

Abstract
The development of a web-based parent-focused intervention to improve parental awareness and monitoring of adolescent alcohol use was preliminarily evaluated. Upon completion of baseline assessment, sixty-seven parents were randomly assigned to the experimental web-based parent-focused intervention or an assessment only control condition. Participants who completed the experimental program, relative to control participants, significantly improved knowledge of problems related to underage drinking (p < .01) while improvements in overall monitoring of their children approached significance (p = .08). Improvements in monitoring by experimental participants, relative to controls, were pronounced in phone monitoring (p < .01) and indirect monitoring (p = .05). Participants in this study improved their communication about alcohol from pre- to post-intervention regardless of intervention. There were no statistical between group differences found regarding underage drinking attitudes. This pilot evaluation demonstrates that this program warrants further examination in controlled trials with greater power. Study implications are discussed in light of results.
Keywords: alcohol, adolescent, web-based program, monitoring
Underage alcohol use contributes to negative consequences that affect a vast proportion of young people in the United States, impeding physical, psychological, and social development. The trajectory of alcohol misuse by youth has been shown to increase with each advancing year of age (Substance Abuse and Mental Health Services Administration, 2009). Indeed, thirty percent of all students have consumed alcohol by the time they reach the 8th grade, and 12% of 8th grade, 30% of 10th grade and 44% of 12th grade students report drinking to intoxication during the past year (Johnston et al., 2011).
A recent review of preventative interventions identified several school-based programs as “most promising” for reducing or delaying adolescent alcohol use (Spoth et al., 2008). Common elements of these promising programs include parent involvement and training. These programs provide education to parents about the risk factors that promote underage drinking, instruction on strategies for reducing adolescent substance use, and opportunities to build communication skills with their children through practice assignments (Catalano et al, 2003; Komro et al., 2004; Spoth et al., 2001). Other important components of these interventions include communicating expectations, and having clearly defined family rules against adolescent alcohol use (Guo, Hawkins, Hill, & Abbott, 2001; Spoth et al., 2008). Promising programs often provide information and strategies that are relevant to monitoring the activities of teenagers (Fulkerson, Pasch, Perry, & Komro, 2008; Ryan, Jorm, & Lubman, 2010; Ryan, Jorm, Kelly, Hart, Morgan, & Lubman, 2011).
Although positive results have emerged from these school-based programs, recruitment and retention of parents in these programs are often problematic (Beatty & Cross, 2006; Spoth et al., 1998; Williams et al., 1995). Perceived time commitment, scheduling conflicts, issues related to family privacy, and social stigma are among factors that contribute to poor rates of parent involvement. Health and transportation problems have also been cited as barriers to participation. For instance, some programs require weekly group attendance for up to 14 weeks (one to two hours in duration). Parents have been found to report that it is important to establish programming to assist them in communicating practically and effectively with their children about drug and alcohol use, and that these programs should, ideally, be implemented within their own home, be easy to use, time-efficient, and interactive (Beatty & Cross, 2006; Hahn et al, 1996; Mallick et al., 1998; Paxton et al., 1998).
To address the problem of parent retention and parents’ desire for time-efficient, easy-to- understand, interactive programming, a one-session web-based psychoeducational program, the iPAM (Increasing Parental Awareness and Monitoring), was developed. This 25-minute program disseminates evidence-based strategies via 3 brief modules using audio-visual media that is engaging, colorful, and interactive. The program highlights the importance of parental knowledge about underage alcohol use, models parent-child communication about alcohol related topics, and furnishes parents with a guide to effectively monitor their teen and assist them to decrease adolescent drinking.
In this study, we hypothesized that iPAM, relative to wait-list control, would increase parents’ knowledge about underage use of alcohol, increase the frequency of communication between parents and youth about issues related to underage alcohol use, increase parental monitoring of youth behaviors, and reduce permissive attitudes of parents about underage alcohol use. To assist in determining feasibility of iPAM, we evaluated parent satisfaction with regard to information conveyance, ease of use, organization, relevance, and visual appeal.
METHOD
Institutional Review Board approval was obtained. Recruitment was conducted within a large metropolitan area in the southeastern United States. Parents were recruited from 4 middle and 4 high schools through mailed advertisements and online parent listservs that contained a web address/link and that stated: As part of a current research study, we are asking that you complete a brief survey and participate in a program that could help parents connect with teens and communicate expectations about health-related behaviors. You will be eligible to receive 2 adult admission movie theater tickets for this opportunity to learn important information. To participate, you must be a parent or guardian of a middle or high school student.
Parents that visited the web-link arrived at a page with study information which indicated that research related activities were anonymous and that outlined the time investment for their participation. Parents were informed that they would be randomized into one of two groups. One group would complete a 45 to 60 minute intervention session (i.e., baseline assessment plus the experimental program; iPAM condition) initially and complete a 30 minute assessment 4 weeks later. The other group involved the completion of a 30 minute assessment initially and the 45–60 minute intervention session in four weeks (i.e., wait-list control condition). All parents were instructed to print or save this information prior to clicking the link containing baseline assessments. After completion of baseline assessment parents were randomized to either the experimental condition or the wait-list control condition. If assigned to iPAM, they were immediately launched into the program. Parents in the control condition were emailed the link to the iPAM program after completion of the post 4-week follow-up. A 15-item program satisfaction survey was completed by all parents in the experimental condition and by the control group parents that elected to engage in the program after completion of the second assessment.
At the conclusion of their initial engagement, all parents regardless of condition were asked to provide their email address and phone number so that they could be contacted in four weeks to complete the last assessment (i.e., post 4-week survey). Upon completion of the post 4-week survey measures, parents from both conditions were sent 2 adult movie passes for their participation in the research.
Participants
One hundred and fourteen parents were randomized to experimental conditions. However 31 parents did not provide contact information to be emailed the weblink to the post 4-week assessment, and were not included in the analyses. Of the parents that provided contact information, eight were inaccurate or inadequate to contact them, and eight did not respond to multiple emails or phone calls to complete the second assessment. Parents that failed to complete the second assessment due to inadequate or lack of contact information were distributed equally across conditions. Sixty-seven parents (iPAM = 33, Control = 34) completed baseline and post 4-week assessments and were included in the analyses. The sample demographics were 96% female and 91% Caucasian, and 57% reported an annual income greater than 70 thousand. Most parents were married and all but one identified as the biological parent.
Assessment Measures
Parent knowledge
A 36-item measure was created to assess parent knowledge about underage alcohol use. Items were derived from publications available on the National Institute of Alcohol Abuse and Alcoholism website (NIAAA; 2005, 2007), the Call to Action from the Office of the Surgeon General (United States Department of Health and Human Services, 2007), and state and local laws about underage alcohol use. Scores for parent knowledge could range from 0 to 36 with higher scores depicting greater knowledge. Item responses were true, false, and not sure/don’t know. Correct true or false items were summed to compute a total score (score of 0 was given to incorrect and not sure/don’t know responses). Representative items included: it is best to teach teens how to drink alcohol at home under supervision; alcohol consumed regularly by adolescents can impact brain development; over 80% of 10th-graders believe that alcohol is readily available for them to drink.
Parental monitoring
The Parental Monitoring Inventory (PMI; Cottrell, Branstetter, Cottrell, Harris, Rishel, & Stanton, 2007) was modified for use in this study. The PMI is a 27-item instrument that measures parental monitoring behavior and yields seven factor scores: Direct, Indirect, School, Health, Computer, Phone, and Restrictive Monitoring. The revised measure included four new items to account for the use of texting and cell phone use and two new items were relevant to indirect monitoring. Twelve items were altered to increase specificity and clarity. Survey items began with a standard prompt (i.e., in the past 4 weeks). Example questions were: how often have you talked with your teen about their plans for their free time; how often have you contacted the parents of your teen’s friends to talk with them about an activity that your teens are doing together; how often have you asked your teen for details once the planned activity is over? Responses were rated on a 4-point Likert-type scale (never, sometimes, usually, always) and were assigned scores of 0 through 3. Higher scores represented greater frequency of monitoring. Scores on the revised measure were found to have high internal reliability (α= .90).
Parent communication about alcohol
Two items were utilized, and the responses were summed to yield a total score measuring frequency of communication about alcohol use during the past 4 weeks. Parents were asked to provide 1) the number of times they communicated with their child about problems or negative consequences associated with alcohol use, and 2) number of times they talked with their teen about alcohol advertising or alcohol use in movies and television.
Parental attitude about underage alcohol use
Five selected items that comprise the Attitudes Toward Alcohol Use subscale of the Minnesota Community Readiness Survey were used to measure parents’ attitudes regarding underage use of alcohol (Beebe, Harrison, Sharma, & Hedger, 2001). Items began with a standard prompt (i.e., in my opinion). Example item stems included: it is acceptable for teenagers under the age of 18 to drink alcohol at parties if they don’t get drunk; it is acceptable for teenagers under the age of 18 to drink as long as they don’t drive afterward; it’s okay for parents to offer their children under the age of 21, alcoholic drinks in their own home. Item responses were rated on a 4-point Likert-type scale (strongly agree = 1, somewhat agree = 2; somewhat disagree = 3, strongly disagree = 4).
Program satisfaction
Fifteen items were used to assess parent perceptions about the utility and appeal of the program, and these responses were rated on a 4-point Likert scale (strongly agree to strongly disagree). Items generally were related to visual appeal, whether or not the web links worked, whether the parent would visit the site again, or recommend it to other parents. Higher scores represented higher satisfaction (see Table 2).
Table 2.
iPAM program satisfaction survey
| n | Strongly Agree % | Agree % | Disagree % | Strongly Disagree % | |
|---|---|---|---|---|---|
| Module 1 Interactive Quiz was informative | 46 | 58.7 | 41.3 | 0.0 | 0.0 |
| Module 2 Real People, Real Strategies informative | 44 | 54.5 | 45.5 | 0.0 | 0.0 |
| Module 3 Parent Checklist was informative | 44 | 61.4 | 38.6 | 0.0 | 0.0 |
| The information from the links was helpful | 43 | 44.2 | 53.5 | 2.3 | 0.0 |
| Links on the website worked | 43 | 44.2 | 53.5 | 2.3 | 0.0 |
| The author has expertise in the area | 43 | 48.8 | 51.2 | 0.0 | 0.0 |
| The website is visually appealing | 43 | 46.5 | 51.2 | 2.3 | 0.0 |
| The pages were well organized | 42 | 45.2 | 52.4 | 2.4 | 0.0 |
| The website has a logical layout and sequence | 42 | 45.2 | 52.4 | 2.4 | 0.0 |
| The information appears accurate, well researched | 43 | 53.5 | 46.5 | 0.0 | 0.0 |
| The information was relevant to my family | 43 | 37.2 | 48.8 | 14.0 | 0.0 |
| The website was easy to use | 42 | 50.0 | 47.6 | 2.4 | 0.0 |
| The website was informative | 42 | 52.4 | 47.6 | 0.0 | 0.0 |
| I would visit this website again | 43 | 37.2 | 58.2 | 2.3 | 2.3 |
| I would recommend this website to other parents | 44 | 45.5 | 52.2 | 2.3 | 0.0 |
iPAM Intervention
The iPAM program comprises three modules that can be completed in approximately 20 to 30 minutes. The first module, Just the Facts, is an audio-visual interactive quiz that examines participant knowledge about underage alcohol use. Responses are immediately followed with feedback about the correctness of the response and additional information related to the respective fact. Questions and answers were presented in text and audio format and conveyed information about the prevalence and problems of underage alcohol use, parental influence to prevent underage alcohol use, and state laws related to underage alcohol use. A similar quiz format is used to inform teenagers about alcohol use in web-based preventive intervention sponsored by the NIAAA (www.thecoolspot.gov).
The second module, Real People, Real Strategies, provides modeling of parent-teen communication using digital audio-visual media. This module was designed to address parent concerns about how to talk about alcohol and other substance use with their children, and included additional factual information related to environmental influences, parental monitoring, adolescent access to alcohol, and positive communication (Beatty & Cross, 2006).
The last module, Parent Monitoring Checklist, provides parents with a single-page, informational guide with specific information about monitoring their teen. A printed checklist about how to monitor teenagers was a time-effective method to provide important information about specific monitoring behaviors that are associated with lower levels of alcohol use in adolescents (Fulkerson, Pasch, Perry, & Komro, 2008; Ryan, Jorm, Kelly, Hart, Morgan, & Lubman, 2011). Parents were instructed to read the checklist, and either print or save it to their computer desktop for easy access.
Assessment-only Control
The assessment-only control parents completed the same baseline and post 4-week assessments that were completed by the iPAM condition parents. After the post 4-week assessment was completed these parents were emailed a link to the iPAM program. No follow up data were collected to discover whether these parents followed the link to the program.
RESULTS
Baseline Differences
Multivariate analysis of variance (MANOVA) procedures compared the two conditions (iPAM, n = 33; wait-list control, n = 34) on baseline scores of parental knowledge, monitoring, frequency of communication, and attitude about underage alcohol use. No significant differences were observed for any of these variables (see Table 1 for means). Chi square analyses and t-tests comparing the two conditions on age, race, ethnicity and income also revealed no significant differences.
Table 1.
Group means and standard deviations at baseline and 4-week followup
|
iPAM n=33 |
Control n=34 |
|||
|---|---|---|---|---|
|
| ||||
| Baseline | Post 4-week follow up | Baseline | Post 4-week follow up | |
| M (SD) | M (SD) | M (SD) | M (SD) | |
| Knowledgeb*** | 25.42 (5.31) | 28.88 (4.68) | 26.35 (5.06) | 26.61 (6.08) |
| Total Monitoring | 47.58 (13.93) | 48.96 (13.04) | 52.26 (13.86) | 50.50 (13.97) |
| Monitoring Subscales: | ||||
| Direct | 7.79 (1.69) | 7.55 (1.20) | 7.94 (1.41) | 7.82 (1.44) |
| Indirect | 10.75 (5.65) | 11.79 (5.42) | 13.11 (6.14) | 12.05 (7.04) |
| School | 7.15 (2.84) | 7.39 (2.52) | 8.00 (2.01) | 8.26 (2.26) |
| Health | 7.30 (3.00) | 6.94 (2.97) | 7.70 (2.23) | 7.58 (2.66) |
| Phoneb** | 4.03 (2.39) | 4.73 (2.97) | 5.06 (3.32) | 4.41 (2.62) |
| Computer | 6.93 (2.79) | 7.03 (2.99) | 7.00 (3.52) | 6.70 (3.39) |
| Restrictive | 3.60 (2.17) | 3.57 (2.00) | 3.44 (2.03) | 3.58 (2.16) |
| Communicationa* | 2.42 (2.47) | 3.42 (3.03) | 1.91 (2.27) | 2.08 (2.62) |
| Attitude | 3.73 (.39) | 3.73 (.37) | 3.56 (.47) | 3.53 (.41) |
main effect of time;
interaction between group and time;
p<.05;
p< .01;
p<.001
Changes in Parent Knowledge, Monitoring, Communication, and Attitude
Changes from baseline to post-intervention in parental knowledge, monitoring, frequency of communication, and parental attitude about underage alcohol use were assessed using 2 (condition: iPAM and Control) × 2 (time: baseline and post 4-week) mixed model analyses of variance (ANOVA). Mean scores and results are reported in Table 1. A significant interaction between condition and time was observed for Knowledge, F(1, 65) = 14.56, p < .001, partial η2 = .183] indicating greater positive change among iPAM parents (see Figure 1).
Figure 1.
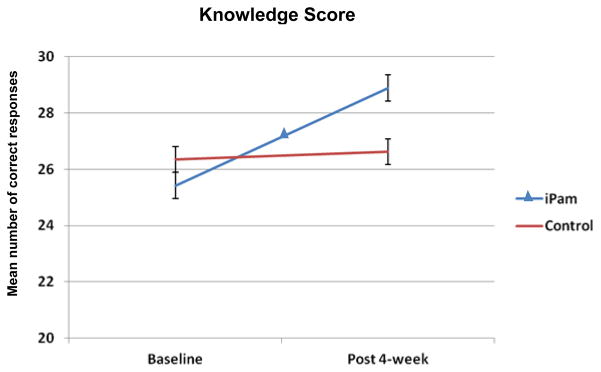
Mean knowledge scores by time and condition
A condition x time interaction effect for Total Monitoring approached significance [F(1, 65) = 3.09, p = .08, partial η2 = .183]. Although this interaction was non-significant, we conducted analyses involving the monitoring sub-scales to assist in determining areas worthy of future exploration. We view such analyses as exploratory given our lack of power and preliminary nature of this pilot study. Findings related to the monitoring subscales showed phone monitoring to be significant [F(1, 65) = 7.37, p < .01, partial η2 = .102] (see Figure 2) and the indirect monitoring subscales approached significance [F(1, 65) = 4.00, p = .05, partial η2 = .183].
Figure 2.

Mean phone monitoring scores by time and condition
A main effect of time was observed for Communication [F(1, 65) = 4.36, p = .04, partial η2 = .063], indicating that communication about the problems associated with underage alcohol use increased across the 4 weeks of assessment (Figure 3). No interaction effect was observed.
Figure 3.
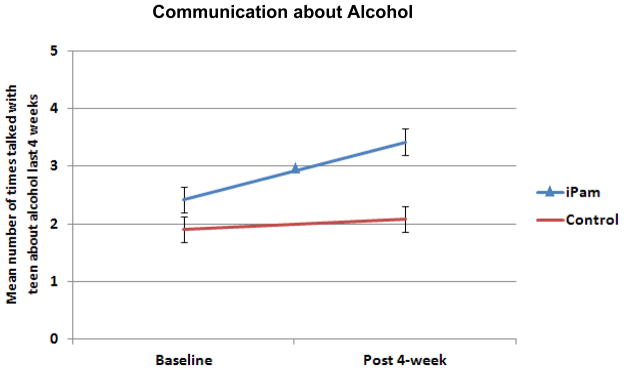
Mean frequency of communication by time and condition
No significant main or interaction effects were observed for changes in parental attitudes about underage alcohol use.
iPAM program satisfaction
Most parents agreed, or strongly agreed, they were satisfied with the various aspects of iPAM, reflecting that the program demonstrated visual appeal, organization, relevance, and utility (Table 2). Fourteen percent of the parents indicated that they disagreed the program was relevant to them.
DISCUSSION
Findings from this comparative study showed one-session of iPAM significantly increased parental knowledge about the prevalence and problems associated with underage drinking relative to a control condition. Parental monitoring changes in response to iPAM were also observed, albeit to a non-significant extent. Parent-teenager communication about problems related to underage alcohol use statistically improved regardless of treatment assignment. However, it should be mentioned that examination of mean differences between intervention conditions on this variable appeared to indicate most of this variance was attributed to improvements noted in iPAM participants. The parent scores related to attitudes about underage alcohol use were uniformly high at baseline and did not change over time. Parent evaluations of the iPAM were generally positive, as most parents agreed that they were satisfied with the program. Interestingly, 14% of the parents reported that they disagreed iPAM was relevant to their family, and 5% disagreed or strongly disagreed they would visit the iPAM site again. This finding suggests that iPAM may be irrelevant to a small percentage of families, and that in future studies iPAM may demonstrate greater improvements in target measures relative to other control conditions when participants are concerned with underage alcohol use. We believe these observations suggest iPAM may have promise as a mechanism for delivering effective parent-based prevention and intervention programs, and warrants further examination in controlled trials with greater power. Indeed, our results hint towards the utility and potential efficacy of developing a more extensive program.
Limitations and Future Directions
There are a number of limitations that need to be noted in this pilot study. First, the measures used to assess knowledge and monitoring were created or modified specifically for use in this project, and lack stringent psychometric testing. Of concern, for example, the monitoring measure may have lacked sensitivity to detect important monitoring changes over time (i.e., four point Likert-type scale resulted in a limited range of responses). Also, there appeared to be a ceiling effect in the measurement of parental attitudes about underage drinking, as baseline means in both conditions reflected highly non-permissive attitudes. Future investigations should utilize validated adolescent measures of alcohol use, attitudes about underage alcohol use, and access to alcohol.
The sampling strategy resulted in recruitment of a relatively small, homogeneous sample of parents who were predominantly female, Caucasian, and of mid- to high-socioeconomic status. Related to sampling, due to the relatively low number of participants the study lacked power to detect differential treatment condition effects. Recruitment of adequate sample sizes in future studies would permit examination of differential treatment condition effects and assist in understanding the influence of iPAM on other independent variables, such as gender and age of the teenagers. To encourage participation of a more diverse group of parents, recruitment and intervention sessions might be conducted at community centers and faith-based institutions where adequate technology (computer access) can be made available for parent use.
Acknowledgments
Our thanks and appreciation is extended to Carol Burkett, Director, Orange County Coalition for a Drug-Free Community and the Orange County Underage Drinking Task Force Implementation Committee, Orange County, Florida for providing partial funding for this project and to the Clinical and Translational Science Award (CTSA: 1UL1RR029884), and NIDA T32 (5T32DA022981) for postdoctoral support at the University of Arkansas for Medical Sciences.
References
- Beebe TJ, Harrison PA, Sharma A, Hedger S. The Community Readiness Survey: Development and initial validation. Evaluation Review. 2001;25(1):55–71. doi: 10.1177/0193841X0102500103. [DOI] [PubMed] [Google Scholar]
- Beatty SE, Cross DS. Investigating parental preferences regarding the development and implementation of a parent-directed drug-related educational intervention: An exploratory study. Drug and Alcohol Review. 2006;25(4):333–342. doi: 10.1080/09595230600741172. [DOI] [PubMed] [Google Scholar]
- Catalano RF, Mazza JJ, Harachi TW, Abbott RD, Haggerty KH, Fleming CB. Raising healthy children through enhancing social development in elementary school: Results after 1.5 years. Journal of School Psychology. 2003;41(2):143–164. [Google Scholar]
- Cottrell SA, Branstetter S, Cottrell L, Harris CV, Rishel C, Stanton BF. Development and validation of a parental monitoring instrument: Measuring how parents monitor adolescents’ activities and risk behaviors. The Family Journal. 2007;15(4):328–335. [Google Scholar]
- Fulkerson JA, Pasch KE, Perry CL, Komro K. Relationships between alcohol-related informal social control, parental monitoring and adolescent problem behaviors among racially diverse urban youth. Journal of Community Health. 2008;33(6):425–433. doi: 10.1007/s10900-008-9117-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo J, Hawkins JD, Hill KG, Abbott RD. Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. Journal of Studies on Alcohol. 2001;62(6):754–762. doi: 10.15288/jsa.2001.62.754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hahn E, Simpson M, Kidd P. Cues to parent involvement in drug prevention and school activities. Journal of School Health. 1996;66:165–170. doi: 10.1111/j.1746-1561.1996.tb06268.x. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national results on adolescent drug use: Overview of key findings, 2010. Ann Arbor: Institute for Social Research, The University of Michigan; 2011. p. 77. [Google Scholar]
- Komro KA, Perry CL, Veblen-Mortenson S, Bosma LM, Dudovitz BS, Williams CL, et al. Brief report: the adaptation of Project Northland for urban youth. Journal of Pediatric Psychology. 2004;29(6):457–66. doi: 10.1093/jpepsy/jsh049. [DOI] [PubMed] [Google Scholar]
- Mallick J, Evans R, Stein G. Parents and drug education: Parents’ concerns, attitudes, and needs. Drugs: Education, Prevention & Policy. 1998;5:169–176. [Google Scholar]
- National Institutes of Alcohol Abuse and Alcoholism. Alcohol and development in youth: A multidisciplinary overview. 2005;28(3) Retrieved May 2008 from http://pubs.niaaa.nih.gov/publications/arh283/toc28-3.htm. [PMC free article] [PubMed] [Google Scholar]
- National Institutes of Alcohol Abuse and Alcoholism. Make a difference: Talk to your child about alcohol. NIH Publication No 06-4314. 2007 Retrieved May 2008 from http://pubs.niaaa.nih.gov/publications/MakeADiff_HTML/makediff.htm#otherpubs.
- Paxton R, Finniga S, Haddow M, Allott R, Leonard R. Drug education in primary schools: putting what we know into practice. Health Education Journal. 1998;57:117–127. [Google Scholar]
- Ryan SM, Jorm AF, Kelly CM, Hart LM, Morgan AJ, Lubman DI. Parenting strategies for reducing adolescent alcohol use: A Delphi consensus study. BMC Public Health. 2011;6:11–13. doi: 10.1186/1471-2458-11-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan SM, Jorm AF, Lubman DI. Parenting factors associated with reduced adolescent alcohol use: a systematic review of longitudinal studies. Australian & New Zealand Journal of Psychiatry. 2010;9(44):774–783. doi: 10.1080/00048674.2010.501759. [DOI] [PubMed] [Google Scholar]
- Spoth R, Greenberg M, Turrisi R. Preventive interventions addressing underage drinking: State of the evidence and steps toward public health impact. Pediatrics. 2008;121:S311–S336. doi: 10.1542/peds.2007-2243E. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth R, Redmond C, Shin C. Direct and latent-variable parenting outcomes of two universal family-focused preventative interventions: Extending a public health oriented research base. Journal of Consulting and Clinical Psychology. 1998;66:385–399. doi: 10.1037//0022-006x.66.2.385. [DOI] [PubMed] [Google Scholar]
- Spoth R, Redmond C, Shin C. Randomized trial of brief family interventions for general populations: adolescent substance use outcomes four years following baseline. Journal of Consulting and Clinical Psychology. 2001;69(4):627–642. doi: 10.1037//0022-006x.69.4.627. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. NSDUH Series H-36, HHS Publication No SMA 09-4434. Office of Applied Studies; Rockville, MD: 2009. Results from the 2008 National Survey on Drug Use and Health: National Findings. [Google Scholar]
- United States Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2007. Retrieved May 2008 from http://www.surgeongeneral.gov/topics/underagedrinking/familyguide.pdf. [PubMed] [Google Scholar]
- Williams CL, Perry C, Dudovitz B, Veblen-Mortenson S, Anstine P, Komro KA, Toomey TL. A home-based prevention program for sixth-grade alcohol use: Results from Project Northland. The Journal of Primary Prevention. 1995;16:125–147. doi: 10.1007/BF02407336. [DOI] [PubMed] [Google Scholar]