

Abstract
Objectives:
The study was designed to determine the prevalence of dental caries and partial edentulism, in addition to assessing the oral hygiene status and restorative care among adults in a community-based outreach program in Port Harcourt.
Materials and Methods:
A cross-sectional study was conducted among adults who participated in oral health screening program, which took place in Alakahia and Obigbo rural communities in Port Harcourt, Rivers State, Nigeria. After a brief oral health education, clinical examination was conducted and the diagnosis of caries was made based on the guidelines laid down by World Health Organization. Prevalence of caries was measured using decayed missing and filled teeth (DMFT) index, and oral hygiene status was assessed using the OHI-S. The restorative index [(F/F + D) ×100] was also calculated and the sociodemographic factors of the subjects were noted. Chi-square test, independent t-test and descriptive statistic were employed for analysis.
Results:
One fifty-five females (53.8%) and 133 males (46.2%) attended the events and their mean age was 29.3 ± 10.5 years. About one-third of the participants (35.1%) presented with dental caries. The mean DMFT for the whole group was 0.67 ± 2.0. The restorative index for the subjects was 26.8%. The oral hygiene status of most of the participants was fair. This was significantly better in females than in males (P = 0.002).
Conclusion:
Although about one-third of the participants had dental caries, only a quarter of them had received restorative care. Most of the respondents had fair and poor oral hygiene, this suggests the need to educate and motivate the community toward adopting and maintaining positive oral health attitudes and practices.
Keywords: Community, dental caries, oral health, oral health education, oral health practice, restorative index, screening
INTRODUCTION
Poor oral health impacts a great deal on the quality o life of children, adults, and the aged. It affects children nutrition, growth, and development as well as attendance at school. In adults, routine daily activities may be disrupted leading to considerable economic loss.[1,2] Good oral health is beyond good dentition; it includes absence of pain, diseases, or any disorders of the dentofacial region and oral cavity.[3]
Dental caries and periodontal diseases are the major oral health problems and indicators of oral health burden all over the world.[4,5] Although the prevalence of dental caries varies worldwide, it is believed that the disease has a high prevalence, wide geographic spread, and graded severity.[2,4,5] The impact of the disease on the economy and the quality of life of people make it a health condition of public interest.[5,6] Recent epidemiological reports suggest that there is resurgence in the scourge of dental caries in the developed countries, where the disease had hitherto been significantly controlled.[1,7] In the developing countries, however, studies have consistently shown that the burden of oral diseases such as caries and periodontal diseases is increasing.[8]
Dental caries is age related and literature suggests that caries incidence had three peaks: At about age 7 years for coronal decay of the primary dentition; at about age 14 years for coronal decay of the permanent dentition; and at about age 30–40 years for root surface decay.[9] Bacterial plaque has been implicated in the aetiopathology of dental caries and periodontal diseases. It is believed that good oral hygiene practices will to some extent help in the control of these major oral diseases.[9,10] Before effective strategies for oral health care and prevention could be designed, epidemiological data on major oral diseases is most necessary.[11,12]
There is paucity of reports relating to community-based epidemiologic studies on oral health status of adults in Nigeria particularly, those residents in the south–south region of the country. The World Health Organization (WHO) recommends epidemiological studies on 35–44 years and 65–74 years age groups due to their relevance in describing and analyzing the cumulative damage of caries on people's oral health over the years.[6] Information from these adult population groups is also used to generate evidence on final outcomes of dental care delivered to people during their entire life cycle.[13] This study was therefore designed to determine the prevalence of dental caries and partial edentulism among adults in a community-based outreach program in Port Harcourt, Nigeria. It also assessed the oral hygiene status and restorative care of the participants.
MATERIALS AND METHODS
This was a cross-sectional study involving individuals who participated in the oral health screening programs organized by two of the authors in collaboration with the final year dental students of the University of Port Harcourt in 2012. The programs took place in two rural communities of Alakahia and Obigbo in Obio/Akpor and Obigbo Local Government Areas of Rivers State, Nigeria, respectively. The records of individuals who presented for the oral health screening during the outreach program were employed for the study. Ethical approval was obtained from the Research and Ethics Committee of the University of Port Harcourt Teaching Hospital and informed consent obtained from the participants.
The participants were taught good oral hygiene practices before the screening. Common features of oral diseases and the need to seek preventive oral health care services was emphasized. The biodata of the participants, the phone number, and the date of screening were recorded following which a brief interview and examination were conducted. The records were coded to ensure anonymity. Oral examination was carried out and caries was diagnosed based on WHO guidelines.[14] The prevalence of dental caries was assessed using the modified decayed missing and filled teeth (DMFT) index.[14] The restorative index was calculated using the formula: (F/F + D) × 100.[15] The oral hygiene status was assessed using the simplified oral hygiene index (OHI-S) by Green and Vermillion.[16] According to this index, oral hygiene index of between 0.0 and 1.2 was described as good, 1.3 and 3.0 as fair, and between 3.1 and 6.0 is said as poor. Appropriate referral to nearby oral health care facilities was made where necessary.
Statistical analysis
The data obtained were entered into SPSS version 19 (SPSS Inc, Chicago, IL, USA). Descriptive statistics was generated; Chi-square and independent t-test was employed to determine the association between variables. The level of significance was set at 95% confidence interval and P < 0.05 was considered to be significant.
RESULTS
A total of 288 individuals comprising 155 females (53.8%) and 133 males (46.2%) participated at the events. The 20–24 years old age group had the highest number of participants (42.0%) and this was followed by the 25–29 years old age group (18.4%). The 55–64 years old age group had the least number of participants (2.4%). The mean age of the participants was 29.3 ± 10.5 years [Table 1].
Table 1.
Distribution of mean DMFT according to gender and age
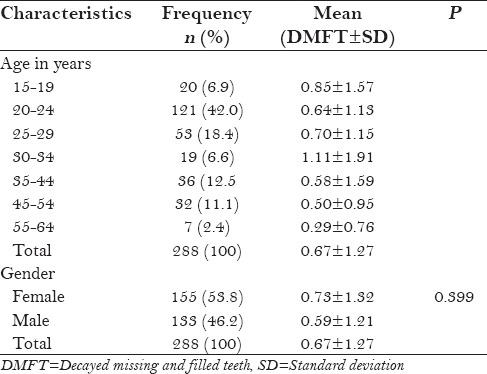
About 35.1% of the participants presented with dental caries and the number of carious teeth ranged from one to six with a mean of 3.4 (±2.1). The mean DMFT for the whole group was 0.67 ± 1.27. There was no statistically significant difference in the mean DMFT between the males and the females (P = 0.399). The lowest mean DMFT (0.29 ± 0.76) was recorded in the 55–64 years age group, whereas the highest (1.11 ± 1.91) was in the 30–34 years age group. The mean DMFT did not follow a particular trend among the different age groups [Table 1].
The prevalence of partial edentulousness was 28.5% and the average number of missing teeth was 3.4 (±2.3). Majority of the participants had no filled teeth. Six and five individuals had two and five filled teeth each, respectively. The restorative index for the subjects was 26.8%.
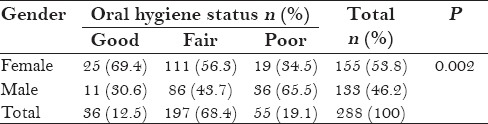
Regarding oral hygiene status, 36 participants (12.5%) had good oral hygiene out of which 25 (69.4%) were females. In 197 individuals (68.4%), the oral hygiene was fair and 111 of these were females (56.3%). Fifty-five participants (19.1%) had poor oral hygiene and 36 (70.6%) of these were males. There was a statistically significant difference between the oral hygiene status (P = 0.002) of male and female participants [Table 2].
Table 2.
Gender distribution of oral hygiene status
DISCUSSION
Gender is a major determinant of oral hygiene status. The result of this study showed that females had significant better oral hygiene status than males. This finding is in agreement with that of other studies.[5,17,18,19] The better oral hygiene status reported among women has been attributed to better oral health care seeking behavior exhibited by women as compared with men.[19] The oral hygiene status recorded in this study was grossly inadequate considering the pivotal role of plaque and calculus in the aetiopathology of dental caries and periodontal diseases, which constitute the primary oral health diseases of worldwide distribution and significance. The number of elderly representation in this study was grossly inadequate and the data may not represent the true oral health indexes for this age group. A bigger survey with good representation of the different age groups is recommended.
The mean age in the present study was comparable to 34.9 ± 14.2 years reported in a similar epidemiologic study on oral health status among adult subjects in a rural community in India.[20] About 35% of the individuals who participated in the present study had dental caries. This was higher than the 22.6% previously reported among adult patients in Port Harcourt, Nigeria,[5] and slightly higher than 30% reported by Nguyen et al.[11] Those who had more than one untreated tooth decay were more than those who had only one tooth decay. This underscored the severity of the disease among the participants. In a Sudanese study,[21] 87.7% of the teeth examined had untreated decay and in the survey conducted in a rural community in India, less than 20% of the people who were surveyed did not have untreated caries.[20] More females had dental caries in our study, however, this was not significant. This finding is comparable to the previous report, which states that females had a higher prevalence and severity of dental caries than males and that no significant difference occurred in caries prevalence between male and female genders.[22]
The prevalence of tooth decay is noted to be on the increase in Africa and in developed countries where hitherto it had been reported to be on the decline.[7] Nonetheless, the hallmark of oral health in Africa remained low prevalence of dental caries.[4] Our result on caries prevalence revealed a mean DMFT of 0.67 ± 1.27 for the whole group, whereas that of the different age groups varied from 0.29 to 1.1. This community-based dental caries prevalence was much lower than the DMFT score of 3.57 previously found among patients attending the Oral Diagnosis Clinic of the University of Port Harcourt Teaching Hospital.[5] The higher DMFT score in the previous study may be due to the fact that the study was conducted among those having oral symptoms, which necessitated their seeking oral health care services. Umesi-Koleoso et al.[22] reported a mean DMFT of 0.72 ± 1.67, whereas a mean DMFT of 0.85 ± 1.50 was reported by Okoye and Ekwueme[23] among younger age groups. A WHO data showed that several sub-Saharan African countries have a DMFT of 0.0–1.1.[4] A significantly higher scores were reported outside Africa for subjects in the same age group. Among African American adults, a mean DMFT of 8.83 was reported for the 18–34 age group.[24] Hopcraft and Morgan,[25] on the other hand, reported a DMFS score of 9.61 for adult subjects belonging to 26–30 years age group. For subjects in the 35–44 years age group and those older than 45 years, the mean DMFT reported for Brazilian and Chilean population was not less than 15.[6]
The restorative index (26.8%) obtained in this study was similar to 25.3% reported in a previous study.[5] This suggests a low level of restorative care among the subjects in both cases probably because of financial constraints, poor accessibility, and lack of awareness. In a German study,[26] the caries index was found to be between 90% and 95%; this high index was attributed to the fact that tooth filling and endodontic treatments are fully covered under the National Health Insurance System. Poverty, poor accessibility, inadequate number, and skewed distribution of oral health care personnel have been implicated in poor utilization of oral care services in developing countries.[4,7,27]
The prevalence of partial edentulism in the present study was 28.5% and the mean number of missing teeth was 3.4. In a cross-sectional study conducted by Kida et al.,[27] the prevalence of tooth loss (83.5%) was much higher. Likewise, the average number of missing teeth (13.8) found in a community-based study conducted by Dye et al.[28] was also much higher. The WHO treatment goal for oral health as it relates to edentulism is the retention of not less than 20 functional teeth throughout life without recourse to prosthesis.[29] No case of complete edentulism was encountered in this study. Previous publications suggest that more people are retaining their teeth till old age.[30]
CONCLUSION
Although about one-third of the participants had dental caries, multiple teeth tend to be involved among those afflicted with the disease and only a quarter of this had received restorative care. Furthermore, most of the respondents had fair and poor oral hygiene, which suggests the need to educate and motivate the community toward adopting and maintaining positive oral health attitudes and practices to prevent tooth loss.
Footnotes
Source of Support: No support in the form of grant was received for this study
Conflict of Interest: No conflict of interest between the authors.
REFERENCES
- 1.Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;22:3–8. [PubMed] [Google Scholar]
- 2.Naito M, Yuasa H, Nomura Y, Nakayama T, Hamajima N, Hanada N. Oral health status and health-related quality of life: A systemic review. J Oral Sci. 2006;48:1–7. doi: 10.2334/josnusd.48.1. [DOI] [PubMed] [Google Scholar]
- 3.Patro BK, Ravi Kumar B, Goswami A, Mathur VP, Nongkynrih B. Prevalence of dental caries among adults and elderly in an urban resettlement colony of New Delhi. Indian J Dent Res. 2008;19:95–8. doi: 10.4103/0970-9290.40460. [DOI] [PubMed] [Google Scholar]
- 4.Thorpe S. Oral health issues in the African region: Current situation and future perspectives. J Dent Educ. 2006;70(Suppl 1):8–15. [Google Scholar]
- 5.Omitola OG, Arigbede AO. Prevalence of dental caries among adult patients attending a tertiary dental institution in south-south region of Nigeria. Port Harcourt Med J. 2012;6:52–8. [Google Scholar]
- 6.Urzua I, Mendoza C, Arteaga O, Rodríguez G, Cabello R, Faleiros S, et al. Dental caries prevalence and tooth loss in Chilean adult population: First national dental examination survey. Int J Dent 2012. 2012 doi: 10.1155/2012/810170. 810170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marthaler TM. Changes in dental caries 1953-2003. Caries Res. 2004;38:173–81. doi: 10.1159/000077752. [DOI] [PubMed] [Google Scholar]
- 8.Agbelusi GA, Jeboda SO. Oral health status of 12-year-old Nigerian children. West Afr J Med. 2006;25:195–8. doi: 10.4314/wajm.v25i3.28277. [DOI] [PubMed] [Google Scholar]
- 9.Lewis DW, Ismail AI. Periodic health examination, 1995 update: 2. Prevention of dental caries. The Canadian Task Force on the Periodic Health Examination. CMAJ. 1995;152:836–46. [PMC free article] [PubMed] [Google Scholar]
- 10.Touger-Decker R, van Loveren C. Sugars and dental caries. Am J Clin Nutr. 2003;78:881S–92S. doi: 10.1093/ajcn/78.4.881S. [DOI] [PubMed] [Google Scholar]
- 11.Nguyen TC, Witter DJ, Bronkhorst EM, Truong NB, Creugers NH. Oral health status of adults in Southern Vietnam-a cross-sectional epidemiological study. BMC Oral Health. 2010;10:2. doi: 10.1186/1472-6831-10-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Arigbede AO, Omitola OG, Gbuje DC. Pattern of restorative dental care in the dental clinic of University of Port Harcourt Teaching Hospital. Nig Qt J Hosp Med. 2011;21:236–40. [Google Scholar]
- 13.Petersen PE. Priorities for research for oral health in the 21st century--the approach of the WHO Global Oral Health Programme. Community Dent Health. 2005;22:71–4. [PubMed] [Google Scholar]
- 14.Oral Health Surveys Basic Methods. 5th ed. Geneva: WHO; 2013. World Health Organization; pp. 42–7. [Google Scholar]
- 15.Denloye O, Ajayi D, Bankole O. A study of dental caries prevalence in 12-14 year old school children in Ibadan, Nigeria. Pediatr Dent J. 2005;15:147–51. [Google Scholar]
- 16.Greene JC, Vermillion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13. doi: 10.14219/jada.archive.1964.0034. [DOI] [PubMed] [Google Scholar]
- 17.Adeyemo WL, Oderinu HO, Oluseye SB, Taiwo OA, Akinwande JA. Indications for extraction of permanent teeth in a Nigerian teaching hospital: A 16-year follow-up study. Nig Q J Hosp Med. 2008;18:128–32. doi: 10.4314/nqjhm.v18i3.45013. [DOI] [PubMed] [Google Scholar]
- 18.Gbenga Omitola O, Olabisi Arigbede A. Prevalence and pattern of pain presentation among patients attending a tertiary dental center in a Southern Region of Nigeria. J Dent Res Dent Clin Dent Prospect. 2010;4:42–6. doi: 10.5681/joddd.2010.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sogi G, Bhaskar DJ. Dental caries and oral hygiene status of 13-14 year old school children of Davangere. J Indian Soc Pedo Prev Dent. 2001;19:113–7. [PubMed] [Google Scholar]
- 20.Maru AM, Narendran S. Epidemiology of dental caries among adults in a rural area in Indian. J Contemp Dent Pract. 2012;13:382–8. doi: 10.5005/jp-journals-10024-1155. [DOI] [PubMed] [Google Scholar]
- 21.Khalifa N, Allen PF, Abu-bakr NH, Abdel-Rahaman ME, Abdelghafar KO. A survey of oral health in a Sudanese population. BMC Oral Health. 2012;12:5. doi: 10.1186/1472-6831-12-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Umesi-Koleoso DC, Ayanbadejo PO, Oremosu OA. Dental caries trend among adolescents in Lagos, South-West Nigeria. West Afr J Med. 2007;26:201–5. doi: 10.4314/wajm.v26i3.28309. [DOI] [PubMed] [Google Scholar]
- 23.Okoye L, Ekwueme O. Prevalence of dental caries in a Nigerian rural community: A preliminary local survey. Ann Med Health Sci Res. 2011;1:187–95. [PMC free article] [PubMed] [Google Scholar]
- 24.Barrow SY, Xionan X, LeGeros AR, Mijares DQ, LeGeros RZ, Galvis DL, et al. Dental caries prevalence among a sample of African American adults in New York city. (viii-ix).Dent Clin North Am. 2003;47:57–65. doi: 10.1016/s0011-8532(02)00054-x. [DOI] [PubMed] [Google Scholar]
- 25.Hopcraft MS, Morgan MV. Pattern of dental caries experience on tooth surfaces in an adult population. Community Dent Oral Epidemiol. 2006;34:174–83. doi: 10.1111/j.1600-0528.2006.00270.x. [DOI] [PubMed] [Google Scholar]
- 26.Splieth CH, Schwahn CH, Bernhardt O, Kocher T, Born G, John U, et al. Caries prevalence in an adult population: Results of the study of health in Pomerania, Germany (SHIP) Oral Health Prev Dent. 2003;1:149–55. [PubMed] [Google Scholar]
- 27.Kida IA, Astrøm AN, Strand GV, Masalu JR. Clinical and socio-behavioral correlates of tooth loss: A study of older adults in Tanzania. BMC Oral Health. 2006;6:5. doi: 10.1186/1472-6831-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dye BA, Wang R, Lashley R, Wei W, Abnet CC, Wang G, et al. Using NHANES oral health examination protocols as part of an esophageal cancer screening study conducted in a high-risk region of China. BMC Oral Health. 2007;7:10. doi: 10.1186/1472-6831-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Geneva: WHO; 1992. World Health Organization. Recent Advances in Oral Health; pp. 16–7. [Google Scholar]
- 30.Taiwo JO, Omokhodion F. Pattern of tooth loss in an elderly population from Ibadan, Nigeria. Gerodontology. 2006;23:117–22. doi: 10.1111/j.1741-2358.2006.00107.x. [DOI] [PubMed] [Google Scholar]