

Abstract
Objectives:
Childhood obesity/underweight status and caries are both important public health problems. This study aims to investigate the caries status and its association with body weight in 8-year-old children in Qingdao, China.
Materials and Methods:
We initiated a cross-sectional investigation on 744 children aged 8 years during the Oral Health Survey in 2012. Dental caries assessments were carried out and weight status was recorded accordingly. The resulting caries status including caries prevalence, dmft (deciduous dentition), and (dmft + DMFT) (mixed dentition), as well as BMI indices were analyzed for comparison and correlation.
Results:
The prevalence of dental caries among the 744 children aged 8 years participating in this survey was 86.3%. The caries status represented by dmft (deciduous dentition) and (dmft + DMFT) (mixed dentition) values was 4.31 and 4.85, respectively, and the restoration rate was extremely low, which was no more than 3.0%. Significant difference was found in dmft/(dmft + DMFT) values between different BMI groups, and underweight individuals were found to have the highest dmft/(dmft + DMFT) value. An inverse relationship between body BMI and dmft/(dmft + DMFT) index was identified based on Pearson's correlation.
Conclusions:
A severe state of caries disease was revealed in 8-year-old children in the Chinese city of Qingdao, for whom urgent dental intervention and treatment were needed. Furthermore, underweight individuals were found with the most severe caries experience, indicating caries may affect the development and growth of the afflicted children. Thus, more emphasis should be placed on improving their dental health, with caries prevention being given the priority.
Keywords: Caries, cross-sectional survey, epidemic survey, obesity, weight
INTRODUCTION
Caries is a dental health concern worldwide which may affect people of all ages. Caries activity usually causes tooth decay or cavities and can even lead to the loss of afflicted teeth, which is particularly harmful to children's growth and development. The World Health Organization (WHO) reported that 60–90% of schoolchildren worldwide experience caries, with the disease being most prevalent in Asian and Latin American countries.[1] Surveys among the US population showed an incidence of 45.3% in children with either past or present coronal caries, and the rate of caries has been increasing in developing countries with the increasing consumption of highly refined sugars in the diet.[2] According to the Third National Epidemiological Survey of Dental Health in China in 2007, the prevalence of dental caries among 5-year-old children in China was 66.0%, with a mean number of 3.5 per capita of caries teeth.[3] Therefore, caries disease has been ranked by the WHO as the third most important disease that requires worldwide attention for its prevention and treatment.
Studies on the etiology of dental caries have identified some risk factors, such as consuming foods and beverages with a high content of refined carbohydrates, receiving bottle-feed for a prolonged period, having deficient hygiene, etc.[4] Given the strong evidence supporting the relationship of dental caries with irregular dietary patterns and the link between abnormal dietary intake and obesity,[5] an association between dental caries and obesity might be biologically plausible. Several reports described the link between caries and weight, indicating that obese children had more caries than children in the normal-weight group.[6,7,8,9,10] However, others concluded that there was no significant difference in the DMFT/dmft score among different body mass index (BMI) groups in 3–8-year-old children.[11] Therefore, no consensus has been reached on the relationship between obesity and dental caries in children.
Qingdao is a key economic center and a port city of China. Yet, till now, there is no national data concerning caries status among school children native of this area, and less is known about the relationship of caries and weight status. In this study, a large-scale population-based oral health survey among 8-year-old children was conducted from January to July in 2012 at Qingdao, Shandong Province, China, supported by the Qingdao government. The aims of the present study were: (1) To assess the caries prevalence and severity in 8-year-old children of Qingdao and (2) to assess the relationship between caries disease and the weight status in 8-year-old children of Qingdao.
MATERIALS AND METHODS
Study design
In this cross-sectional study, oral health survey was conducted from January to July in 2012. Eight-year-old children from 28 public elementary schools in Qingdao were invited to participate in this survey. All children and their parents were informed about the nature of the experiment and they gave their written informed consent. The study was conducted after obtaining the approval of the ethical committee of the Qingdao Municipal Hospital.
Clinical examination
The oral examination, mainly visual inspection plus probing, was undertaken according to the WHO criteria for the diagnosis of caries.[12] A dental mirror and exploring probe were employed for assistance. Generally, dental caries was diagnosed only if there was a prominent color, shape, or caries-like change in pit, fissure, or smooth surface. Caries experience was evaluated on all the subjects’ teeth included in the deciduous (dmft) or mixed (dmft + DMFT) dentition. DMFT (number of decayed, missing, and filled teeth in permanent dentition; in this study, of 8-year-old children; permanent teeth included central incisors, lateral incisors, and first molars in mandibular and maxillary bone) and dmft (number of decayed, missing, and filled teeth in deciduous dentition) indices were recorded from the dental charts. All examinations were performed by eight calibrated professional dentists who were trained for the assessment of the dmft/(dmft + DMFT) index prior to the oral survey. In an initial evaluation on caries detection, the inter-examiner kappa values were above 0.80, indicating good agreement among the examiners.
Weight evaluation
Weight was evaluated using a single calibrated scale (Tanita Ultimate series 2204®; Tanita Corporation Inc., Tokyo, Japan) (corrected to the nearest 0.1 kg). Height was measured using Harpenden stadiometer (Holtain Ltd, Dyved, UK) by having the subject standing straight without shoes (corrected to the nearest 0.1 cm). BMI was calculated using the following formula: weight in kg/(height in meters squared).[13] Weight status was defined by gender-related BMI according to the Centers for Disease Control and Prevention (CDC) guidelines as follows:[13] underweight (BMI ≤5th percentile), normal weight (BMI >5th and <85th percentile), at risk of overweight (BMI ≥85th and <95th percentile), and overweight (BMI ≥95th percentile). All data were collected on standardized forms, and a database was created with all the collected information, including age and gender. To protect confidentiality, the database was password secured and accessible to only one data analyst.
Statistical analysis
Descriptive data were obtained for all outcome variables and reported as mean ± SD. The Student's t-test, Chi-square test, and one-way analysis of variance (ANOVA) were applied for the statistical evaluation of means and comparisons of proportions. The overall caries disease status in each BMI group was compared based on dmft, (dmft + DMFT), and caries prevalence. Pearson's correlation was applied between dmft/(dmft + DMFT) and BMI value to assess the relationship between caries and weight status. Statistical analyses were performed with R software (version 2.13.1). All reported P values were two-sided at 90% confidence level.
RESULTS
A total of 758 children from 28 primary schools in Qingdao were initially included in this study. The withdrawal of 14 children was due to the missing values and it resulted in the final group of 744 children that consisted of 384 males and 360 females. Subjects fell in the age range of 8–8.5 years, with a nearly symmetric gender distribution (51.6% males and 48.4% females). The total number of teeth that went through inspection was 17,139 (averaging 23.0 per capita) and the decayed teeth numbered 3008 (averaging 4.0 per capita). Results showed that 642 (86.3% of the total; 327 males and 315 females) children suffered from dental caries and only 102 of them (13.1% of the total; 57 males and 45 females) were caries-free. Approximately 6.0% of the children in the study (n = 45; 16 males and 29 females) were underweight, 73.9% (n = 550; 264 males and 286 females) had normal weight, while 9.8% (n = 73; 38 males and 35 females) and 10.2% (n = 96; 76 males and 10 females) were at risk of overweight and overweight, respectively.
Caries status in 8-year-old children in Qingdao
The prevalence of dental caries was 85.2% in males and 87.5% in females. No significant difference was found between the two genders (P > 0.05) with respect to caries prevalence. The mean dmft values were 4.29 in males and 4.34 in females in deciduous dentition. Among the permanent teeth, except for the first permanent molar, no caries was found in the permanent central or lateral incisors. The mean DMFT values were 0.43 in males and 0.61 in females in permanent dentition. The constitution of d, m, dmft, and DMFT index between the two genders was similar (P > 0.05), except for f value which was significantly higher in males than in females (P < 0.1). Similarly, significantly higher restoration rates were found in male children (2.9%) than in female children (1.2%) (P < 0.01) Table 1.
Table 1.
Caries experience in children

Teeth with the highest caries prevalence of 51.6% were the right mandibular second deciduous molar (teeth 85) (52.6% in females and 50.7% in males), followed by teeth 75, 74, and 84 with caries prevalence of 50.2, 47.2, and 47.0%, respectively [Figure 1]. Significantly higher caries prevalence was found in mandibular deciduous molars (49.0%) as compared with maxilla deciduous molars (38.1%) [Figure 1]. Among the newly erupted permanent first molars, teeth 36 and 46 were found to have a high caries prevalence of 15.8 and 15.0%, respectively, in contrast to teeth 16 and 26 that had relatively low caries prevalence of 5.7 and 5.0%, respectively [Figure 1].
Figure 1.
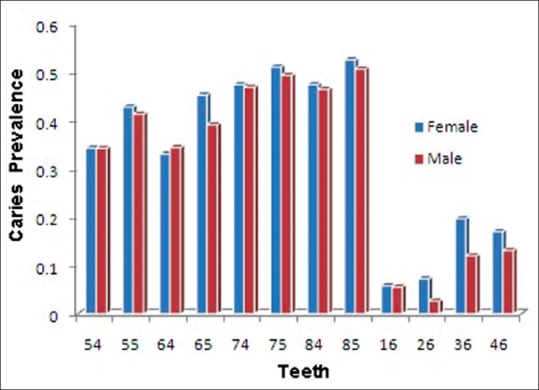
Caries prevalence of each tooth based on gender. The mandibular second deciduous molars (teeth 85) accounted for 51.6% of caries prevalence among the children. There was a significantly higher rate of caries prevalence in mandibular deciduous molars (49.0%) than in maxillary deciduous molars (38.1%). Among the newly erupted permanent first molars, teeth 36 and 46 were found with the highest caries prevalence of 15.8 and 15.0%, respectively
Weight status in 8-year-old children in Qingdao
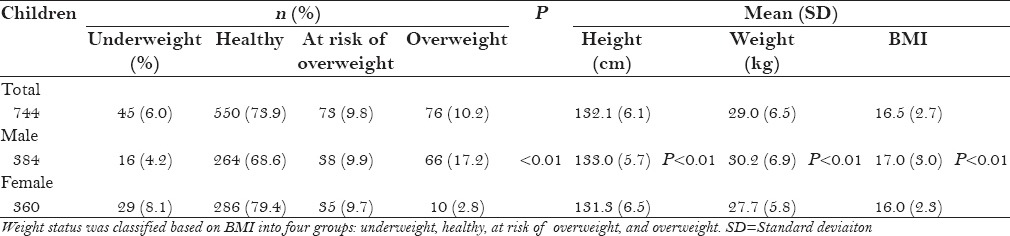
Among the female children, 8.1% fell into the underweight category and 79.4% fell into the healthy category, while 9.7 and 2.8% were considered as at risk of overweight and overweight, respectively. Among the male children, 14.2% were underweight and 68.6% were healthy, while 9.9 and 17.2% were considered to be at risk of overweight and overweight, respectively. Considering all the male and female children, the mean height was 132.1 cm and the mean weight was 19.0 kg. Significant difference was detected in the weight and height between the two genders (P < 0.01) [Table 2].
Table 2.
Classification of body weight status according to CDC guidelines
Relationship between caries disease and weight status
Values of dmft/(dmft + DMFT) in each BMI group were compared and the results showed statistically significant differences between different BMI groups [P < 0.1 for (dmft + DMFT), P < 0.01 for dmft] [Table 3], with the highest dmft/(dmft + DMFT) values in the underweight group. No significant difference was found in the caries prevalence between different BMI groups [Table 3]. Pearson's correlation between dmft/(dmft + DMFT) and BMI was significant [P = 0.04 for dmft, P = 0.004 for (dmft + DMFT)], with R values of −0.075 and −0.104 for dmft and (dmft + DMFT), respectively. These results indicated an inverse relationship between BMI and caries severity [Figure 2].
Table 3.
Comparison of caries status according to BMI classification

Figure 2.
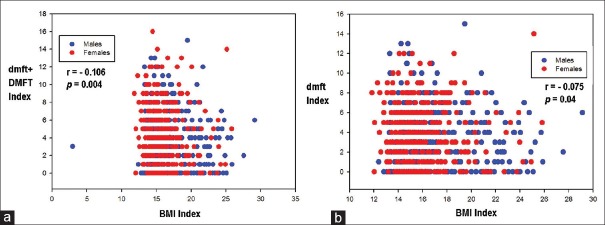
Pearson's correlation of BMI and caries experience. (a) Caries severity was evaluated by (dmft + DMFT) values (b) dmft values. Pearson's correlation between caries severity and BMI index was significant (P = 0.004 for (a) and P = 0.04 for (b))
DISCUSSION
Qingdao is located in the southern part of Shandong Peninsula, facing the Yellow Sea in the east and south. It is one of the most significant seaports of eastern China. In 2012, the Qingdao government initiated a public welfare project of oral health examination, pit and fissure sealant, and caries filling treatment in public primary school students, which provided an opportunity to systematically assess the caries status in children of Qingdao.
The status of dental caries in 8-year-old children in Qingdao
For assessment of dental caries, we used the dmft/DMFT index, as it is one of the most commonly used indices in epidemiological studies for evaluating caries experience. We found that firstly, the 744 children aged 8 years in Qingdao were generally in poor oral health status. The prevalence of caries among all individuals was 86.3%. Although this rate was similar to that reported in other domestic studies (85.4% of caries prevalence in children of similar age group in Guangzhou), the average dmft index (4.31) in our study was significantly higher than that reported (dmft index: 3.11) in the study of Guangzhou.[14] Furthermore, caries prevalence and dmft value in these 8-year-old children from Qingdao were significantly higher than those reported from other countries such as Sudan.[15] The reason might be the changes in dietary habit that happened during the last decade. Changes in dietary content of the children of Qingdao have been observed in the past few years, with them consuming significantly more desserts than ever before; yet, their oral health is at a low level. Secondly, it was noted that averagely, only 2.1% of the decayed teeth were treated with filling. This finding was consistent with the restoration rate of children in a previous regional study,[14] supporting the widespread negligence for the oral health of children in China. Therefore, dental treatment and dental health education of children, parents, teachers, and even the whole society are urgently needed. Thirdly, the significantly higher restoration rate in males might partially reflect that male children have been receiving more oral care than female children. Our findings might add some support to the notion that the restoration rate correlated with the regional economy, culture, and education. Lastly, our data showed that the mandibular second deciduous molars accounted for over 50% of all the decayed teeth, which suggested the necessity to pay more attention to protecting the particular teeth from caries at an early stage.
The status of body weight in 8-year-old children in Qingdao
The prevalence of obesity in children has been a major public health concern. Weight status in children was measured by BMI, according to gender and age-ranked percentages. Our study showed that 10% of children were overweight among all the 8-year-old children, which is slightly lower than the corresponding values previously reported by other analyses conducted in other Chinese regions.[16,17] According to the studies conducted in Chengdu and Shanghai,[16,17] the prevalence of obesity was about 3%, respectively, which was similar to our data on female children but significantly lower than our data on male children (17.2%). Methodological differences (e.g. criteria recommended by CDC guidelines, International Obesity Task Force, or World Health Organization) might have contributed to such differences, causing the difficulty in comparing the results of the studies. In other recent studies, based on the same criteria recommended by CDC guidelines,[18] 31.0% of US children were at risk of overweight and 16.0% were overweight; both percentages are obviously higher than those obtained in our survey.
Relationship between caries severity and weight status
Caries is usually regarded as a consequence of frequent ingestion of fermentable sugars, which can also lead to obesity. As a result, association between caries and obesity has long been suspected.[6,7,8,9,10] However, findings of obesity–caries relationship in children from different countries have actually been mixed and inconclusive. Conclusions on positive links, no links, and inverse links are all present. For example, the sole study from China reported no correlation between obesity and caries among 280 children.[19] This can be due to the confounding factors such as age, gender, dentition, race/ethnicity, and socioeconomic status, which might affect the final conclusion.[16,20,21,22,23,24] To eliminate these potential confounding factors, we conducted our study on subjects from a relatively homogeneous environment. They were all children from a single specific age group from the native population with similar living environment and eating habits, from public primary schools with similar socioeconomic background, and with a nearly symmetric gender distribution. Also, we utilized two indices [dmft and (dmft + DMFT)] to assess the caries severity in children both in deciduous and mixed dentition. Regardless of the index used in the analysis, instead of a previously suspected positive link, a weak inverse relationship of body weight and caries severity was found and the comparison also showed underweight individuals to have significantly more severe caries disease. This finding suggested that the relationship of obesity and caries was not as straightforward as was earlier suspected.[5] Moreover, although not focusing on an identical age group, our result is consistent with a nationally representative survey based on a dataset of 10,800 American adolescents National Health and Nutrition Examination Survey (NHANES) III 1988–1994 and NHANES 1999–2002)[24] which suggested that overweight status may be associated with a somewhat decreased risk for caries.
Our results showed that underweight children were more likely found with more severe caries disease, regardless of primary or mixed dentition. This result was consistent with Mojarad's,[25] Werner's,[26] and Roswitha's reports.[27] This observation might be due to the following factors. Nowadays, in China, the living standard has improved significantly along with the rapid progress in economy. In addition, China's one child policy has turned many children into the “Little Emperor” of their families, which argues against the fact that underweight status of the children is due to poverty. Thus, it is more plausible that caries might be one cause behind children being underweight. The following mechanisms might account for the observed inverse relationship between BMI and dmft/(dmft + DMFT) index.[28] Firstly, untreated caries might have caused severe pain and discomfort in children and, thus, reduced food intake.[29] Secondly, caries can also lead to infection, irritability, and disturbed sleeping habits, which might reduce the quality of life and affect the growth.[30]
One limitation of our study is the use of cross-sectional data to examine the link between caries experience and weight status. To test the cause–effect relationship, a longitudinal design should be conducted. However, the strength of our study is the use of localized and relatively simple representative samples of Chinese children to explore and control for multiple confounding factors, and our results yielded consistent findings with deciduous and mixed dentition.
CONCLUSIONS
This study was a population-based epidemiological survey on caries and body weight status in 8-year-old children in Qingdao, China. A severe state of caries disease was revealed in this survey of 744 children aged 8 years, for whom urgent dental intervention and treatment were needed. Our study identified a weak negative association between caries severity and weight status in this pilot population, indicating caries lesions might be a reason affecting the growth and development of children. Our finding suggested that until more evidence is available, obesity should not be considered as a risk factor for caries diagnosis and treatment planning in children.
Footnotes
Source of Support: This work was supported by Grant 31300424 from the Natural Science Foundation of China
Conflict of Interest: None declared.
REFERENCES
- 1.Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83:661–9. [PMC free article] [PubMed] [Google Scholar]
- 2.Shivakumar KM, Vidya SK, Chandu GN. Dental caries vaccine. Indian J Dent Res. 2009;20:99–106. doi: 10.4103/0970-9290.49066. [DOI] [PubMed] [Google Scholar]
- 3.Qi X. Beijing, China: People's Medical Publishing House; 2008. The Third National Sampling Epidemiological Survey on Oral Health; pp. 72–6. [Google Scholar]
- 4.Masood M, Yusof N, Hassan MI, Jaafar N. Assessment of dental caries predictors in 6-year-old school children-results from 5-year retrospective cohort study. BMC Public Health. 2012;12:989. doi: 10.1186/1471-2458-12-989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gidding SS, Dennison BA, Birch LL, Daniels SR, Gillman MW, Lichtenstein AH, et al. American Heart Association; American Academy of Pediatrics. Dietary recommendations for children and adolescents: A guide for practitioners: Consensus statement from the American Heart Association. Circulation. 2005;112:2061–75. doi: 10.1161/CIRCULATIONAHA.105.169251. [DOI] [PubMed] [Google Scholar]
- 6.Thippeswamy HM, Kumar N, Acharya S, Pentapati KC. Relationship between body mass index and dental caries among adolescent children in South India. West Indian Med J. 2011;60:581–6. [PubMed] [Google Scholar]
- 7.Loyola-Rodriguez JP, Villa-Chavez C, Patiñio-Marin N, Aradillas-Garcia C, Gonzalez C, de la Cruz-Mendoza E. Association between caries, obesity and insulin resistance in Mexican adolescents. J Clin Pediatr Dent. 2011;36:49–53. doi: 10.17796/jcpd.36.1.e25411r576362262. [DOI] [PubMed] [Google Scholar]
- 8.Costacurta M, Di Renzo L, Bianchi A, Fabiocchi F, De Lorenzo A, Docimo R. Obesity and dental caries in paediatric patients. A cross-sectional study. Eur J Paediatr Dent. 2011;12:112–6. [PubMed] [Google Scholar]
- 9.Vázquez-Nava F, Vázquez-Rodríguez EM, Saldívar-González AH, Lin-Ochoa D, Martinez-Perales GM, Joffre-Velázquez VM. Association between obesity and dental caries in a group of preschool children in Mexico. J Public Health Dent. 2010;70:124–30. doi: 10.1111/j.1752-7325.2009.00152.x. [DOI] [PubMed] [Google Scholar]
- 10.Alm A, Fåhraeus C, Wendt LK, Koch G, Andersson-Gäre B, Birkhed D. Body adiposity status in teenagers and snacking habits in early childhood in relation to approximal caries at 15 years of age. Int J Paediatr Dent. 2008;18:189–96. doi: 10.1111/j.1365-263X.2007.00906.x. [DOI] [PubMed] [Google Scholar]
- 11.D’Mello G, Chia L, Hamilton SD, Thomson WM, Drummon BK. Childhood obesity and dental caries among paediatric dental clinic attenders. Int J Paediatr Dent. 2011;21:217–22. doi: 10.1111/j.1365-263X.2011.01112.x. [DOI] [PubMed] [Google Scholar]
- 12.Oral health surveys-basic methods. 4th ed. Geneva: 1997. World-Health-Organization. [Google Scholar]
- 13.Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. 2000 CDC growth charts for the United States: Methods and development. Vital Health Stat 11. 2002:1–190. [PubMed] [Google Scholar]
- 14.Fan W, Huang S, Zheng Z, Chen W, Zhang J. Epidemiological survey on caries state of deciduous teeth in children from Guangzhou, China. J Dent Prev Treat. 2010;18:127–30. [Google Scholar]
- 15.Raadal M, Elhassan FE, Rasmussen P. The prevalence of caries in groups of children aged 4-5 and 7-8 years in Khartoum, Sudan. Int J Paediatr Dent. 1993;3:9–15. doi: 10.1111/j.1365-263x.1993.tb00041.x. [DOI] [PubMed] [Google Scholar]
- 16.Zhang M, Guo F, Tu Y, Kiess W, Sun C, Li X, et al. Further increase of obesity prevalence in Chinese children and adolescents- cross-sectional data of two consecutive samples from the city of Shanghai from 2003 to 2008. Pediatr Diabetes. 2012;13:572–7. doi: 10.1111/j.1399-5448.2012.00877.x. [DOI] [PubMed] [Google Scholar]
- 17.Li P, Yang F, Xiong F, Huo T, Tong Y, Yang S, et al. Nutritional status and risk factors of overweight and obesity for children aged 9-15 years in Chengdu, Southwest China. BMC Public Health. 2012;12:636. doi: 10.1186/1471-2458-12-636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA. 2004;291:2847–50. doi: 10.1001/jama.291.23.2847. [DOI] [PubMed] [Google Scholar]
- 19.Wu L, Chang R, Mu Y, Deng X, Wu F, Zhang S, et al. Association between obesity and dental caries in Chinese children. Caries Res. 2013;47:171–6. doi: 10.1159/000344017. [DOI] [PubMed] [Google Scholar]
- 20.Spiegel KA, Palmer CA. Childhood dental caries and childhood obesity. Different problems with overlapping causes. Am J Dent. 2012;25:59–64. [PubMed] [Google Scholar]
- 21.Gerdin EW, Angbratt M, Aronsson K, Eriksson E, Johansson I. Dental caries and body mass index by socio-economic status in Swedish children. Community Dent Oral Epidemiol. 2008;36:459–65. doi: 10.1111/j.1600-0528.2007.00421.x. [DOI] [PubMed] [Google Scholar]
- 22.Nurelhuda NM, Ahmed MF, Trovik TA, Åstrøm AN. Evaluation of oral health-related quality of life among Sudanese schoolchildren using Child-OIDP inventory. Health Qual Life Outcomes. 2010;8:152. doi: 10.1186/1477-7525-8-152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhang R, Lin HC, Zhi QH, Yang JY, Tu JZ. A study on oral health behavior and other related factors between children with high dmft and no caries. Zhonghua Kou Qiang Yi Xue Za Zhi. 2007;42:298–9. [PubMed] [Google Scholar]
- 24.Kopycka-Kedzierawski DT, Auinger P, Billings RJ, Weitzman M. Caries status and overweight in 2- to 18-year-old US children: Findings from national surveys. Community Dent Oral Epidemiol. 2008;36:157–67. doi: 10.1111/j.1600-0528.2007.00384.x. [DOI] [PubMed] [Google Scholar]
- 25.Mojarad F, Maybodi MH. Association between dental caries and body mass index among hamedan elementary school children in 2009. J Dent (Tehran) 2011;8:170–7. [PMC free article] [PubMed] [Google Scholar]
- 26.Werner SL, Phillips C, Koroluk LD. Association between childhood obesity and dental caries. Pediatr Dent. 2012;34:23–7. [PubMed] [Google Scholar]
- 27.Heinrich-Weltzien R, Monse B, Benzian H, Heinrich J, Kromeyer-Hauschild K. Association of dental caries and weight status in 6- to 7-year-old Filipino children. Clin Oral Investig. 2013;17:1515–23. doi: 10.1007/s00784-012-0849-3. [DOI] [PubMed] [Google Scholar]
- 28.Sheiham A. Dental caries affects body weight, growth and quality of life in pre-school children. Br Dent J. 2006;201:625–6. doi: 10.1038/sj.bdj.4814259. [DOI] [PubMed] [Google Scholar]
- 29.Marques AP, Messer LB. Nutrient intake and dental caries in the primary dentition. Pediatr Dent. 1992;14:314–21. [PubMed] [Google Scholar]
- 30.Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: Child and parent perspectives. Pediatr Dent. 2003;25:431–40. [PubMed] [Google Scholar]