551–8. doi: 10.1542/peds.2008-2102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Husten CG. Smoking cessation in young adults. Am J Public Health. 2007;97:1354–6. doi: 10.2105/AJPH.2007.117358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chang HY, Wu WC, Wu CC, Cheng JY, Hurng BS, Yen LL. The incidence of experimental smoking in school children: An 8-year follow-up of the child and adolescent behaviors in long-term evolution (CABLE) study. BMC Public Health. 2011;11:844. doi: 10.1186/1471-2458-11-844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Conley Thomson C, Siegel M, Winickoff J, Biener L, Rigotti NA. Household smoking bans and adolescents’ perceived prevalence of smoking and social acceptability of smoking. Prev Med. 2005;41:349–56. doi: 10.1016/j.ypmed.2004.12.003. [DOI] [PubMed] [Google Scholar]
- 15.Fakhfakh R, Hsairi M, Belaaj R, Romdhane H, Achour N. Epidemiology and prevention of smoking in Tunisia. current situation and perspectives. Arch Inst Pasture Tunis. 2001;78:59–67. [PubMed] [Google Scholar]
- 16.Ramlau R, Ditdkowska J, Wojciechowska U, Tarkowski W. Tobacco smoking in Wielkopolska towards the end of 20th century. Pneumonal Alergol Pol. 2005;73:128–34. [PubMed] [Google Scholar]
- 17.Mohtasham Amiri Z, Cirus Bakht S, NikRavesh Rad R. Cigarette smoking among male high school students in Rasht. J Guilan Univ Med Sci. 2008;17:100–7. [Google Scholar]
- 18.Lloyd-Richardson EE, Papandonatos G, Kazura A, Stanton C, Niaura R. Differentiating stages of smoking severity among adolescents: Stage-specific psychological and social influences. J Consult Clin Psychol. 2002;70:998–1009. doi: 10.1037//0022-006x.70.4.998. [DOI] [PubMed] [Google Scholar]
- 19.Ayatollahi SA, Mohammadpoor asl A, Rajaeefard AR. Predicting the stages of smoking acquisition in the male students of Shiraz's high schools, 2003. Nicotine Tob Res J. 2005;7:845–51. doi: 10.1080/14622200500330233. [DOI] [PubMed] [Google Scholar]
- 20.Alexander C, Piazza M, Mekos D, Valente T. Peer, schools, and adolescent cigarette smoking. J Adolesc Health. 2001;29:22–30. doi: 10.1016/s1054-139x(01)00210-5. [DOI] [PubMed] [Google Scholar]
- 21.Mercken L, Candel M, van Osch L, de Vries H. No smoke without fire: The impact of future friends on adolescent smoking behavior. Br J Health Psychol. 2011;16:170–88. doi: 10.1348/135910710X531608. [DOI] [PubMed] [Google Scholar]
- 22.Golbasi Z, Kaya D, Cetindag A, Capik E, Aydogan S. Smoking prevalence and associated attitudes among high school students in Turkey. Asian Pac J Cancer Prev. 2011;12:1313–6. [PubMed] [Google Scholar]
- 23.Gasparotti C, Limina RM, Donato F, Comincini F, Facchi G, Festa A, et al. A survey to assess consumption, attitudes and knowledge regarding tobacco smoke amongst secondary school students in Brescia (Italy) Ig Sanita Pubbl. 2010;66:623–35. [PubMed] [Google Scholar]
- 24.Maatoug J, Harrabi I, Gaha R, Bouyahia O, Gaha M, Kebaili R, et al. Intervention on smoking in adolescents in Sousse, Tunisia. Rev Pneumol Clin. 2010;66:179–86. doi: 10.1016/j.pneumo.2009.08.009. [DOI] [PubMed] [Google Scholar]
- 25.Witte K. Fear as motivator, fear as inhibitor: Using the extended parallel process model to explain fear appeal successes and failures. In: Andersen PA, Guerrero LK, editors. The Handbook of Communication and Emotion: Research, Theory, Applications, and Contexts. San Diego: Academic Press; 1998. pp. 423–50. [Google Scholar]
- 26.Witte K, Cameron KA, McKeon JK, Berkowitz JM. Predicting risk behaviors: Development and validation of a diagnostic scale. J Health Commun. 1996;1:317–41. doi: 10.1080/108107396127988. [DOI] [PubMed] [Google Scholar]
- 27.Wong NC, Cappella JN. Antismoking Threat and Efficacy Appeals: Effects on Smoking Cessation Intentions for Smokers with Low and High Readiness to Quit. J Appl Commun Res. 2009;37:1–20. doi: 10.1080/00909880802593928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Witte K, McKeon JK, Cameron KA, Berkovitz JM. The risk behavior scale: A health educator's tool. Michigan State University. 1995. [last accessed on 2009 June 15]. Available from: https://www.msu.edu/~wittek/rbd.htm .
- 29.Gharlipour Gharghani Z, Seyyed Hazavehei MM, Sharifi MH, Nazari M. Study of cigarette smoking status using extended parallel process model (EPPM) among secondary school male students in Shiraz city. Jundishapur J Health Sci. 2010;2:26–36. [Google Scholar]
- 30.Witte K, Allen MA. Meta-analysis of fear appeals: Implications for effective public health campaigns. Health Educ Behav. 2000;27:591–615. doi: 10.1177/109019810002700506. [DOI] [PubMed] [Google Scholar]
- 31.Hong H. An extension of the extended parallel process model (EPPM) in television health news: The influence of health consciousness on individual message processing and acceptance. Health Commun. 2011;26:343–53. doi: 10.1080/10410236.2010.551580. [DOI] [PubMed] [Google Scholar]
- 32.Pechmann C, Zhao GZ, Goldberg ME, Reibling ET. What to convey in antismoking advertisements for adolescents: The use of protection motivation theory to identify effective message themes. J Mark. 2003;67:1–18. [Google Scholar]
- 33.Sharot T, Korn CW, Dolan RJ. How unrealistic optimism is maintained in the face of reality. Nat Neurosci. 2011;14:1475–9. doi: 10.1038/nn.2949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Harris AJ, Hahn U. Unrealistic optimism about future life events: A cautionary note. Psychol Rev. 2011;118:135–54. doi: 10.1037/a0020997. [DOI] [PubMed] [Google Scholar]
- 35.Allahverdi Pour H, Heidar Nia AR, Kazem Nezhad A, Witte K, Shafiei F, Azad Fallah P. Applying fear appeals theory for preventing drug abuse among male high school students in Tehran. Scientific J Hamadan Univ Med Sci. 2006;13:43–50. [Google Scholar]
- 36.Arnett JJ. Optimistic bias in adolescent and adult smokers and nonsmokers. Addict Behav. 2000;25:625–32. doi: 10.1016/s0306-4603(99)00072-6. [DOI] [PubMed] [Google Scholar]
- 37.Ziaadini H, Kheradmand A, Nakhaee N, Taherzadeh H. Prevalence of cigarette smoking and relevant factors among school students in south of Iran. J Fundamentals Ment Health. 2008;10:239–45. [Google Scholar]
- 38.Sharifi-rad GH, Hazavei MM, Hasan-zadeh A, Danesh-amouz A. The effect of health education based on health belief model on preventive actions of smoking in grade one, middle school students. Arak Med Univ J. 2007;10:79–86. [Google Scholar]
- 39.Rahnavard Z, Mohammadi M, Rajabi F, Zolfaghari M. An educational intervention using health belief model on smoking preventive behavior among female teenagers. J Fac Nurs Midwifery Tehran Univ Med Sci. 2011;17:15–26. [Google Scholar]
- 40.Rogers RW. A protection motivation theory of fear appeals and attitude change. J Psych. 1975;91:93–114. doi: 10.1080/00223980.1975.9915803. [DOI] [PubMed] [Google Scholar]
- 41.Maddux JE, Rogers RW. Protection motivation and self-efficacy: A revised theory of fear appeals and attitude change. J Exp Soc Psychol. 1983;19:469–79. [Google Scholar]
- 42.Witte K. Putting the Fear Back into Fear Appeals: The extended parallel process model. Commun Monogr. 1992;59:329–49. [Google Scholar]
- 43.Cho H, Witte K. Managing fear in public health campaigns: A theory-based formative evaluation process. Health Promot Pract. 2005;6:482–90. doi: 10.1177/1524839904263912. [DOI] [PubMed] [Google Scholar]
- 44.Lorenzo-Blanco EI, Bares C, Delva J. Correlates of Children adolescents’ negative attitudes toward cigarettes: The role of gender, peer, parental, and environmental factors. Nicotine Tob Res. 2012;14:142–52. doi: 10.1093/ntr/ntr152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Schuck K, Otten R, Engels RC, Barker ED, Kleinjan M. Bidirectional influences between parents and children in smoking behavior: A longitudinal full-family model. Nicotine Tob Res. 2013;15:44–51. doi: 10.1093/ntr/nts082. [DOI] [PubMed] [Google Scholar]
- 46.Rafiee A, Haghighizadeh MH, Pouryazdan M. Prevalence rate and individual, familial and social characteristics associated. Jundishapur J Health Sci. 2010;1:16–21. [Google Scholar]
- 47.Fujimoto K, Valente TW. Decomposing the components of friendship and friends’ influence on adolescent drinking and smoking. J Adolesc Health. 2012;51:136–43. doi: 10.1016/j.jadohealth.2011.11.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Zadeh S, Sadeghi A. Epidemiological study of cigarette smoking in Urmia high school boys. Med J Tabriz Univ Med Sci Health Serv. 2001;34:27–32. [Google Scholar]
- 49.Leatherdale ST, Cameron R, Brown KS, McDonald PW. Senior student smoking at school, student characteristics, and smoking onset among junior students: A multilevel analysis. Prev Med. 2005;40:853–9. doi: 10.1016/j.ypmed.2004.09.033. [DOI] [PubMed] [Google Scholar]
- 50.Botvin GT, Griffin KW, Diaz T, Scheier LM, Williams C, Epstein JA. Preventing illicit drugs use in adolescents: Long-term follow-up data from a randomized control trial of a school population. Addict Behav. 2000;25:769–74. doi: 10.1016/s0306-4603(99)00050-7. [DOI] [PubMed] [Google Scholar]
- 51.Lintonen TP, Konu AI, Rimpela M. Identifying potential heavy smokers in early adolescence. Health Educ. 2000;101:159–68. [Google Scholar]
- 52.Moscato S, Black DR, Blue CL, Mattson M, Galer-Unti RA, Coster DC. Evaluating a fear appeal message to reduce alcohol use among “Greeks”. Am J Health Behav. 2001;25:481–91. [PubMed] [Google Scholar]
- 53.Witte K. Fear control and danger control: A test of the extended parallel process model (EPPM) Commun Monogr. 1994;61:113–34. [Google Scholar]
- 54.Kotowski MR, Smith SW, Johnstone PM, Pritt E. Using the Extended Parallel Process Model to create and evaluate the response efficacy of brochures to reduce the risk for noise-induced hearing loss in college students. Noise Health. 2011;13:261–71. doi: 10.4103/1463-1741.82958. [DOI] [PubMed] [Google Scholar]
- 55.Valente TW, Hoffman BR, Ritt-Olson A, Lichtman K, Johnson CA. Effects of a Social-Network method for group assignment strategies on Peer-Led Tobacco prevention programs in schools. Am J Public Health. 2003;93:1837–43. doi: 10.2105/ajph.93.11.1837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ulgen H, Ozturk C, Armstrong M. Effect of self-efficacy on Turkish children's perceptions of the advantages/disadvantages of smoking. Asian Pac J Cancer Prev. 2012;13:795–8. doi: 10.7314/apjcp.2012.13.3.795. [DOI] [PubMed] [Google Scholar]
- 57.Asad Pour M, Ghofrani Pour F, Haji Zadeh S. The effect of group discussion on smoking in male students of high school in Rafsanjan city. Daneshvar Med J. 2001;8:1–6. [Google Scholar]