

Abstract
Objectives:
Facial esthetics is an important part of the orthodontic treatment. Many cases frequently require premolar extraction, either for relief of crowding or for profile change. Supposedly, extraction provides some vertical reduction. This investigation challenges the clinical effects of such treatment protocols.
Patients and Methods:
This was a retrospective and quasi-experimental study. Records of 60 patients in their post-pubertal age were randomly selected for this study. The criteria for case selection were: Class II Division I malocclusion with either two upper or four upper and lower first premolars extraction. Patients were not vertical-sensitive type of face. Pre- and post-treatment X-rays were scanned and digitized with Dolphin V 10.0 software. The X-rays of both groups were compared based upon the following cephalometric measurements: Lower anterior facial height (LAFH), Me–PP, Pal-MeGe, LAFH/total anterior facial height (TAFH) × 100, upper anterior facial height (UAFH)/TAFH × 100, U6 to PP, L6 to MP, and U6D–PTV.
Results:
In the four bicuspid group, a statistically significant increase was observed in all measurements: 2.53 mm increase in LAFH (P ≤ 0.04), 2.92 mm increase in Me–PP (P ≤ 0.01), 0.65° increase in Pal-MeGe (P ≤ 0.02), 0.66° increase in LAFH/TAFH × 100 (P ≤ 0.01), 1.26 mm increase in U6 to PP (P ≤ 0.02), 1.96 mm increase in L6 to MP (P ≤ 0.002), and 3.06 mm increase in U6D–PTV (P ≤ 0.0001). But a decrease of 0.66° in UAFH/TAFH × 100 (P ≤ 0.01) was observed. In the two bicuspid group, a significant increase was generally recorded: 2.06 mm increase in LAFH (P ≤ 0.05), 1.19° increase in Pal-MeGe (P ≤ 0.02), 1.39 mm increase in L6 to MP (P ≤ 0.002), and 2.37 mm increase in U6D–PTV (P ≤ 0.004).
Conclusions:
The results of this study are indicative of no change in patient's facial height with bicuspid extraction. In fact, extrusive effect of all types of tooth movement mostly overcomes the benefits of “wedging effect concept.”
Keywords: Biomechanics, Class II malocclusion, facial height, facial profile, premolar extraction
INTRODUCTION
Profile has the key role for establishment of facial esthetics in the process of orthodontic treatment planning. The anterior and posterior facial heights define the facial balance. In patients with normal growth pattern, the posterior facial height is more developed than the anterior one.[1,2,3,4,5] This facial dimension would also define the changes in the direction of mandibular rotation. Finally, it should be reminded that soft tissue status is another key factor for treatment planning.
The decision for extraction in orthodontics is a challenging one, especially for borderline cases. Clinicians would recommend premolar extraction for patients with steep mandibular plane, increased facial height, and even with minor dentoskeletal discrepancies. The philosophy behind this treatment protocol is that the extractions would provide forward and upward movement of molar teeth. Accordingly, the counterclockwise rotation of the mandible would reduce the facial height of the patient.[6,7] There are opinions that state the extractions are harmful to temporomandibular joints.[8,9,10,11,12] Nonetheless, it remains a valid question whether crowding of dental arch can be resolved otherwise. However, there are some other studies that show premolar extraction would not improve facial height of the patient.[13,14,15,16,17,18,19,20]
Considering the controversial results of various studies on the effect of premolar extraction on facial height of patients, this study was designed to compare the outcome of such extraction cases when performed either in both arches or in maxillary arch in Class II Division I non-growing patients.
PATIENTS AND METHODS
This retrospective, quasi-experimental study was performed on 60 Class II Division I non-growing patients who had referred to the postdoctoral orthodontic clinic of the School of Dentistry. All patient records were retrieved from the digitally retained archive of the clinic. The cephlometric X-rays were with the quality of 300 dpi resolution. Cases were matched in two equal groups of 30 patients each with either four upper bicuspid extractions (group 1) or two upper bicuspid extractions (group 2). Both groups consisted of equal gender distribution. Other case selection criteria were the following: Normal vertical growth pattern (SN-GoGn angle), neither headgear nor functional appliances were used for treatment, and all cases were treated with edgewise mechanics. Post-growth stage was diagnosed according to cervical vertebral maturation-modified radiographic evaluation.[21] Patients had mild to moderate excess overjet with no facial imbalance.
The cephalometric landmarks were registered using Dolphin V 10.0 (Dolphin, California, USA) [Figure 1]. A single examiner was calibrated for cephalometric measurements. Thus, there was no need to use Kappa test agreement to calculate the inter-examiner precision value for the reliability of the study. The angular measurements were saved in separate files for individual patients. The registered 18 measurements comprised the following: SNA, SNB, ANB, Y-axis (SN-Gn), SN-GoGn, PP-MeGo, and SN-MeGo angles, Me–PP distance, posterior facial height (PFH), total anterior facial height (TAFH) (N–Me distance), upper anterior facial height (UAFH) (N–ANS distance), lower anterior facial height (LAFH) (ANS–Me distance), U6 to palatal plane, L6 to mandibular plane, LAFH/TAFH × 100, UAFH/LAFH × 100, PFH/TAFH × 100, and U6D–PTV distance. The values were the average measurements for each variable measured by an orthodontist twice. To reduce the measurement errors, 10 patient records were randomly selected for thorough evaluations after final procedures. For the reliability of procedures, the α-Cronbach test was used for evaluation.
Figure 1.
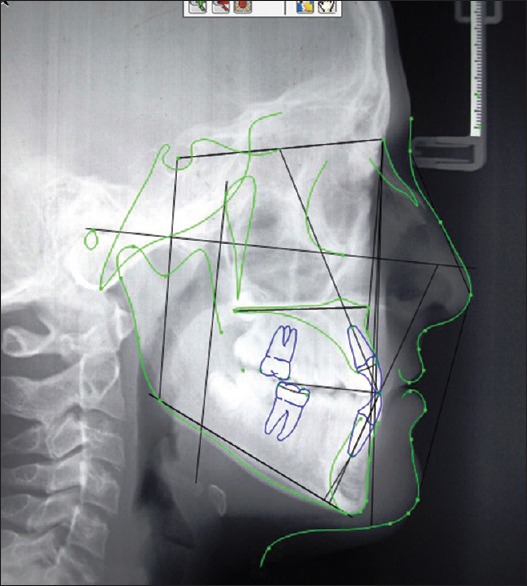
The cephalometric landmarks and lines registered on the Dolphin V 10.0 software are depicted on the lateral cephalogram
There were two sets of data for each case based upon the initial and final cephalometric measurements. The data was analyzed with paired t-test using the SPSS 18 software. The central distribution of variables was also calculated for further evaluation.
RESULTS
All variables were evaluated for both groups.
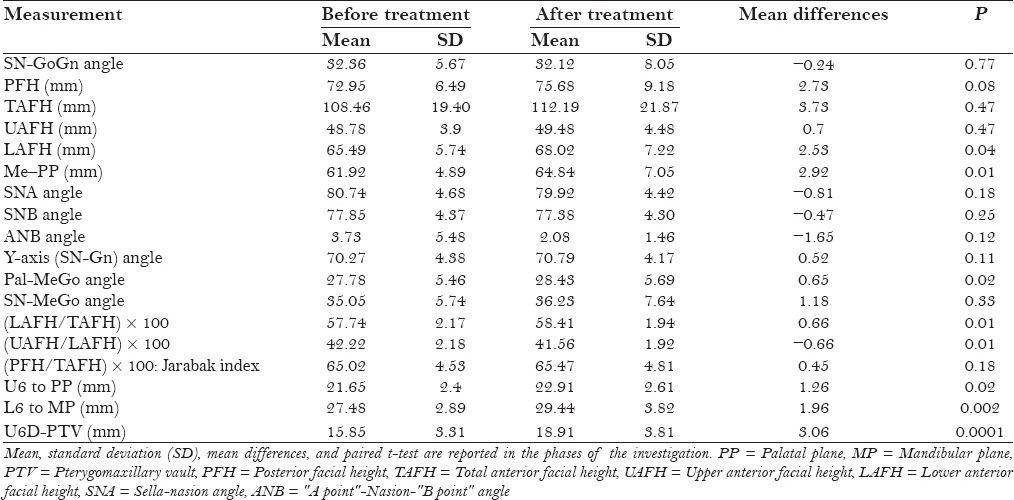
In group 1 (the four bicuspids extraction subjects), there were some statistically significant changes after treatment. The results of linear variables were as follows: LAFH increased to 2.53 mm (P = 0.04), the Me–PP increased to 2.92 mm (P = 0.01), the L6 to MP increased to 1.96 mm (P = 0.002), the U6D–PTV increased to 3.06 mm (P = 0.0001), and the dentoalveolar variable of U6 to PP increased to 1.26 mm (P = 0.02). The angular variable Pal-MeGo also increased to 0.65° (P = 0.02). The proportional ratio for LAFH/TAFH × 100 increased to 0.66 (P = 0.01), but the UAFH/LAFH × 100 ratio decreased to −0.66 (P = 0.01). The mean and SD of all cephalometric measurements for group 1 before and after treatment are presented in Table 1.
Table 1.
Eighteen cephalometric values (before and after treatment) selected in the four first premolar extraction group
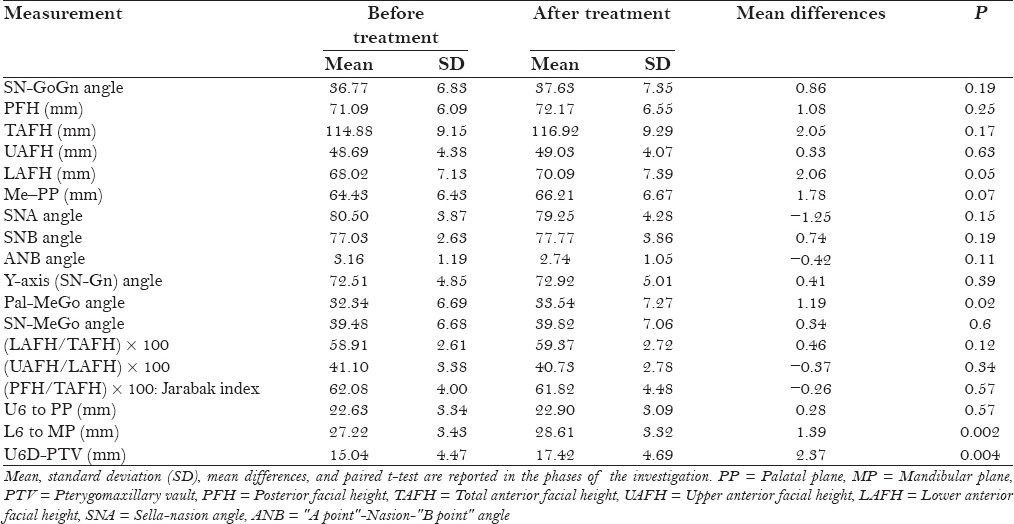
In group 2 (the two bicuspids extraction subjects), the results are as follows. The linear changes consisted of: LAFH increased to 2.06 mm (P = 0.05), the U6D–PTV had an increase of 2.37 mm (P = 0.004), and the L6 to MP increased to 1.39 mm (P = 0.002). The angular measurement of Pal-MeGo also increased to 1.19° (P = 0.02). The mean and SD of all cephalometric landmarks for group 1 before and after treatment are presented in Table 2.
Table 2.
Eighteen cephalometric values (before and after treatment) selected in the upper two first premolar extraction group
DISCUSSION
This study compared 18 linear, angular, and proportional variables of two groups of 30 subjects each (two and four bicuspids extraction, respectively) at two stages of before and after treatment. It was found that the four bicuspid cases showed more changes (8 variables) than the two bicuspid cases (4 variables) [Tables 1 and 2]. However, the LAFH, Pal-MeGo, L6 to MP, and U6D–PTV indices increased significantly in both groups. Furthermore, in group 1, there was an increase in variables (LAFH/TAFH) × 100, Me–PP, and U6 to PP and a decrease in the variable (UAFH/LAFH) × 100.
Conventionally, premolar extraction is aimed to resolve the tooth size arch size discrepancy, to permit correction of axial inclination of anterior teeth, or to reduce vertical height of the face. According to the results of this study, the bicuspid extraction philosophy (neither four bicuspid nor two bicuspid extraction) for facial height reduction does not provide any statistically significant changes for patients after treatment. Unexpectedly, lower anterior facial height and the angular measurement of palatal plane to mandibular plane increased in both groups. This is also emphasized by Staggers.[16] The biomechanical reason for this can be the inherent extrusive effect of most orthodontic tooth movement modalities, i.e. molar protraction, which can be adversely compensative to the facial height reduction.
There are some studies that focused on cephalometric angular measurements in premolar extraction cases. Bishara et al.[12] reported a significant decrease in SNA angle on comparing four bicuspid extraction cases with non-extraction control subjects. Their study cases were treated with headgear, as well. Another study did not find a significant change in SNB angle after treatment.[22] In fact, their cases showed slight increase in SNB during the post-retention period, perhaps due to the late mandibular growth phenomenon.
An obvious facial height reduction is proved to occur only in high-pull headgear treatment protocols and in the incisor retraction mechanics, following premolar extraction.[14,23] However, the present study did not show any significant changes in sagittal angular measurements, since no adjunctive appliance therapy was included in the treatment plan. Clearly, there was some decrease in SNA, SNB, and ANB angles, but the decrease was not significant statistically (P values of 0.15, 0.19, and 0.11, respectively). In other words, the extrusive consequence of molar protraction was not compensated with extraoral appliances. Finally, it should be noted that using functional appliances and cervical headgear (as opposed to high-pull) will increase the facial height in vertical-sensitive patients.[24]
A study by Cusimano et al.[25] indicated that premolar extraction does not result in decreasing the facial height. In fact, it indicated that the facial height slightly increased in patients with high mandibular plane angle. Interestingly enough, according to other studies, extraction of second molar could not benefit patients with long face, either.[16,26]
The variable of U6D–PTV increased significantly in both groups of upper premolars and upper and lower premolars extraction (P = 0.004 and 0.0001, respectively). This is due to the fact that even in the maximum anchorage condition, mesial movement of molars can certainly occur.[12] Obviously, in the condition of extraoral anchorage methods, the result would be reversed because of distal movement of molars.
Growth pattern of the lower jaw can definitely have a positive effect on the facial height in growing patients.[16,27] For this reason, this study excluded all growing cases from the samples. Samples of this study were in the post-growth spurt age based upon the cervical vertebral maturation (CVM) modified method – the age of 15 years and older – and had normal vertical growth pattern.
The change in the linear variable of TAFH was not statistically significant (P value in U4s group = 0.17 and in U and L4s group = 0.47). However, the LAFH variable increased significantly with treatment (P value in group 1 = 0.05 and in group 2 = 0.05). Taner-Sarisoy and Darendeliler[14] noticed that premolar extraction does not significantly change the facial height in the cases treated with fixed appliances, even in growing patients. According to Al-Nimri's study,[17] even second premolar extraction does not provide statistically significant changes in the facial height of treated patients.
The results of this study showed that all linear measurements increased with treatment. However, among all variables, LAFH, Me–PP, U6 to PP, L6 to MP, and U6D–PTV in four bicuspids extraction group and LAFH, L6 to MP, and U6D to PTV in upper bicuspids extraction group increased significantly. Other studies indicated that all linear measurements increased with premolar extractions,[15,16,20] whereas one study showed that these changes were not statistically significant.[19]
The angular measurements of this study indicated that only the Pal-MeGo angle increased in both groups (P = 0.02). Concerning the proportional values, the variables (LAFH/TAFH) × 100 and (UAFH/LAFH) × 100 changed significantly in group 1 (P = 0.01). In the studies by Kocadereli,[15] Chua,[19] and Kim,[20] none of the proportional value changes was significant.
The values indicative of rotational changes of mandible, such as SN-GoGn and Y-axis, of the present study were little and insignificant. Clearly, in cases treated with headgear, these values will increase significantly.[22] Finally, it should be emphasized that the case selection criteria for such studies, i.e. non-growing patients, unique mechanotherapy, type of malocclusion, play a key role in achieving a clear result at the end of treatment.
CONCLUSIONS
The results of the present study reveal that premolar extraction cannot be a primary goal of treatment for profile reduction. In addition, the number of premolars extracted (U and L or U only) does not provide any advantage for facial height changes. Perhaps, the extrusive effect of all types of tooth movement may disperse the benefit of bite-closing effect of molar and/premolar protraction mechanics.
ACKNOWLEDGMENTS
Dr. M. Mahdi Zafarmand was a senior dental student at the time of this study at Shahid Beheshti University of Medical Sciences School of Dentistry (Int. Branch). This research is registered as a doctoral thesis in partial fulfillment of the requirement for graduation in dentistry at Shahid Beheshti University of Medical Sciences School of Dentistry (Int. Branch) at the Office of Research Affairs under the No. 2787.
Footnotes
Source of Support: Nil
Conflict of Interest: The authors of the above article have no conflict of interest in this publication.
REFERENCES
- 1.Baum AT. A cephalometric evaluation of the normal skeletal and dental pattern of children with excellent occlusions. Angle Orthod. 1951;21:96–103. doi: 10.1043/0003-3219(1951)021<0096:ACEOTN>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Downs WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod. 1948;34:812–40. doi: 10.1016/0002-9416(48)90015-3. [DOI] [PubMed] [Google Scholar]
- 3.Hellman M. Preliminary study in the development of the human face. Dent Cosmos. 1927;69:250–69. [Google Scholar]
- 4.Janson GR. Bauru, São Paulo, Brazil: Universidade de São Paulo; 1990. Longitudinal and Comparative Study of Facial Growth-from 13 to 18 years old-in Young White Brazilian, Utilizing McNamara Jr's Cephalometric Analysis; p. 138. thesis. [Google Scholar]
- 5.Martins DR, Janson G, Almeida RR, Pinzan A, Henriques JF, Freitas MR. São Paulo, Brazil: Editora Santos; 1998. Atlas de crescimento craniofacial. thesis. [Google Scholar]
- 6.Fields HW, Proffit WR, Nixon WL, Phillip C, Stanek E. Facial pattern differences in long-faced children and adults. Am J Orthod. 1984;85:217–23. doi: 10.1016/0002-9416(84)90061-7. [DOI] [PubMed] [Google Scholar]
- 7.Pearson LE. Vertical control in treatment of patients having backward-rotational growth tendencies. Angle Orthod. 1978;48:132–40. doi: 10.1043/0003-3219(1978)048<0132:VCITOP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Schudy FF. The control of vertical overbite in clinical orthodontics. Angle Orthod. 1968;38:19–39. doi: 10.1043/0003-3219(1968)038<0019:TCOVOI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Looi LK, Mills JR. The effect of two contrasting forms of orthodontic treatment on the facial profile. Am J Orthod. 1986;89:507–17. doi: 10.1016/0002-9416(86)90009-6. [DOI] [PubMed] [Google Scholar]
- 10.Persson M, Persson EC, Skagius S. Long-term spontaneous changes following removal of all first premolars in Class I cases with crowding. Eur J Orthod. 1989;11:271–82. doi: 10.1093/oxfordjournals.ejo.a035995. [DOI] [PubMed] [Google Scholar]
- 11.Klapper L, Navarro SF, Bowman D, Pawlowski B. The influence of extraction and nonextraction orthodontic treatment on brachyfacial and dolichofacial growth patterns. Am J Orthod Dentofacial Orthop. 1992;101:425–30. doi: 10.1016/0889-5406(92)70116-R. [DOI] [PubMed] [Google Scholar]
- 12.Bishara SE, Cummins DM, Jakobson JR, Zaher AR. Dentofacial and soft tissue changes in Class II, Division 1 cases treated with and without extractions. Am J Orthod Dentofacial Orthop. 1995;107:28–37. doi: 10.1016/s0889-5406(95)70154-0. [DOI] [PubMed] [Google Scholar]
- 13.Hayasaki SM, Castanha Menriques JF, Janson G, de Freitas MR. Influence of extraction and nonextraction orthodontic treatment in Japanese-Brazilians with class I and class II division 1 malocclusion. Am J Orthod Dentefacial Orthop. 2005;127:30–6. doi: 10.1016/j.ajodo.2003.10.043. [DOI] [PubMed] [Google Scholar]
- 14.Taner-Sarisoy L, Darendeliler N. The influence of extraction orthodontic treatment on craniofacial structures: Evaluation according to two different factors. Am J Orthod Dentofacial Orthop. 1999;115:508–14. doi: 10.1016/s0889-5406(99)70272-6. [DOI] [PubMed] [Google Scholar]
- 15.Kocadereli I. The effect of first premolar extraction on vertical dimension. Am J Orthod Dentofacial Orthop. 1999;116:41–5. doi: 10.1016/s0889-5406(99)70301-x. [DOI] [PubMed] [Google Scholar]
- 16.Staggers JA. Vertical changes following first premolar extraction. Am J Orthod Dentofacial Orthop. 1994;105:19–24. doi: 10.1016/S0889-5406(94)70095-8. [DOI] [PubMed] [Google Scholar]
- 17.Al-Nimri KS. Vertical changes in class II division 1 malocclusion after premolar extraction. Angle Orthod. 2006;76:52–8. doi: 10.1043/0003-3219(2006)076[0052:VCICID]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Basciftci FA, Usumez S. Effects of extraction and nonextraction treatment on class I and class II subjects. Angle Orthod. 2003;73:36–42. doi: 10.1043/0003-3219(2003)073<0036:EOEANT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 19.Chua AL, Lim JY, Lubit EC. The effects of extraction versus nonextraction orthodontic treatment on the growth of the lower anterior face height. Am J Orthod Dentofacial Orthop. 1993;104:361–8. doi: 10.1016/S0889-5406(05)81334-4. [DOI] [PubMed] [Google Scholar]
- 20.Kim TK, Kim JT, Mah J, Yang WS, Baek SH. First or second premolar extraction effects on facial vertical dimension. Angle Orthod. 2005;75:177–82. doi: 10.1043/0003-3219(2005)075<0173:FOSPEE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Baccetti T, Franchi L, McNamara JA., Jr The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119–29. [Google Scholar]
- 22.Ciger S, Aksu M, Germeç D. Evaluation of post treatment changes in class II Division 1 patients after nonextraction orthodontic treatment: Cephalometric and model analysis. Am J Orthod Dentofacial Orthop. 2005;127:219–23. doi: 10.1016/j.ajodo.2004.08.015. [DOI] [PubMed] [Google Scholar]
- 23.Yamaguchi K, Nanda RS. The effects of extraction and nonextraction treatment on the mandibular position. Am J Orthod Dentofacial Orthop. 1991;100:443–52. doi: 10.1016/0889-5406(91)70084-A. [DOI] [PubMed] [Google Scholar]
- 24.Nanda SK. Patterns of vertical growth in the face. Am J Orthod Dentofacial Orthop. 1998;93:103–16. doi: 10.1016/0889-5406(88)90287-9. [DOI] [PubMed] [Google Scholar]
- 25.Cusimano C, McLaughlin RP, Zernik JH. Effects of first bicuspid extractions on facial height in high-angle cases. J Clin Orthod. 1993;27:594–8. [PubMed] [Google Scholar]
- 26.Bishara SE, Cummins DM, Zaher AR. Treatment and post treatment changes in patients with class II, Division 1 malocclusion after extraction and nonextraction treatment. Am J Orthod Dentofacial Orthop. 1997;111:18–27. doi: 10.1016/s0889-5406(97)70297-x. [DOI] [PubMed] [Google Scholar]
- 27.Rothstein T, Phan XL. Dental and facial skeletal characteristics and growth of females and males with class II division 1 malocclusion between the ages of 10 and 14 (revisited). Part II. Anteroposterior and vertical circumpubertal growth. Am J Orthod Dentofacial Orthop. 2001;120:542–55. doi: 10.1067/mod.2001.118628. [DOI] [PubMed] [Google Scholar]