

Abstract
This study aimed to improve the understanding of the clinical characteristics of patients with fasciolopsiasis and thus reduce misdiagnosis and inappropriate treatment. We retrospectively analyzed the clinical data of two patients with fasciolopsiasis which caused appendicitis. Fasciolopsis buski infestation as a cause of appendicitis is very rarely seen in the clinic. The clinical characteristics, clinical manifestations, diagnostic methods and the principles of treatment in these two patients were analyzed.
Keywords: Fasciolopsis buski, Appendicitis, Fasciolopsiasis, Misdiagnosis
Core tip: The incidence of Fasciolopsis buski infestation is low in modern society, and Fasciolopsis buski infestation as a cause of acute appendicitis is even rare. We describe two patients with appendicitis caused by Fasciolopsis buski infestation and summarize the diagnosis and treatment of the disease.
INTRODUCTION
Fasciolopsis buski, also known as the Asian large bowel trematode[1], is a large parasite, which is normally found in the human small intestine and can cause fasciolopsiasis. The incidence of fasciolopsiasis is often associated with aquatic plants. This disease occurs due to the ingestion of infected aquatic foods or contact with infected pigs. Adult Fasciolopsis buski live in the jejunum of the definitive host and cause mechanical damage to the bowel wall in the human host. The parasites and their metabolites can cause an allergic reaction. This disease is rarely seen in the clinic, but can occur during a particular season. Fasciolopsis buski covering the appendiceal orifice leading to appendicitis is very rare. We present two cases of appendicitis due to mechanical obstruction caused by Fasciolopsis buski infestation.
CASE REPORT
Case 1
A 45-year-old woman was admitted to our hospital due to right lower abdominal pain. The abdominal pain started five days previously with no obvious predisposing causes. This paroxysmal dull pain was mainly noted around the navel. The patient’s temperature was normal. The pain then shifted to the right lower quadrant. Anal discomfort and mild itching were observed and she underwent abdominal ultrasound as an outpatient. Mild swelling of the appendix was noted, the echo was reduced and distribution was uneven, the appendix was approximately 62 mm × 9 mm × 6 mm in size, and a portion of the bowel in the right lower quadrant was slightly broadened without effusion between the intestines. The patient was thought to have appendicitis and was admitted to hospital. Her physical examination showed a temperature of 37.9 °C, pulse rate of 80 beats/min, respiration rate of 19 breaths/min, and blood pressure of 130/60 mmHg. The ventral area was soft and the McBurney point showed mild tenderness, with no rebound tenderness. Bowel sounds were slightly active, Rovsing’s sign was positive, and psoas sign and obturator sign were negative. A routine blood examination showed a white blood cell (WBC) of 4.4×109/L, neutrophils (NEUT)% of 51.4%, leukomonocyte % of 35.8%, eosinophils (EO)% of 0.5%, neutrophils of 2.3 × 109/L, leukomonocyte of 1.6×109/L, eosinophils of 0.6 × 109/L, red blood cell (RBC) of 3.21 × 1012/L, hemoglobin (HGB) of 101 g/L, packed cell volume (PCV) of 0.210 L/L, and platelet (PLT) 142 × 109/L. These findings demonstrated that the patient was mildly anemic, her WBC was normal and EO was increased. This patient’s disease course was more than 3 d, thus we considered her to have serious periappendicular inflammation. She was treated conservatively with anti-inflammatory therapy and another routine blood examination was carried out 5 d later which showed a RBC of 2.81 × 1012/L, HGB of 89 g/L, and WBC 3.4 × 109/L. Her HGB progressively declined and the patient underwent colonoscopy (Figure 1A) which showed two red oval objects around the ileocecal-appendiceal orifice. The examiner first thought that these were ileocecal adenomatous colon polyps. However, on biopsy, they were found to be alive with obvious peristalsis. The heads were attached to the intestinal wall by suckers. The parasites were large, hypertrophic, red in color and oval, dorsoventrally flat with a narrow head and wide rear. Following removal of these parasites (Figure 1B), parts of the ileocecal intestinal wall showed hyperemia with edema and areas of bleeding. The mucous membrane was pale and ischemic and the appendiceal orifice was mildly hyperemic. Based on the results of colonoscopy, we considered that a parasitic infestation of the ileocecal-appendiceal orifice had subsequently resulted in local appendicitis. The parasites were sent to the parasite office of the Centers for Disease Control and Prevention (CDC) and were identified as Fasciolopsis buski. Following centrifugal precipitation of the patient’s stool smear, Fasciolopsis buski eggs were found on microscopy. The final clinical diagnosis was Fasciolopsis buski infestation. The patient received oral praziquantel and her abdominal pain disappeared.
Figure 1.
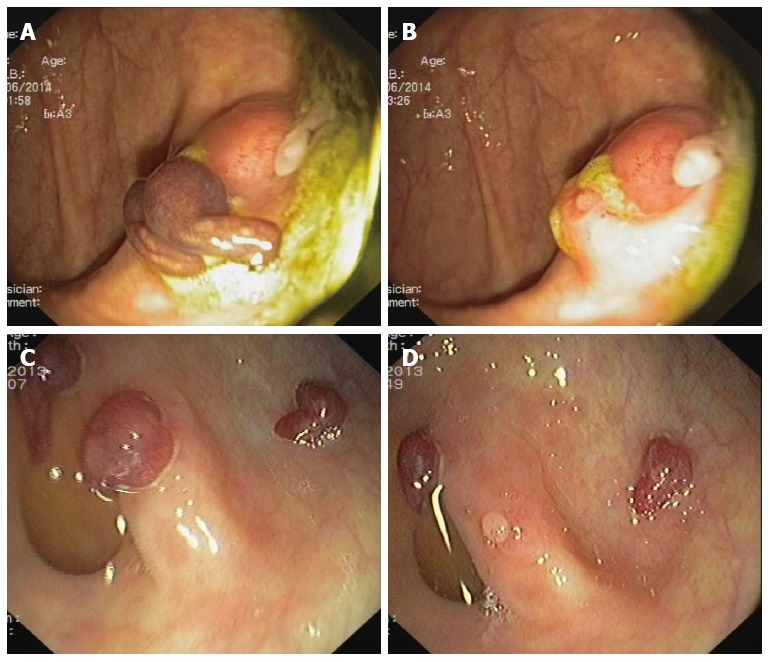
Colonoscopy. A: Two worm-like parasites covering the appendiceal orifice; B: Following removal of the parasites, the appendiceal orifice showed hyperemia and edema; C: Three live parasites were found at the ileocecal-appendiceal orifice; D: Following removal of the parasites, parts of the intestinal wall showed hyperemia and edema, and the mucosa was pale and ischemic.
Case 2
A 71-year-old woman attended the outpatient service due to repeated watery stools with dull right lower abdominal pain for 3 mo. The patient did not spit blood, and did not experience tarry stools, severe abdominal pain, chills or fever. Her physical examination showed ventral softness, mild tenderness around the navel, tenderness around the McBurney point, no rebound tenderness or ascites, and active bowel sounds. Feces examination did not show pus cells, red blood cells or eggs. Routine blood examination showed a WBC of 5.2 × 109/L, NEUT of 2.7 × 109/L, EO of 0.5 × 109/L, RBC of 3.04 × 1012/L, HGB of 75 g/L, PCV of 0.180 L/L, and PLT of 212 × 109/L. These findings demonstrated that the patient was moderately anemic and her EO was increased. Colonoscopy showed three red oval objects around the ileocecal-appendiceal orifice (Figure 1C). These objects moved when the examiner touched them and they were attached to the intestinal wall by suckers. The appendiceal orifice and parts of the intestinal wall were hyperemic with edema. The parasites were sent to the parasite office of the CDC and were identified as Fasciolopsis buski (Figure 1D). The patient received oral praziquantel and her diarrhea and abdominal pain significantly improved.
DISCUSSION
Fasciolopsis buski is found in the human small intestine and causes fasciolopsiasis. The incidence of this disease is often associated with growing aquatic plants and cultivating pigs. The two patients reported in this study came from the same local area - the countryside of Huyang, Dangtu town of Anhui Province, China. When asked about the medical history of these patients, their families indicated a recent small scale Fasciolopsis buski infestation in the area. Fasciolopsiasis often occurs following the ingestion of infected aquatic foods such as water chestnut, chufa and water bamboo, or contact with infected pigs. The intermediate hosts of Fasciolopsis buski are aquatic foods and the final hosts are humans and pigs. Fasciolopsis buski adults often live in the final host’s upper small intestine (jejunum)[2]. The pathogenesis consists of mechanical injury to the intestinal wall and an allergic reaction caused by the parasite’s metabolites. As the parasite’s sucker matures it strongly adheres to the intestine wall. The mucous membrane can appear necrotic, parts of the intestinal wall can show punctuate bleeding and edema, and some areas can become ulcerated or develop abscesses. The lesions can cause significant infiltration of neutrophils and eosinophils. When routine blood samples are examined, the ratio and quantity of eosinophils are significantly increased. Patients can experience abdominal pain, diarrhea, low temperature, anemia, edema and mental decline. Very few patients die of multiple organ failure. The gold standard for diagnosing fasciolopsiasis is the identification of Fasciolopsis buski eggs or adults in the intestinal lumen. More research on the hosts of Fasciolopsis buski and pathogenesis of the infestation is required[3]. In the clinic, acute and chronic appendicitis caused by Fasciolopsis buski infection has not yet been reported. In this report, the mechanism of appendicitis caused by Fasciolopsis buski in these patients was attachment of the sucker to the appendiceal orifice. This caused a partial blockage in the local appendix lumen, increased intraluminal pressure, inflammation and edema in some areas resulting in acute or chronic appendicitis. This type of appendicitis did not have a clear abdominal pain position, and the pain was not severe. When Fasciolopsis buski did not adsorb the appendiceal orifice entirely, or the location changed, the pain would improve or completely disappear. For diagnosis of this disease, examination of the patient’s feces should be carried out to determine the presence of eggs, and abdominal imaging such as computed tomography and ultrasound can identify inflammation of the appendix, swelling in the lumen, and endoscopy can show peristalsis of live worms in the appendix cavity or appendix[4]. By identifying Fasciolopsis buski adults and eggs, combined with the clinical characteristics of patients such as abdominal pain, the diagnosis is often not difficult. Fasciolopsis buski often infects the upper section of the small intestine[5], however, we found live parasites in the ileocecal junction of both patients. This was different from studies reported in the literature. Many medical staff do not have a deep understanding of Fasciolopsis buski infestation and this may result in misdiagnosis and inappropriate treatment. A comprehensive understanding of the mechanism of ileocecal junction infection has significance in clinical practice.
COMMENTS
Case characteristics
Fasciolopsis buski is a large parasite, is normally found in the human small intestine, and can cause fasciolopsiasis. Fasciolopsis buski covering the appendiceal orifice leading to appendicitis is very rare.
Clinical diagnosis
The physical signs in the two patients were dissimilar. Endoscopic examination and a report from the parasite office of the Centers for Disease Control and Prevention (CDC) was required in one patient, and a feces smear showed Fasciolopsis buski eggs under microscopy in the other patient.
Differential diagnosis
Acute/chronic appendicitis, acute/chronic colitis and an appendix abscess.
Laboratory diagnosis
Colonoscopy showed two live objects around the ileocecal-appendiceal orifice. The parasites were sent to the parasite office of the CDC and were identified as Fasciolopsis buski. Following centrifugal precipitation of the fecal smear, Fasciolopsis buski eggs were found on microscopy.
Imaging diagnosis
In both cases, endoscopy showed Fasciolopsis buski.
Pathological diagnosis
In both cases, the parasite office of the CDC identified Fasciolopsis buski.
Treatment
Both patients received oral praziquantel and abdominal pain disappeared.
Related reports
No cases of appendicitis with mechanical obstruction due to Fasciolopsis buski infestation have been reported in the literature.
Term explanation
Fasciolopsis buski also known as the Asian large bowel trematode, is a large parasite which is normally found in the human small intestine and can cause fasciolopsiasis.
Experiences and lessons
The clinical characteristics of fasciolopsiasis should be understood to reduce misdiagnosis and inappropriate treatment. Authors retrospectively analyzed the clinical data of two patients with fasciolopsiasis which caused appendicitis.
Peer-review
The authors have described two cases of appendicitis’s rare cause: mechanical obstruction due to fasciolopsis buski infestation. The article highlights the clinical characteristics of this rare cause of appendicitis and provides insights into the fasciolopsis buski disease.
Footnotes
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: August 4, 2014
First decision: August 27, 2014
Article in press: November 19, 2014
P- Reviewer: Galvan-Montano A, Karateke F, Rangarajan M S- Editor: Gou SX L- Editor: A E- Editor: Zhang DN
References
- 1.Zhongshan School of Medicine. Human parasitology. 2nd ed. Beijing: People's Medical Publishing House; 1982. pp. 105–119. [Google Scholar]
- 2.Xu YC, Xu F. A case of fasciolopsis buski infections to pernicious anemia and body swelling with ascites. Linchuang Shuxue Yu Jianyan. 2009;11:274. [Google Scholar]
- 3.Xiang CB, Zhang QS, Zhang DB. The investigation and analysis of piece trematode infection from people in China. Zhiye Ye Jiankang. 2003;l9:90. [Google Scholar]
- 4.Lee TH, Huang CT, Chung CS. Education and imaging. Gastrointestinal: fasciolopsis buski infestation diagnosed by upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2011;26:1464. doi: 10.1111/j.1440-1746.2011.06697.x. [DOI] [PubMed] [Google Scholar]
- 5.Karthikeyan G, Ramkumar V, Kumar SP, Ramkumar S, Selvamani S, Vetriveeran B, Karuppasamy N, Moses IC. Intestinal infestation with Fasciolopsis buski leading to acute kidney injury. J Assoc Physicians India. 2013;61:936–938. [PubMed] [Google Scholar]