

Abstract
Background:
It is very important for dentists to be familiar with anomalies of teeth not only for the clinical complications but also their management. Taurodontism also provides a valuable clue in detecting its association with various syndromes and other systemic conditions. The purpose of this study was to assess the prevalence of Taurodont molars among a North Indian population.
Materials and Methods:
A total of 1000 patients’ full-mouth periapical radiographs were screened. The radiographs were evaluated under optimal conditions using double magnifying glasses. A total of 7615 molars (including third molars) were evaluated. The relative incidence and the correlations regarding the location of Taurodont teeth (right versus left side and maxillary versus mandibular) were analyzed using the Chi-square test.
Results:
Twenty-eight patients were found to have a Taurodont molar (11 women and 17 men [P = 0.250]). The prevalence of Taurodont molar was 2.8%. Males had a higher prevalence rate than females (3.4% vs. 2.2%, respectively). A cluster analysis of total Taurodonts in the mandible (45%) versus maxilla (55%) of both males and females combined showed a statistically significant difference (P < 0.05).
Conclusion:
The occurrence of Taurodontism is basically based on racial expression in different populations. These variations in prevalence between different populations may be due to ethnic variations. The occurrence of Taurodont molars among this Indian population was rare.
Keywords: Molar, prevalence, Taurodontism
INTRODUCTION
Taurodontism is defined as the enlargement of the pulp cavity of a molar tooth at the expense of root length. External morphology was used to describe Taurodont teeth that had apically displaced furcation areas. The name was given because of the apparent similarity between these teeth and those of ungulates, especially bulls. Hence, we have the term Taurodont, “tauro” from the latin term for “bull” and “dont” from the Greek term for “tooth”[1] appears to be a continuous trait.[2] Identification of the Taurodont teeth can only be made by radiographic examination as the external morphology of the teeth is within normal configurations. Appearance of a Taurodont tooth is very characteristic, and radiographic examination is the only way to visualize a rectangular configuration of the pulp chamber. The pulp chamber is extremely large with a greater apico-occlusal height and there is no cervical constriction of the teeth. These teeth have short roots and the bifurcation or trifurcation may be only few millimeters above the apices of the roots.[3] Theories regarding the etiology of Taurodontism have been many. It has been suggested that the anomaly represents a primitive pattern, a mutation, a specialized or retrograde character, an atavistic feature, an X-linked trait, familial or an autosomal dominant trait. Although Taurodontism has been reported in association with certain syndromes and some genetic defects, its true significance is still obscure.[4]
Taurodontism appears most frequently as an isolated anomaly, but it has also been associated with several developmental syndromes and anomalies including amelogenesis imperfecta, Down's syndrome, ectodermal dysplasia, Klinefelter syndrome, tricho-dento-osseous syndrome, Mohr syndrome, Wolf–Hirschhorn syndrome and Lowe syndrome.[5] Taurodontism has also been reported to present with other rare syndromes such as Smith–Magenis syndrome,[6] Williams syndrome,[7] McCune–Albright syndrome[8] and Van der Woude syndrome.[9]
Most studies of its prevalence have, however, employed a categorical approach.[10,11,12] Extreme enlargement of the pulp cavity in an ancient population was first reported in Neanderthal teeth from the Krapina,[1,13,14,15] who described it as a distinguishing feature of this Middle Palaeolithic human population.
The prevalence of Taurodontism is reported to range from 2.5% to 11.3% of the human population. This range is likely accounted for by variations in race and differences in diagnostic criteria.[16] Taurodontism is exhibited in 2.5-3.5% of the chromosomally normal Caucasian population, and most of these teeth are hypotaurodontic.[17] The aim of this retrospective study was to evaluate the frequency of the occurrence of Taurodont molars in an Indian dental school patient population using full-mouth periapical radiographs. In this paper, we also emphasize the diagnosis, etiology and anatomic and radiographic characteristics of Taurodont teeth and also its association with various syndromes and anomalies. We also describe the endodontic consideration of such teeth.
MATERIALS AND METHODS
A total of 1000 patients’ retrospective full-mouth periapical radiographs, which were recorded in the Department of Conservative Dentistry and Endodontics, from January 2007 to December 2012, were screened. Each of these patients had to have full-mouth periapical radiographs, had to be at least 18 years of age and had to be of Indian origin. Personal details including age, sex and race of all these patients were recorded to ensure that all patients were of Indian origin. In order to obtain a balanced distribution between male and female patients, an equal number of (500) full-mouth radiographs of male and female patients were studied.
The full-mouth radiographs were taken using Kodak Ultra-speed films (Kodak, Stuttgart, Germany). All radiographs were reviewed under optimal conditions using magnifying glasses. The radiographs were placed on a viewing box and light surrounding the radiograph was blocked. Radiographs of each patient were evaluated by two dentists. If disagreement existed, a joint evaluation of all authors was made until a consensus was reached. Shifman and Channel criteria were used for Taurodont teeth. In 1978, Shifman and Chanannel[12] proposed the following criteria for determining the presence of Taurodontism, the distance between the cementoenamal junction and the floor of the pulp chamber is ≥2.5 mm and if the distance from the lowest point at the occlusal end of the pulp chamber (A) to the highest point at the apical end of the chamber (B) divided by the distance from A to the apex is 0.2 or greater [Figure 1]. The relative incidence and the correlations regarding the location of Taurodont teeth (maxillary versus mandibular and male versus female) were analyzed [Table 1 and Figure 2] using the Chi-squared test.
Figure 1.
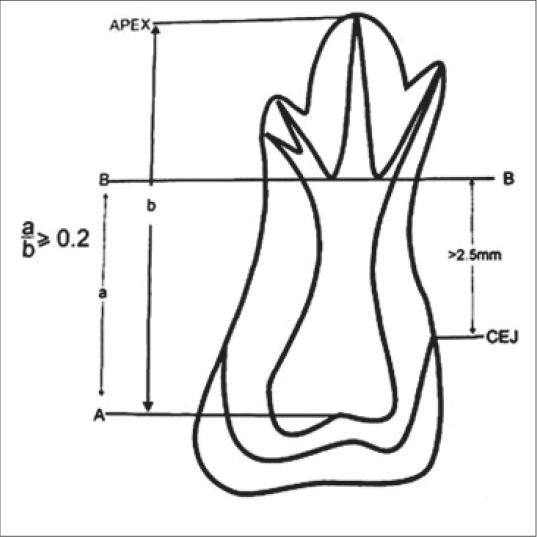
Measurements based on the study by Shifman and Chanannel were used to determine the presence of taurodontism. (A) The lowest point at the occlusal end of the pulp chamber and (B) The highest point at the apical end of the pulp chamber. CEJ, cementoenamel junction
Table 1.
Distribution of teeth examined and Taurodont teeth in the maxilla and mandible
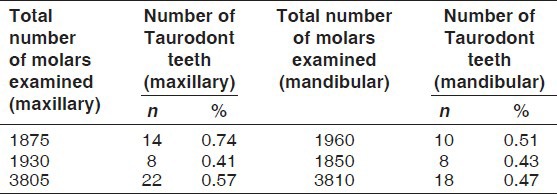
Figure 2.
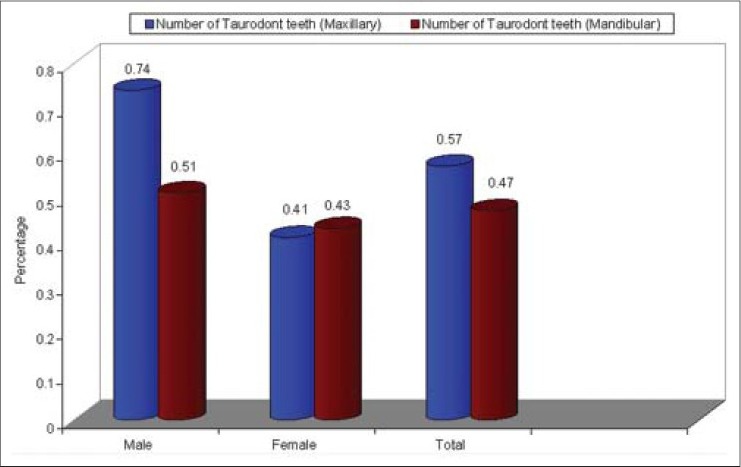
The relative incidence and the correlations regarding the location of Taurodont teeth (maxillary and mandibular) in males and females
RESULTS
One thousand patients, 500 male and 500 female, between the age of 20 and 70 years (average, 45 years) were included in this study. A total of 7615 molars (including the third molars) were evaluated. Maxillary molars comprised 3805 teeth and mandibular molars comprised 3810 teeth [Table 2]. Of the 7615 molars examined, 40 (0.53%) teeth were found to have Taurodontism. These teeth were detected in 28 (2.8%) of 1000 subjects, with 17 as males (60.71%) and 11 as females (39.28%). Twenty-eight patients were found to have a Taurodont molar teeth (24 teeth in male and 16 teeth in female, P = 0.267). The gender distribution of the patients with Taurodontism showed no statistically significant difference. Taurodontism was present in 17 of the 500 male patients (3.4%) and 11 of the 500 female patients (2.2%), P = 0.250 [Table 3 and Figure 3].
Table 2.
Distribution of right and left molars in the maxilla and mandible

Table 3.
Distribution of total subjects and subjects having Taurodont teeth by gender P=0.250 (NS)
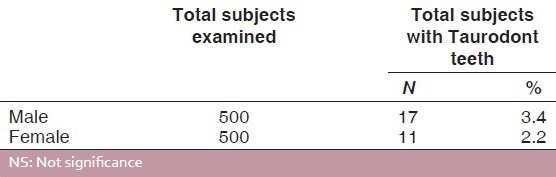
Figure 3.
Distribution of total subjects and subjects having Taurodont teeth by gender
A cluster analysis of total Taurodonts in the mandible (45%) versus the maxilla (55%) of both males and females combined showed a statistically significant difference (P < 0.05; Table 1).
DISCUSSION
Although there have been several studies reporting the prevalence of various dental anomalies, no reported study has been conducted on the prevalence of Taurodontism in an Indian population. In the present study, patients who reported in the OPD of the Department of Conservative Dentistry and Endodontics, Faculty of Dental Sciences, who either underwent restorative treatment or an endodontic procedure, providing an estimation of the prevalence of Taurodontism in the Indian sub-population were analyzed.
The present data indicated that the occurrence of Taurodontism in the Indian population was 2.8%. There is one study in our knowledge that evaluated both maxillary and mandibular molars, reporting the prevalence of Taurodontism in Indians being 2.49%.[18] In a recent study of various malocclusions, the prevalence of Taurodontism was found to be 1%.[19] Darwazeh et al.[20] found a higher rate of 8.0% in Jordanian dental patients; Shifman and Chanannel reported a prevalence of 5.6% in Israeli patients,[12] whereas MacDonald-Jankowski and Li reported an even higher rate (46.4%) of Taurodontism in an adult Chinese population.[17] The difference might arise from racial differences or differences in diagnostic criteria. The prevalence rates reported by previous studies range from 0.25% to 48% in different populations.[21]
In the present study, men presented a higher prevalence of Taurodont teeth than women, although these differences were not statistically significant (P = 0.250). However, the present observation is different from a previous study on Asians that reported a higher prevalence in women.[17]
The diagnosis of Taurodontism using panoramic radiographs is difficult; the anterior regions of both jaws may become distorted and this may result in an incorrect diagnosis of Taurodontic molars.[22,23] Additionally, the differential diagnosis between Taurodontic teeth and other teeth exhibiting large pulp chambers (patients with amelogenesis imperfecta seem to have large pulp chambers because of the lack of enamel) is of clinical significance. Nevertheless, a reliable diagnosis of Taurodontic molars has been shown to be possible using orthopantomograms.[23] However, to ensure proper identification and the best accuracy of assessment, full-mouth periapical radiographs were used in the present study.
On the basis of the external morphology, Shaw proposed a classification of Taurodont teeth, but later a more accurate approach was established by Keen[11] for the categorization of taurodontic teeth using internal morphology. He proposed the Taurodont Index as an objective method for the assessment and related the height of the pulp chamber to the length of the longest root. This index is used as a biological landmark that undergoes changes during the whole life. To overcome these changes, Shifman and Chananel[12] used landmarks that are not modified by apposition of reparative dentine or morphological changes of the root anatomy. Currently, this method is most common and accepted. However, even this ratio can be affected by incomplete root formation or radicular resorption. In addition, root length varies by sex and ethnic groups, which may cast some doubt on the credibility of any metric method as a screening tool for Taurodontism between different populations, and limits the comparability of the results of different studies.[21]
Recently, a case report highlighted the use of high-end diagnostic imaging modalities such as spiral computerized tomography in making a confirmatory diagnosis of the multiple morphologic abnormalities such as Taurodontism, dens invaginatus, pyramidal cusps of the premolars and dens evaginatus.[24]
From an endodontist's view, Taurodontism presents a challenge during negotiation, instrumentation and obturation in root canal therapy. Magnification devices such as magnifying loupes or surgical microscopes can be helpful to locate canal orifices, evaluate the pulp chamber and obturate the canals.[25]
The importance of Taurodontism is felt more by Endodontists while negotiating the complex internal anatomy of such teeth. Shifman and Buchner stressed on the importance of gaining access to the canal orifice, which is not difficult in such teeth due to the absence of reactional dentin that is present in normal teeth[3]; however, this view was contradictory to the study by Durr et al., which says that such a morphology could make the orifice location difficult, creating further difficulty during root canal preparation and obturation.[26]
Hayashi reported mandibular Taurodont tooth with five canals, wherein only three canals could be instrumented till the working length. He also explained the presence of extra root canals in terms of shape and number.[25] It is therefore stressed that careful exploration of canal orifices and grooves is mandatory under the magnification the diagnosis of Taurodont tooth is established. The use of magnification always helps in revealing additional orifices and canals.[27]
The voluminous pulp present in Taurodont teeth needs to be removed completely for the success of treatment; it is here that the importance of irrigation comes into play. Prakash et al. suggested copious irrigation with 2.5% sodium hypochlorite to remove pulpal tissue from the irregular canal walls in such teeth.[28] Grossman and Meiman reported that irrigation with 5% sodium hypochlorite for 20 min to 2 h dissolves all pulpal tissue.[29] Moorer and Wesselink demonstrated that one of the major factors in pulpal tissue removal was agitation with irrigation.[30] It is highly recommended that agitation must be done with copious irrigation to get rid of the pulpal tissue in Taurodont teeth.
The proximity of the orifices and deeply situated opening of the canals made it difficult to obturate the canals with any single method of obturation. Therefore, a combination of lateral condensation and warm vertical condensation technique can be performed to achieve the best results.[31]
CONCLUSION
Within the limitations of this study, it was found that:
The present study found the prevalence of Taurodont molar to be 2.8%
Male have a higher prevalence rate then female (3.4% vs. 2.2%, respectively), with P = 0.250
Maxillary molars are most commonly involving teeth than mandibular molars in males, while females have an equal frequency of Taurodont teeth.
The occurrence of Taurodontism is basically based on racial expression in different populations. These variations in prevalence between different populations may be due to ethnic variations, but may also be influenced by differences in criteria used for the interpretation of Taurodontism and also the specific teeth examined.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Keith A. Problems relating to the teeth of the earlier forms of prehistorical man. Proc R Soc Med. 1913;6:103–24. [PMC free article] [PubMed] [Google Scholar]
- 2.Blumberg JE, Hylander WL, Goepp RA. Taurodontism: A biometric study. Am J Phys Anthropol. 1971;34:243–55. doi: 10.1002/ajpa.1330340208. [DOI] [PubMed] [Google Scholar]
- 3.Shifman A, Buchner A. Taurodontism: Report of sixteen cases in Israel. Oral Surg Oral Med Oral Pathol. 1976;41:400–5. doi: 10.1016/0030-4220(76)90153-5. [DOI] [PubMed] [Google Scholar]
- 4.Bhat SS, Sargod S, Mohammed SV. Taurodontism in deciduous molars: A case report. J Indian Soc Pedod Prev Dent. 2004;22:193–6. [PubMed] [Google Scholar]
- 5.Tomona N, Smith AC, Guadagnini JP, Hart TC. Craniofacial and dental phenotype of Smith-Magenis syndrome. Am J Med Genet A. 2006;140:2556–61. doi: 10.1002/ajmg.a.31371. [DOI] [PubMed] [Google Scholar]
- 6.Axelsson S, Bjornland T, Kjaer I, Heiberg A, Storhaug K. Dental characteristics in Williams syndrome: A clinical and radiographic evaluation. Acta Odontol Scand. 2003;61:129–36. doi: 10.1080/00016350310001451. [DOI] [PubMed] [Google Scholar]
- 7.Akintoye SO, Lee JS, Feimster T, Booher S, Brahim J, Kingman A, et al. Dental characteristics of fibrous dysplasia and McCune-Albright syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:275–82. doi: 10.1016/s1079-2104(03)00225-7. [DOI] [PubMed] [Google Scholar]
- 8.Nawa H, Oberoi S, Vargervik K. Taurodontism and Van der Woude syndrome. Is there an association? Angle Orthod. 2008;78:832–7. doi: 10.2319/081707-384.1. [DOI] [PubMed] [Google Scholar]
- 9.Balis S. Error and accuracy rates of panoramic radiography as a screening method for mass surveying of children. J Public Health Dent. 1981;41:220–34. doi: 10.1111/j.1752-7325.1981.tb01092.x. [DOI] [PubMed] [Google Scholar]
- 10.Shaw JC. Taurodont teeth in South African races. J Anat. 1928;62:476–98. [PMC free article] [PubMed] [Google Scholar]
- 11.Keene HJ. A morphologic and biometric study of taurodontism in a contemporary population. Am J Phys Anthropol. 1966;25:208–9. [Google Scholar]
- 12.Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Commun Dent Oral Epidemiol. 1978;6:200–3. doi: 10.1111/j.1600-0528.1978.tb01150.x. [DOI] [PubMed] [Google Scholar]
- 13.Adloff P. Die Zaähne des Homo primigenius von Krapina. Anat Anz. 1907;31:273–82. [Google Scholar]
- 14.Gorjanovic-Kramberger K. Die Kronen und Wurzeln der Mahlza¨hne des Homo primigenius und ihre genetische Bedeutung. Anat Anz. 1907;31:97–38. [Google Scholar]
- 15.Gorjanovic-Kramberger D. ber prismatische Molarwurzeln rezenter und diuvialer Menschen. Anat Anz. 1908;32:401–13. [Google Scholar]
- 16.Joseph M. Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefilter syndrome: A review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:670–7. doi: 10.1016/j.tripleo.2007.11.015. [DOI] [PubMed] [Google Scholar]
- 17.MacDonald-Jankowski DS, Li TT. Taurodontism in a young adult Chinese population. Dentomaxillofac Radiol. 1993;22:140–4. doi: 10.1259/dmfr.22.3.8299833. [DOI] [PubMed] [Google Scholar]
- 18.Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. J Oral Sci. 2011;53:231–8. doi: 10.2334/josnusd.53.231. [DOI] [PubMed] [Google Scholar]
- 19.Uslu O, Akcam MO, Evirgen S, Cebeci I. Prevalence of dental anomalies in various malocclusions. Am J Orthod Dentofacial Orthop. 2009;135:328–35. doi: 10.1016/j.ajodo.2007.03.030. [DOI] [PubMed] [Google Scholar]
- 20.Darwazeh AM, Hamasha AA, Pillai K. Prevalence of taurodontism in Jordanian dental patients. Dentomaxillofac Radiol. 1998;27:163–5. doi: 10.1038/sj/dmfr/4600342. [DOI] [PubMed] [Google Scholar]
- 21.Bürklein S, Breuer D, Schäfer E. Prevalence of taurodont and pyramidal molars in a German population. J Endod. 2011;37:158–62. doi: 10.1016/j.joen.2010.10.010. [DOI] [PubMed] [Google Scholar]
- 22.Sanderink GC. Imaging characteristics in rotational panoramic radiography. Dentomaxillofac Radiol Suppl. 1987;9:1–213. [PubMed] [Google Scholar]
- 23.Tulensalo T, Ranta R, Kataja M. Reliability in estimating taurodontism of permanent molars from orthopantomograms. Community Dent Oral Epidemiol. 2006;17:258–62. doi: 10.1111/j.1600-0528.1989.tb00629.x. [DOI] [PubMed] [Google Scholar]
- 24.Metgud S, Metgud R, Rani K. Management of a patient with a taurodont, single-rooted molars associated with multiple dental anomalies: A spiral computerized tomography evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e81–6. doi: 10.1016/j.tripleo.2009.04.014. [DOI] [PubMed] [Google Scholar]
- 25.Hayashi Y. Endodontic treatment in taurodontism. J Endod. 1994;20:357–8. doi: 10.1016/S0099-2399(06)80100-7. [DOI] [PubMed] [Google Scholar]
- 26.Durr DP, Campos CA, Ayers CS. Clinical significance of taurodontism. J Am Dent Asso. 1980;100:378–81. doi: 10.14219/jada.archive.1980.0100. [DOI] [PubMed] [Google Scholar]
- 27.Yeh SC, Hsu TY. Endodontic treatment in taurodontism with Klinefelter's syndrome: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:612–5. doi: 10.1016/s1079-2104(99)70094-6. [DOI] [PubMed] [Google Scholar]
- 28.Prakash R, Vishnu C, Suma B, Velmurugan N, Kandaswamy D. Endodontic management of taurodontic teeth. Indian J Dent Res. 2005;16:177–81. doi: 10.4103/0970-9290.29900. [DOI] [PubMed] [Google Scholar]
- 29.Grossman LI, Meiman BW. Solution of pulp tissue by chemical agents. J Am Dent Assoc. 1941;28:223–5. [Google Scholar]
- 30.Moorer WR, Wesselink PR. 110th year Nederlands Tijdschrift voor Tandheelkunde. 2. Root canal treatment, intra-canal disinfectants and bacterial culture: Past and present. Ned Tijdschr Tandheelkd. 2003;110:178–80. [PubMed] [Google Scholar]
- 31.Bharti R, Chandra A, Tikku AP, Wadhwani KK. “Taurodontism” an endodontic challenge: A case report. J Oral Sci. 2009;51:471–4. doi: 10.2334/josnusd.51.471. [DOI] [PubMed] [Google Scholar]