

Abstract
Objectives
Little is known about whether the feeling of happiness follows the age-related decline in physical and mental functioning. The objective of this study was to analyze differences with age in physical and mental functions and in the feeling of happiness among Danes aged 45 years and older.
Method
Three Danish population-based surveys including 11,307 participants aged 45+ years, of whom 2411 were in the age group of 90+, were conducted in the period 1995–2001. The participation rate in the three surveys was between 63% and 82% and the same design and the same instrument were used. Self-reported mobility, a cognitive composite score, and a depression symptomatology score including a question about happiness were assessed. T-score metric was used to compare across domains and age groups.
Results
Overall, successively older age groups performed worse than the youngest age group (45–49 years), and the estimated linear decline was greater after age 70 than before age 70. For example, when comparing the oldest age group (90+ years) with the youngest, the T-score differences were found to be the largest for the mobility score (men: 40.2, women: 41.4), followed by the cognitive function (men: 22.0, women: 24.9), and the total depression symptomatology score (men: 15.5, women: 17.4). Conversely, the T-score difference in happiness was small (men: 5.6, women: 6.0).
Conclusion
Despite markedly poorer physical and mental functions with increasing age, in this Danish sample age did not seem to affect happiness to a similarly notable extent, although, in this study, cohort and age effects cannot be disentangled.
Keywords: happiness, cognitive composite score, depression symptomatology, mobility, aging
Introduction
The first International Day of Happiness was launched in 2013 as a result of 193 United Nations member states adopting a resolution for increasing human happiness and well-being (United Nations, 2013). The rationale for the actions leading up to this was a recognition that not only would the gross domestic product be a useful tool in future policy decisions but so would broader measures of progress. As a result, happiness was suggested to be a new measure of a society's success (Helliwell, Layard, & Sachs, 2012).
In contrast to what one would hypothesize, and although good physical and mental functions were important for happiness (Helliwell et al., 2012), the curve that described age-related differences in happiness was suggested to be U-shaped among individuals above 20 years of age (Blanchflower & Oswald, 2008). Based on a European sample, it was estimated that the minimum happiness occurred between 45 and 50 years of age for both males and females (Blanchflower & Oswald, 2008). However, other investigators have found that the happiness curve illustrated a range of forms including flat development, an inverted U-shape, or an approximation of a U-shape, until the late 60s followed by a decline in happiness (Easterlin, 2006; Frijters & Beatton, 2012; Gerstorf et al., 2010; Wunder, Wiencierz, Schwarze, & Kuchenhoff, 2013). In comparison, age-related differences in domains such as physical and mental functions very consistently take the form of a deteriorating curve which may well deteriorate at different speeds and even accelerate in the oldest old, but not forming a U-shaped curve (Andersen-Ranberg et al., 1999; Crimmins & Beltran-Sanchez, 2011; Frederiksen et al., 2006; McGue & Christensen, 2013; Stathokostas, Jacob-Johnson, Petrella, & Paterson, 2004).
In a study of older adults, 60 years and older, the lower level of happiness was associated with disability, which was identified by having serious difficulty with hearing, vision, cognition, functional ability, personal care, and instrumental activities of daily living (Freedman, Stafford, Schwarz, Conrad, & Cornman, 2012). Furthermore, in a study of 65-year-old men and women univariate relationships between happiness and disability (as measured by the World Health Organization Disability Assessment Schedule [WHO-DAS]), cognition and depression were found (Cooper, Bebbington, & Livingston, 2011). However, it remains unstudied whether the age-related development of happiness tracks with cognition, depression, and functional ability in the second half of life.
In a recent twin study using a cross-sectional design, age-related differences were observed in cognition and depression symptomatology (McGue & Christensen, 2013). However, the mobility function and happiness were not studied, and the sample size in the oldest age group was small. Thus, when comparing these domains across a large age range within the same country at the same calendar time, it is warranted to use the same instrument and to include a large numbers of oldest-old individuals. Therefore, in this study, we aimed to investigate age-related differences in self-reported mental and mobility functions and feeling of being happy among Danes aged 45 years or older.
Method
The sample consisted of the intake wave from multiple data-sets from three large Danish surveys: the Study of Middle-Aged Danish Twins (MADT), the Longitudinal Study of Aging Danish Twins (LSADT), and the Danish 1905-Cohort survey (C1905). The data collection of MADT was carried out in 1998 and comprised a large random sample of twins from the birth cohorts from 1931 through 1952 (Gaist et al., 2000; McGue & Christensen, 2013). Out of the total eligible sample of 5280 twins, 4314 (81.7%) participated. LSADT is a population-based twin study comprising all twins aged 70 years or older at the intake data collection, which was carried out in 1995, 1997, 1999, and 2001. In total, 4731 (72.3%) twins participated (Christensen, Holm, McGue, Corder, & Vaupel, 1999). C1905 is a population-based study that was carried out in 1998 and included all Danes born in 1905, of whom 2262 (62.8%) participated in the study (Nybo et al., 2001). Data were collected through in-person interview assessments of participants or proxy participants using similar standardized questionnaires and the same physical and cognitive tests in the three surveys. All surveys in this study have been planned by the same research group, by the same principal investigator, and carried out in a sequential manner with the same design and instrument. All three surveys were approved by the ethical committee system in Denmark (trial numbers MADT: S-VF-19980072; LSADT: S-VF-20040241; C1905: VF-20040240), and participants provided written informed consent. Furthermore, surveys were also registered at the Danish Data Protection Agency (journal numbers for MADT and LSADT: 2007-54-0227; C1905: 2010-41-5169).
The physical function was evaluated by the self-report of the ability to (1) walk 400 meters without resting, (2) manage stairs to the second floor, and (3) run 100 meters. For descriptive purpose, all items were dichotomized into able or unable. For comparison across ages and measures, these three items were recorded on an ordinal scale (range: 1–4 (best)), and the average of the three items was used as a general mobility score.
The cognitive function was evaluated by five brief tests: fluency (the number of animals named in 1 minute), digits forward (the number of correct responses out of a possible of 14 digits forward tasks), digits backward (the number of correct responses out of a possible of 14 digits backward tasks), immediate recall (the number of words recalled immediately out of a list of 12 words), and delayed recall (the number of recalled words from the list of 12 words after a delay of 10 minutes). These five test items were also used to compute a cognitive composite score (CCS) (McGue & Christensen, 2001) that was calculated by standardizing each single test to the mean and standard deviation (SD) of the values of the 45–49 year olds before summing them into the CCS (low score is poor performance).
Happiness was evaluated by the single-item question ‘Do you feel happy and satisfied with life at present?’ and the five possible answers were: (1) yes, always; (2) yes, most of the time; (3) yes, occasionally; (4) no, almost never; and (5) no, never. Answers (1) and (2) defined those who were happy and answers (3), (4), and (5) defined those who were unhappy. For comparison across measures, these answers were also analyzed using the recoded ordinal scale (range: 1–5 (best)). Single-item questions to capture happiness in study populations have been widely used and have proven able to detect age group differences (Cooper et al., 2011; Veenhoven, 2014).
Depression was evaluated by inclusion of the modified version of the 21-item depression section of the Cambridge Mental Disorders of the Elderly (CAMDEX) (Roth et al., 1986). It was applied as described in detail previously (Johnson, McGue, Gaist, Vaupel, & Christensen, 2002; McGue & Christensen, 1997). Seventeen of the 21 CAMDEX depression items were used to define an overall measure of depression (range of total scale: 17–49), eight items reflected the lack of well-being and were categorized into the affective scale, and nine reflected the lack of energy and were categorized into the somatic scale (McGue & Christensen, 1997). Higher scores on the depression scales reflect the greater levels of depression symptomatology (McGue & Christensen, 2003).
Statistical analyses
The association between the different measurements and age was analyzed separately between genders. Age was divided into 10 age groups (45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90+) and, for continuous measurements, significant differences in means were tested using one-way analysis of variance (ANOVA). For dichotomized measurements, significant differences in proportions by age groups were tested using a chi-square test. In the interest of the graphic representations, an average age within each age group was calculated and used as the x-coordinate in the figures.
To estimate difference per decade, linear regression analysis was performed for continuous variables, and binomial generalized linear regression was performed for binary variables. Both used age divided by 10 as the independent variable. The assumed linear association was graphically inspected and no major deviances were observed except for the binary variables, where a linear spline with a knot at age 70 clearly showed a better fit to the data.
To compare age-related differences across the different continuous measures with their differing means and standard deviations, the T-score (Hale & Astolfi, 2011; McGue & Christensen, 2013) was calculated for the cognitive composite score, the total depression score, the mobility score, and the ordinal happiness measure. In short, a Z-score for the result of each individual was calculated by using the mean and the standard deviation of the youngest age group, and subsequently this was standardized to a mean of 50 and a standard deviation of 10 (Hale & Astolfi, 2011), separately for the two genders. Thus, a T-score of 40 for an age group indicates that, on average, the function level is 1 SD lower than that of the standardized population mean for those aged 45–49. For these analyses, we selected only those cases with complete data in all of the measures (n = 9877).
Results
Participant characteristics
Overall, the average age was 72.9 (SD 14.8) years and there was a minimum of 494 participants in each age group (Table 1). The 2411 participants in the 90+ year age group had a range of 90–102 years, but with 95% being 92–93 years due to the inclusion of participants from the C1905 study. Participation rates were the highest for men and varied between 62% and 85% by age group (Table 1).
Table 1.
Sample size, mean age, and participation rates by age and gender.
| Age group | All | Men | Women | |||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| N | Mean age (years) (SD) | N | Participation rate (%) | N | Participation rate (%) | |
| 45–49 | 792 | 48.0 (1.1) | 398 | 83.2 | 394 | 82.2 |
| 50–54 | 1014 | 52.5 (1.5) | 515 | 85.4 | 499 | 81.8 |
| 55–59 | 975 | 57.5 (1.4) | 507 | 82.9 | 468 | 79.6 |
| 60–64 | 959 | 62.5 (1.4) | 479 | 81.9 | 480 | 78.4 |
| 65–69 | 574 | 66.5 (0.8) | 299 | 82.3 | 275 | 77.9 |
| 70–74 | 1756 | 72.5 (1.4) | 833 | 72.5 | 923 | 63.1 |
| 75–79 | 1548 | 77.0 (1.4) | 610 | 76.4 | 938 | 71.2 |
| 80–84 | 784 | 82.4 (1.4) | 291 | 78.3 | 493 | 73.8 |
| 85–89 | 494 | 87.0 (1.4) | 168 | 84.8 | 326 | 79.6 |
| 90+ | 2411 | 93.1 (0.7) | 625 | 69.8 | 1786 | 61.7 |
| All | 11,307 | 72.9 (14.8) | 4725 | 78.1 | 6582 | 70.2 |
Measurements by age groups
Performance in selected cognitive tests was poorer in the oldest age groups (Figure 1, panels (A)–(D)). For example, naming animals in 1 minute decreased from an average of 24 at the ages of 45–49 to 13 at the ages above 90 and words remembered after 10 minutes dropped from 7 to only 1 word on average. Also, high scores of depression symptomatology were found with older age, but with a much smaller gradient (Figure 1, panels (E)–(G)). In females, the total score of depression symptomatology (panel (E)) went from 19.3 through 21.5 to 25.5 in the age groups 45–49, 70–74, and 90+. Furthermore, larger differences across age groups were found in the somatic scale compared with the affective scale of the depression symptomatology score (panels (F)–(G)). Proportions of each age group being able to manage stairs, walk 400 meters without rest, and run 100 meters became smaller with older age (Figure 2). Being able to run 100 meters had a very pronounced decrease from 90% in the youngest age group to almost 0% in the oldest. The proportion of being happy also showed a decrease with age, but the drop was far less dramatic from around 90% in most age groups and dropping below 80% only in the 90+ age group with 72% men and 75% women being happy.
Figure 1.
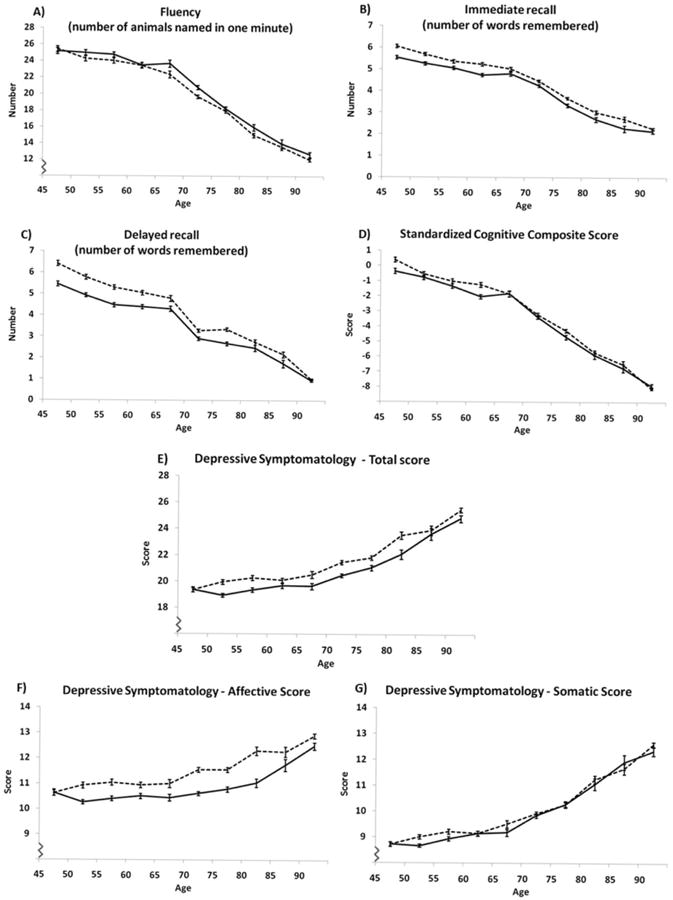
Descriptors of selected items from the cognitive composite score (panels (A)–(C)), the cognitive composite score (panel (D)), and the total score of symptoms of depression and its affective and somatic subscale scores (panels (E)–(G)) by age and gender. Data are presented as means and 95% confidence interval.
Figure 2.
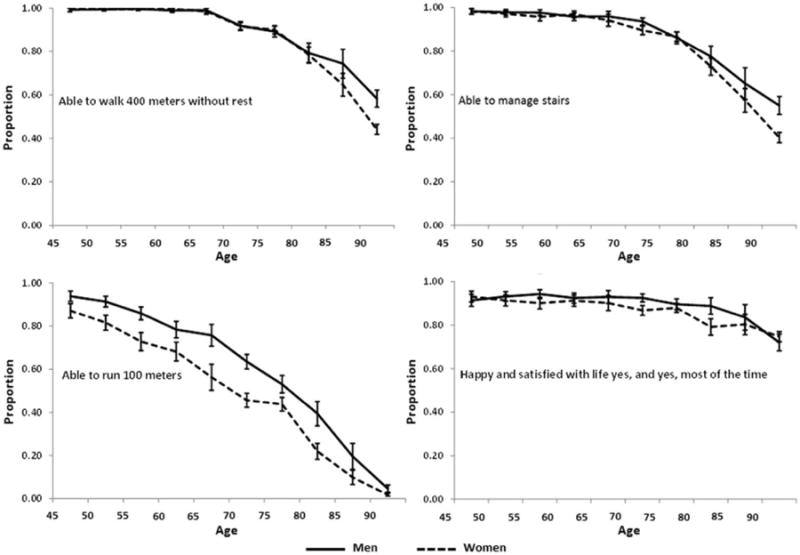
Proportions being able to perform selected mobility activities and stating being happy and satisfied with life by sex and age groups. Data are presented as proportions and 95% confidence interval.
With regard to gender differences in the age-adjusted analysis, males named more animals, had lower total depression symptomatology, lower affective and somatic scale score of depression symptomatology than females (all p < 0.02). Conversely, females were able to recall more words both immediately and after delay, and also had a better overall cognitive composite score (all p < 0.001). Moreover, more males than females were able to walk 400 meters without rest, manage stairs, run 100 meters, and more males than females reported being happy (all p < 0.001).
Estimation of age group differences
The estimation of age-related differences per decade (Table 2) for continuous measures showed very little gradient among those below 70 years, in particular, for the three scales of depression symptomatology, and a larger gradient among those 70 years and older. For all the binary variables, the decrease in prevalence was substantially higher among those 70 years and older compared to those below 70 years. Except for running 100 meters, the decrease in prevalence below the age of 70 was small (a decline in prevalence of around 0.01, or 1%, per decade) and except for being happy, the decrease in prevalence was high above the age of 70 (a decline in prevalence of around 0.20%, or 20%, per decade). Being happy generally showed a lower decrease in prevalence difference per decade. The differences in the regression coefficients and the prevalence differences of those below 70 years versus those 70 years and older were all highly statistically significant (all p < 0.001).
Table 2.
Estimated difference in mental and physical functioning and happiness per decade year by gender.
| Men | Women | |||
|---|---|---|---|---|
|
|
|
|||
| <70 years | ≥70 years | <70 years | ≥70 years | |
|
| ||||
| Continuous variables (mean difference/10 years (95% CI)) | ||||
| Number of animals named | −1.10 (−1.58; −0.61)† | −3.93 (−4.27; −3.58)‡ | −1.44 (−1.92; −0.95)‡ | −3.74 (−3.98; −3.50)‡ |
| Numbers of words remembered immediately | −0.45 (−0.55; −0.34)‡ | −1.02 (−1.11; −0.93)‡ | −0.55 (−0.66; −0.44)‡ | −1.01 (−1.08; −0.94)‡ |
| Numbers of words remembered after delay | −0.60 (−0.75; −0.46)‡ | −0.93 (−1.03; −0.83)‡ | −0.90 (−1.06; −0.74)‡ | − 1.20 (−1.28; −1.12)‡ |
| Cognition (CCS) | −0.93 (−1.15; −0.71)‡ | −2.18 (−2.35; −2.01)‡ | − 1.12 (−1.35; −0.89)‡ | −2.36 (−2.49; −2.24)‡ |
| Depression symptomatology | ||||
| Total score | 0.32 (0.09; 0.56)† | 2.16 (1.91; 2.41)‡ | 0.53 (0.26; 0.80)‡ | 2.06 (1.85; 2.27)‡ |
| Affective scale | 0.004 (−0.14; 0.15)ns | 0.90 (0.77; 1.03)‡ | 0.18 (0.01; 0.35)* | 0.72 (0.59; 0.84)‡ |
| Somatic scale | 0.32 (0.19; 0.44)‡ | 1.26 (1.10; 1.42)‡ | 0.35 (0.22; 0.49)‡ | 1.34 (1.23; 1.46)‡ |
| Binary variables (prevalence difference/10 years (95% CI)) | ||||
| Walk 400 meters without rest | −0.002 (−0.01; 0.003)ns | −0.15 (−0.17; −0.13)‡ | −0.005 (−0.01; −0.004)‡ | −0.22 (−0.23; −0.21)‡ |
| Manage stairs | −0.01 (−0.03; −0.004)† | −0.18 (−0.19; −0.16)‡ | −0.01 (−0.03; −0.002)* | −0.23 (−0.25; −0.22)‡ |
| Able to run 100 meters | −0.10 (−0.12; −0.08)‡ | −0.29 (−0.31; −0.27)‡ | −0.15 (−0.18; −0.12)‡ | −0.22 (−0.24; −0.21)‡ |
| Happy: yes, and yes, almost always | 0.003 (−0.01; 0.02)ns | −0.09 (−0.10; −0.07)‡ | −0.01 (−0.03; 0.01)ns | −0.06 (−0.08; −0.05)† |
Notes: CCS = standardized cognitive composite score. CI = confidence interval.
p < 0.05;
p < 0.01;
p < 0.001;
ns denotes non-significant.
To evaluate the different magnitudes of age drops among the measures, we used the T-scores. Comparing e.g. the oldest age group with the youngest age group, we found the T-score differences to be largest for the mobility score in which men in the age group of 45–49 had a T-score of 52.7, whereas men in the age group of 90+ had a T-score of 12.5 (Figure 3). The corresponding T-scores for women were 47.2 and 5.8, respectively. This indicates a mobility function of the oldest age group that was approximately 4 SD lower than that of the youngest group. A lower function, although not so drastic, was also found in the cognitive function of the oldest age group, where differences of 2.2 SD and 2.5 SD compared with the youngest group were found for men and women, respectively. Similarly, although in the opposite direction, differences of the total depression symptomatology score for the oldest versus the youngest age group were 1.6 SD and 1.7 SD for men and women, respectively. Finally, the difference for being happy was 0.6 SD for both men and women, when comparing the oldest age group with the youngest.
Figure 3.
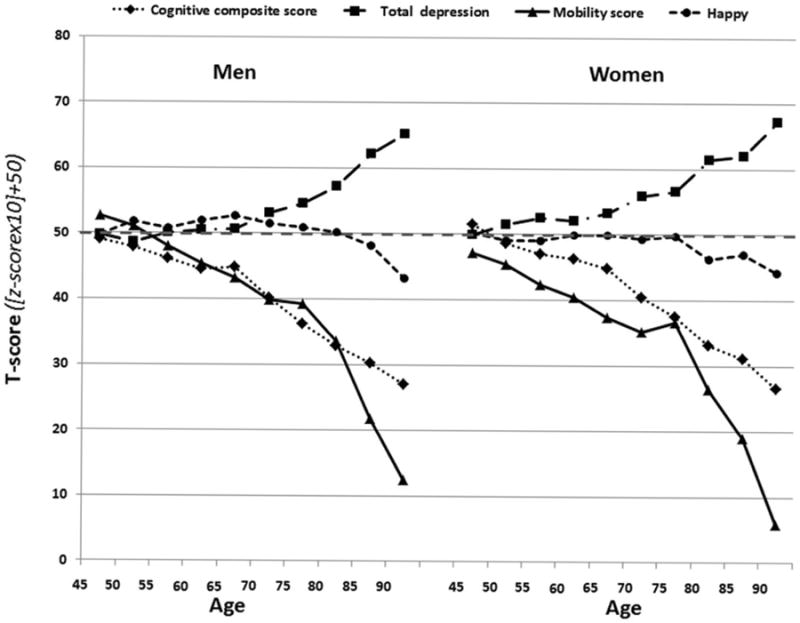
Age-related differences in the scores of physical and mental functions and the feeling of happiness by gender. Mean of each age group by 5-year intervals ranging from 45–49 to 90+ are plotted against T-scores for each measure. T-scores are scaled to have a mean of 50 and a standard deviation of 10.
Discussion
In this Danish sample with individuals aged 45 and onwards, we observed that happiness remained rather unchanged despite large age-related differences between the youngest and oldest age groups in measures of physical and mental functions.
Mental and physical functioning and happiness
The age-related differences observed in physical and mental functions were consistent with previous studies in which higher decline was also observed in the older age groups (Andersen-Ranberg et al., 1999; Crimmins & Beltran-Sanchez, 2011; McGue & Christensen, 2013). Our findings support studies showing lower happiness in older age groups (Easterlin, 2006) and are in contrast to the finding of a U-shape (Blanchflower & Oswald, 2008) or an age-related increase in happiness observed in the literature (Cooper et al., 2011). The differences in the findings of an association between age and happiness in the various studies may be a result of the many different measures of happiness which include e.g. single-item and multi-item instruments with various numbers of response categories as well as visual analog scales (Veenhoven, 2014).
As the feeling of happiness is related to many factors that are not exclusively individual but may be due to external factors such as societal structure and environment (Helliwell et al., 2012), this may, in fact, be the main explanation for the smaller age-related differences in happiness in comparison with the other domains as observed in this study. Among individual factors, an explanation may be found in coping strategies and lowered expectations with age (Ebner, Freund, & Baltes, 2006; Hsu & Tung, 2010; Jopp & Rott, 2006). Another reason for the smaller age-related differences in happiness that we observe could be due to our use of the same single-item happiness question in all age groups. It is conceivable that using a multi-item instrument with a visual analogue scale as a response option could be more sensitive to age-related differences. However, the single-item questions applied in this study to measure functional ability were able to detect substantial age-related differences.
Strengths and limitations
A major strength of the study that we used study samples from population-based surveys retrieved from the Danish Civil Registration System (Pedersen, Gotzsche, Moller, & Mortensen, 2006) or the Danish Twin Registry (Skytthe, Kyvik, Holm, & Christensen, 2011), hereby reducing the potential risk of selection bias compared to e.g. recruiting participants through ads in newspapers.
One of the potential study limitations, which may imply a bias, is the ranking of the Danes as the happiest population in the world (Christensen, Herskind, & Vaupel, 2006; Helliwell et al., 2012; Ott, 2011) despite a shorter life expectancy compared with e.g. other Scandinavian countries (Christensen et al., 2010; Jacobsen, von Euler, Osler, Lynge, & Keiding, 2004). Moreover, Denmark had the lowest GINI coefficient, which is a measure of income inequality, among 20 countries in the Organisation for Economic Co-operation and Development (OECD) during the mid 1990s and the 2000s (OECD, 2011). This reflects the fact that Danes live in an egalitarian society in which mutual respect and conceivably also happiness can thrive (Christensen et al., 2006; Helliwell et al., 2012; OECD, 2011). Also, our measure of happiness was a part of the adapted version of the CAM-DEX depression score (McGue & Christensen, 1997), which was also used to describe depression symptomatology in this study. As larger age-related differences were observed for the full depression scale than for happiness alone, this may lead to the interpretation that Danes insist on retaining their feeling of happiness as long as possible. Furthermore, in another study using the same data as ours, the percentage rating their health as better in comparison with age-peers increased from about 30% to 70% for the age group between 40+ and 90+ years (Andersen, Christensen, & Frederiksen, 2007). Thus, assuming a particular Danish approach to the feeling of happiness, the results of this study may not be generalizable to other countries.
Even though we argue that selection bias is smaller in this study than in most studies, selection bias should be considered when interpreting the results of our study as non-responders to participation in the various intake interviews may be particularly unhappy. However, they might also be those with the poorest function. Furthermore, when calculating the T-score, and thereby enabling the comparison of age-related differences across outcomes, missing data primarily in cognitive decline and depression symptomatology resulted in a reduction of the analytic sample from 11,307 to 9877. Our post hoc analysis showed that the cases without complete data had poorer mobility function than those with full data. However, this is unlikely to jeopardize the overall conclusion about the age-related differences as happy people are likely to be those with better function regardless of age.
This study is a cross-sectional study and, therefore, we are not describing age changes and not able to illustrate possible cohort effects. A recent study of 90+-year-old individuals found cohort effects in cognitive function and activities of daily living with better function in later cohorts, but not for depression symptomatology and physical performance measured (Christensen et al., 2013). The impact of a cohort effect in this study would imply that we might have overestimated age-related differences. At the same time, a study on birth cohort effects in the feeling of happiness reported generally similar levels of well-being across birth generations (Blanchflower & Oswald, 2008).
Finally, treating twins as individuals in the data analysis for this study might be considered problematic. However, through register linkage with other Danish large-scale surveys and health and social registers, it was observed that twins are generally representative of the general population in terms of health and survival after the difficult infancy period (Christensen et al., 2006; Christensen & McGue, 2012; Christensen, Vaupel, Holm, & Yashin, 1995). Still, we acknowledge that it remains unstudied whether twins and singletons are similar in terms of happiness per se. Nevertheless, differences in well-being between twins and singletons were less than 0.05 SD and thus very small (Johnson, Krueger, Bouchard, & McGue, 2002). Furthermore, both lower suicide risk in twins and similarity in the self-report of depression have been found in other studies comparing twins and singletons (Moilanen et al., 1999; Tomassini, Juel, Holm, Skytthe, & Christensen, 2003).
Conclusions
In conclusion, in a sample of more than 10,000 Danes aged 45–90+, we observed that age-related differences in the feeling of happiness do not closely track well-established age-related declines in physical and mental functions. Although we are not able to separate the age and cohort effects, we suggest that the smaller age group differences observed for depression and happiness as compared to the other outcomes may be a result of an inherent adjustment for age and sex with the adaptation that respondents automatically apply when answering the question (i.e. a more relative judgment). Randomized controlled trials could be the next step to study whether help to improve or maintain particularly the mobility function could be an intervention, among many, to be used in the effort to increase happiness in the populations – as endorsed by the United Nations.
Acknowledgments
Funding: This work was supported by grants from the US National Institute on Aging [grant number P01-AG08761]; National Institute on Alcohol Abuse and Alcoholism [grant number R01 AA009367]; the Danish Ageing Research Center is supported by a grant from the VELUX Foundation.
References
- Andersen FK, Christensen K, Frederiksen H. Self-rated health and age: A cross-sectional and longitudinal study of 11,000 Danes aged 45 – 102. Scandinavian Journal of Public Health. 2007;35:164–171. doi: 10.1080/14034940600975674. [DOI] [PubMed] [Google Scholar]
- Andersen-Ranberg K, Christensen K, Jeune B, Skytthe A, Vasegaard L, Vaupel JW. Declining physical abilities with age: A cross-sectional study of older twins and centenarians in Denmark. Age Ageing. 1999;28:373–377. doi: 10.1093/ageing/28.4.373. [DOI] [PubMed] [Google Scholar]
- Blanchflower DG, Oswald AJ. Is well-being U-shaped over the life cycle? Social Science & Medicine. 2008;66:1733–1749. doi: 10.1016/j.socscimed.2008.01.030. [DOI] [PubMed] [Google Scholar]
- Christensen K, Davidsen M, Juel K, Mortensen L, Rau R, Vaupel JW. The divergent life-expectancy trends in Denmark and Sweden – and some potential explanations. In: Crimmins EM, Preston SH, Cohen B, editors. International differences in mortality at older ages Dimensions and sources. Washington, DC: The National Academies Press; 2010. pp. 385–407. [PubMed] [Google Scholar]
- Christensen K, Herskind AM, Vaupel JW. Why Danes are smug: Comparative study of life satisfaction in the European Union. British Medical Journal. 2006;333:1289–1291. doi: 10.1136/bmj.39028.665602.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen K, Holm NV, McGue M, Corder L, Vaupel JW. A Danish population-based twin study on general health in the elderly. Journal of Aging and Health. 1999;11:49–64. doi: 10.1177/089826439901100103. [DOI] [PubMed] [Google Scholar]
- Christensen K, McGue M. Commentary: Twins, worms and life course epidemiology. International Journal of Epidemiology. 2012;41:1010–1011. doi: 10.1093/ije/dys101. [DOI] [PubMed] [Google Scholar]
- Christensen K, Petersen I, Skytthe A, Herskind AM, McGue M, Bingley P. Comparison of academic performance of twins and singletons in adolescence: Follow-up study. British Medical Journal. 2006;333:1095–1097. doi: 10.1136/bmj.38959.650903.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen K, Thinggaard M, Oksuzyan A, Steenstrup T, Andersen-Ranberg K, Jeune B, et al. Vaupel JW. Physical and cognitive functioning of people older than 90 years: A comparison of two Danish cohorts born 10 years apart. Lancet. 2013;382:1507–1513. doi: 10.1016/S0140-6736(13)60777-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen K, Vaupel JW, Holm NV, Yashin AI. Mortality among twins after age 6: Fetal origins hypothesis versus twin method. British Medical Journal. 1995;310:432–436. doi: 10.1136/bmj.310.6977.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper C, Bebbington P, King M, Jenkins R, Farrell M, Brugha T, et al. Livingston G. Happiness across age groups: Results from the 2007 National Psychiatric Morbidity Survey. International Journal of Geriatric Psychiatry. 2011;26:608–614. doi: 10.1002/gps.2570. [DOI] [PubMed] [Google Scholar]
- Cooper C, Bebbington P, Livingston G. Cognitive impairment and happiness in old people in low and middle income countries: Results from the 10/66 study. Journal of Affective Disorders. 2011;130:198–204. doi: 10.1016/j.jad.2010.09.017. [DOI] [PubMed] [Google Scholar]
- Crimmins EM, Beltran-Sanchez H. Mortality and morbidity trends: Is there compression of morbidity? Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2011;66:75–86. doi: 10.1093/geronb/gbq088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Easterlin RA. Life cycle happiness and its sources – intersections of psychology, economics, and demography. Journal of Economic Psychology. 2006;27:463–482. [Google Scholar]
- Ebner NC, Freund AM, Baltes PB. Developmental changes in personal goal orientation from young to late adulthood: From striving for gains to maintenance and prevention of losses. Psychology and Aging. 2006;21:664–678. doi: 10.1037/0882-7974.21.4.664. [DOI] [PubMed] [Google Scholar]
- Frederiksen H, Hjelmborg J, Mortensen J, McGue M, Vaupel JW, Christensen K. Age trajectories of grip strength: Cross-sectional and longitudinal data among 8,342 Danes aged 46 to 102. Annals of Epidemiology. 2006;16:554–562. doi: 10.1016/j.annepidem.2005.10.006. [DOI] [PubMed] [Google Scholar]
- Freedman VA, Stafford F, Schwarz N, Conrad F, Cornman JC. Disability, participation, and subjective wellbeing among older couples. Social Science & Medicine. 2012;74:588–596. doi: 10.1016/j.socscimed.2011.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frijters P, Beatton T. The mystery of the U-shaped relationship between happiness and age. Journal of Economic Behavior and Organization. 2012;82:525–542. [Google Scholar]
- Gaist D, Bathum L, Skytthe A, Jensen TK, McGue M, Vaupel JW, Christensen K. Strength and anthropometric measures in identical and fraternal twins: No evidence of masculinization of females with male co-twins. Epidemiology. 2000;11:340–343. doi: 10.1097/00001648-200005000-00020. [DOI] [PubMed] [Google Scholar]
- Gerstorf D, Ram N, Mayraz G, Hidajat M, Lindenberger U, Wagner GG, Schupp J. Late-life decline in well-being across adulthood in Germany, the United Kingdom, and the United States: Something is seriously wrong at the end of life. Psychology and Aging. 2010;25:477–485. doi: 10.1037/a0017543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hale CD, Astolfi D, editors. Measuring Learning & Performance: A Primer. 2nd. St. Leo, FL: Saint Leo University; 2011. Standardized testing: Introduction; pp. 183–197. Retrived from http://www.charlesdennishale.com/ [Google Scholar]
- Helliwell J, Layard R, Sachs J, editors. World happiness report. New York, NY: Earth Institute, Columbia University; 2012. Retrived from http://issuu.com/earthinstitute/docs/world-happiness-report. [Google Scholar]
- Hsu HC, Tung HJ. What makes you good and happy? Effects of internal and external resources to adaptation and psychological well-being for the disabled elderly in Taiwan. Aging and Mental Health. 2010;14:851–860. doi: 10.1080/13607861003800997. [DOI] [PubMed] [Google Scholar]
- Jacobsen R, von Euler M, Osler M, Lynge E, Keiding N. Women's death in Scandinavia – what makes Denmark different? European Journal of Epidemiology. 2004;19:117–121. doi: 10.1023/b:ejep.0000017834.35943.bd. [DOI] [PubMed] [Google Scholar]
- Johnson W, Krueger RF, Bouchard TJ, Jr, McGue M. The personalities of twins: Just ordinary folks. Twin Research. 2002;5:125–131. doi: 10.1375/1369052022992. [DOI] [PubMed] [Google Scholar]
- Johnson W, McGue M, Gaist D, Vaupel JW, Christensen K. Frequency and heritability of depression symptomatology in the second half of life: Evidence from Danish twins over 45. Psychological Medicine. 2002;32:1175–1185. doi: 10.1017/s0033291702006207. [DOI] [PubMed] [Google Scholar]
- Jopp D, Rott C. Adaptation in very old age: Exploring the role of resources, beliefs, and attitudes for centenarians' happiness. Psychology and Aging. 2006;21:266–280. doi: 10.1037/0882-7974.21.2.266. [DOI] [PubMed] [Google Scholar]
- McGue M, Christensen K. Genetic and environmental contributions to depression symptomatology: Evidence from Danish twins 75 years of age and older. Journal of Abnormal Psychology. 1997;106:439–448. doi: 10.1037//0021-843x.106.3.439. [DOI] [PubMed] [Google Scholar]
- McGue M, Christensen K. The heritability of cognitive functioning in very old adults: Evidence from Danish twins aged 75 years and older. Psychology and Aging. 2001;16:272–280. doi: 10.1037//0882-7974.16.2.272. [DOI] [PubMed] [Google Scholar]
- McGue M, Christensen K. The heritability of depression symptoms in elderly Danish twins: Occasion-specific versus general effects. Behavior Genetics. 2003;33:83–93. doi: 10.1023/a:1022545600034. [DOI] [PubMed] [Google Scholar]
- McGue M, Christensen K. Growing old but not growing apart: Twin similarity in the latter half of the lifespan. Behavior Genetics. 2013;43:1–12. doi: 10.1007/s10519-012-9559-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moilanen I, Linna SL, Ebeling H, Kumpulainen K, Tamminen T, Piha J, Almqvist F. Are twins' behavioural/emotional problems different from singletons'? European Child and Adolescent Psychiatry. 1999;8(Suppl. 4):62–67. doi: 10.1007/pl00010702. [DOI] [PubMed] [Google Scholar]
- Nybo H, Gaist D, Jeune B, Bathum L, McGue M, Vaupel JW, Christensen K. The Danish 1905 cohort: A genetic-epidemiological nationwide survey. Journal of Aging and Health. 2001;13:32–46. doi: 10.1177/089826430101300102. [DOI] [PubMed] [Google Scholar]
- OECD. Divided we stand: Why inequality keeps rising. OECD Publishing; 2011. [Table 6.A1.1., p. 249]. Retrieved from http://dx.doi.org/10.1787/9789264119536-en. [Google Scholar]
- Ott JC. Government and happiness in 130 nations: Good governance fosters higher level and more equality of happiness. Social Indicators Research. 2011;102:3–22. doi: 10.1007/s11205-010-9719-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The Danish civil registration system. A cohort of eight million persons. Danish Medical Bulletin. 2006;53:441–449. [PubMed] [Google Scholar]
- Roth M, Tym E, Mountjoy CQ, Huppert FA, Hendrie H, Verma S, Goddard R. CAMDEX. A standardised instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection of dementia. British Journal of Psychiatry. 1986;149:698–709. doi: 10.1192/bjp.149.6.698. [DOI] [PubMed] [Google Scholar]
- Skytthe A, Kyvik KO, Holm NV, Christensen K. The Danish twin registry. Scandinavian Journal of Public Health. 2011;39:75–78. doi: 10.1177/1403494810387966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stathokostas L, Jacob-Johnson S, Petrella RJ, Paterson DH. Longitudinal changes in aerobic power in older men and women. Journal of Applied Physiology. 2004;97:781–789. doi: 10.1152/japplphysiol.00447.2003. [DOI] [PubMed] [Google Scholar]
- Tomassini C, Juel K, Holm NV, Skytthe A, Christensen K. Risk of suicide in twins: 51 year follow up study. British Medical Journal. 2003;327:373–374. doi: 10.1136/bmj.327.7411.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations. International day of happiness. 2013 Retrieved March 20, 2013, from http://www.un.org/en/events/happinessday/
- Veenhoven R. Measures of Happiness. World Database of Happiness. 2014 Retrieved from http://worlddatabaseofhappiness.eur.nl/hap_quer/hqi_fp.htm.
- Wunder C, Wiencierz A, Schwarze J, Kuchenhoff H. Well-being over the life span: Semiparametric evidence from British and German longitudinal data. Review of Economic Statistics. 2013;95:154–167. [Google Scholar]